Significant AI Trends for the Financial Industry in 2024 and How to Utilize Them
South African Partner Application
1. Nutrition Empowe (Pty) Ltd
ers Reg. Number. 2008/004479/07
P.O.Box 4607, Edenvale. 16
610, E-mail: info@n-powa.org
Gauteng. South Africa. Website: www.n-powa.org
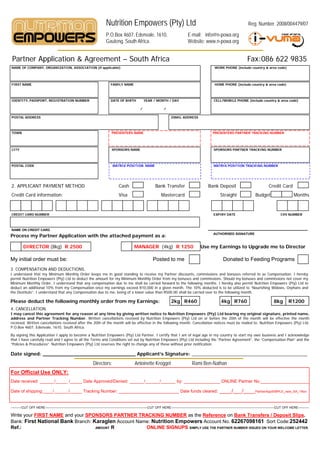
Partner Application & Agreement – South Afr
rica Fax:086 622 9835
NAME OF COMPANY, ORGANIZATION, ASSOCIATION (if applicable) WORK PHONE (include country & area code)
FIRST NAME FAMILY NAME HOME PHONE (include country & area code)
IDENTITY, PASSPORT, REGISTRATION NUMBER DATE OF BIRTH YEAR / MO
ONTH / DAY CELL/MOBILE PHONE (include country & area code)
/ /
POSTAL ADDRESS EMAIL ADDRESS
TOWN PRESENTERS NAME PRESENTERS PARTNER TRACKING NUMBER
Nutrition Empowers 123400
CITY SPONSORS NAME SPONSORS PARTNER TRACKING NUMBER
POSTAL CODE MATRIX POSITION NAME MATRIX POSITION TRACKING NUMBER
2. APPLICANT PAYMENT METHOD Cash Ba Transfer
ank Bank Deposit Credit Card
Credit Card information: Visa Mastercard Straight Budget Months
CREDIT CARD NUMBER EXPIRY DATE CVV NUMBER
NAME ON CREDIT CARD
Process my Partner Application with the attached payment as a:
s AUTHORISED SIGNATURE
DIRECTOR (8kg) R 2500 MANAGER (4kg) R 1250 Use my Earnings to Upgrade me to Director
My initial order must be: Pos
sted to me Donated to Feeding Programs
3. COMPENSATION AND DEDUCTIONS.
I understand that my Minimum Monthly Order keeps me in good standing to receive m Partner discounts, commissions and bonuses referred to as Compensation. I hereby
my
permit Nutrition Empowers (Pty) Ltd to deduct the amount for my Minimum Monthly Orde from my bonuses and commissions. Should my bonuses and commissions not cover my
er
Minimum Monthly Order, I understand that any compensation due to me shall be carried f d forward to the f
following months. I hereby also permit Nutrition Empowers (Pty) Ltd to
deduct an additional 10% from my Compensation once my earnings exceed R10,000 in a given month. The 10% deducted is to be utilized to “Nourishing Widows, Orphans and
the Destitute”. I understand that any Compensation due to me, being of a lower value tha R500.00 shall be carried over to the following month.
an
Please deduct the following monthly order from my Earnings: 2kg R460 4kg R760 8kg R1200
4. CANCELLATION.
I may cancel this agreement for any reason at any time by giving written notice to Nutrition Empowers (Pty) Ltd bearing my original signature, printed name,
e
address and Partner Tracking Number. Written cancellations received by Nutrition Empowers (Pty) Ltd on or before the 20th of the month will be effective the month
n
received. Written cancellations received after the 20th of the month will be effective in the following month. Cancellation notices must be mailed to: Nutrition Empowers (Pty) Ltd.
P.O.Box 4607, Edenvale, 1610, South Africa.
By signing this Application I apply to become a Nutrition Empowers (Pty) Ltd Partner. I c
y g g pp pp y p ( y) certify that I am of legal age in my country to start my own business and I acknowledge
y g g y y y g
that I have carefully read and I agree to all the Terms and Conditions set out by Nutrition Empowers (Pty) Ltd including the “Partner Agreement”, the “Compensation Plan” and the
“Policies & Procedures”. Nutrition Empowers (Pty) Ltd reserves the right to change any of these without prior notification.
Date signed: ______________________________ Applicant’s Signature: ____________________________________________
Directors: Antoinette Kr
roggel Rami Ben-Nathan
For Official Use ONLY:
Date received: ______/_____ /_____ Date Approved/Denied: ______/______/
/______ by: _______________ ONLINE Partner No.____________________
Date of shipping: ________ Date funds cleared:
shipping:____/______/_____ Tracking Number: __________________
/ / ____/___/____PartnerAppSIMPLE new SA 1Nov
/ / PartnerAppSIMPLE_new_SA_1Nov
----------CUT OFF HERE-----------------------------------------------------------------------------------------------CUT OFF HERE------------------------------------------------------------------------------------------------CUT OFF HERE----------
F
Write your FIRST NAME and your SPONSORS PARTNER TRACKING NUMBER as the Reference on Bank Transfers / Deposit Slips.
Bank: First National Bank Branch: Karaglen Account Name: Nut
trition Empowers Account No. 62267098161 Sort Code:252442
Ref.: AMOUNT R ONLIN SIGNUPS SIMPLY USE THE PARTNER NUMBER ISSUED ON YOUR WELCOME LETTER.
NE