
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (11)
Similaire à Alberta Diabetes Surveillance System (ADSS) - Diabetes Atlas: Diabetes in First Nations
Similaire à Alberta Diabetes Surveillance System (ADSS) - Diabetes Atlas: Diabetes in First Nations (20)
Plus de Kelli Buckreus
Plus de Kelli Buckreus (18)
Alberta Diabetes Surveillance System (ADSS) - Diabetes Atlas: Diabetes in First Nations
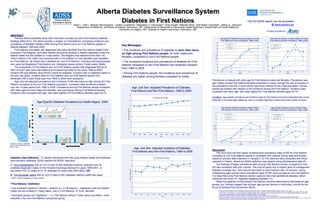
- 1. 0 5 10 15 20 25 30 20-34 35-49 50-64 65-74 75+ Age Group Rateper1000 Non-First Nations - 1995 First Nations - 1995 Non-First Nations - 2004 First Nations - 2004 Alberta Diabetes Surveillance SystemAlberta Diabetes Surveillance System Diabetes in First NationsDiabetes in First Nations Ellen L. Toth1*, Brenda Hemmelgarn2, Lynden Crowshoe3, Stephanie U. Vermeulen4, Greg Hugel4, Malcolm King1, Kelli Ralph-Campbell1, Jeffrey A. Johnson4, Department of Medicine, University of Alberta, Edmonton, AB1, Department of Medicine & Community Health Sciences2, Department of Family Medicine, University of Calgary, AB3, Institute of Health Economics, Edmonton, AB4 The full ADSS report can be accessed @ www.achord.ca ABSTRACTABSTRACT The first Alberta Diabetes Atlas 2007 has been compiled as part of the Alberta Diabetes Strategy 2003-2013. The Atlas includes a chapter on First Nations, comparing incidence and prevalence of diabetes mellitus (DM) among First Nations and non-First Nations people in Alberta between 1995 and 2005. First Nations individuals with diagnosed DM were identified from the Alberta Health Care Insurance Plan Registry, and were defined as anyone residing in Alberta registered under the federal Indian Act and entitled to Treaty status. The Registry was searched from April 1st, 1993 to March 31st, 2005. Any individual with a First Nations or Inuit identifier was classified as “First Nations”; all others were classified as “non-First Nations”, including Aboriginal people who were not Registered First Nations (ex. Aboriginal people without Treaty status, Métis). The proportions of First Nations and non-First Nations people with diagnosed DM as of April 1st each year were calculated and compared annually for the years 1995 to 2005. Incident DM was defined using NDSS criteria for diabetes: a person with no diabetes claims in the prior two years. Incident rates for First Nations and non-First Nations people who developed DM in each fiscal year from 1995 to 2004 were compared. Age- and sex-adjusted prevalence and incidence of DM was twice as high among the First Nations compared to the non-First Nations population. Increased rates remained constant over the 10-year period from 1995 to 2005. Prevalence among First Nations people increased with older ages for both males and females, and was higher among First Nations females. Incidence also increased with age, with rates highest for First Nations females aged 50-74. Diabetes Case Definition.Diabetes Case Definition. To identify individuals with DM using Alberta Health and Wellness administrative database, ADSS applied the NDSS* algorithm: A. One hospitalization with an ICD-9 code of 250 (diabetes mellitus), selected from all available diagnostic codes on the Hospital Discharge Abstract for years 1995-2001, or equivalent ICD-10 codes (E10-14, diabetes) for years after 2001/2002; OR, B. Two physician claims with an ICD-9 code of 250 (diabetes mellitus) within two years. Key Messages:Key Messages: • The incidence and prevalence of diabetes is more than twice as high among First Nations people, for both males and females, compared to non-First Nations people. • The increased incidence and prevalence of diabetes for First Nations compared to non-First Nations has remained constant from 1995 to 2005. • Among First Nations people, the incidence and prevalence of diabetes are higher among females compared to males. AgeAge--Specific Diabetes Prevalence by Health Region, 2005Specific Diabetes Prevalence by Health Region, 2005 Population of Alberta: 3,275,376 (source: Population Registry File, March 31/06) * NDSS = National Diabetes Surveillance System AgeAge-- and Sexand Sex-- Adjusted Prevalence of Diabetes,Adjusted Prevalence of Diabetes, First Nations and NonFirst Nations and Non--First Nations, 1995 to 2005First Nations, 1995 to 2005 ““First NationsFirst Nations”” Definition:Definition: • Any individual residing in Alberta – whether on- or off-reserve – registered under the federal Indian Act and entitled to Treaty status, with a “First Nations” or “Inuit” identifier. • Aboriginal people not “registered” – i.e. First Nations without Treaty status and Métis – were included in the non-First Nations comparison group. AgeAge-- and Sexand Sex-- Adjusted Incidence of Diabetes,Adjusted Incidence of Diabetes, First Nations and NonFirst Nations and Non--First Nations, 1995 to 2005First Nations, 1995 to 2005 DiscussionDiscussion The more than two-fold higher incidence and prevalence rates of DM for First Nations compared to non-First Nations people is consistent with national survey data and studies based on primary data collection in Canada.(1-5) The rates are also consistent with those reported in Ontario, where the NDSS definition was applied using administrative data.(6) Our findings of higher prevalence rates among First Nations women compared to men are also consistent with prior reports. This may be partly due to higher rates of undiagnosed diabetes amongst men, who may be less likely to seek medical care. Of concern, young childbearing aged women show prevalence rates of DM twice as high as non-First Nations. It is likely that some First Nations women captured here had gestational diabetes, which reinforces the notion of “diabetes begetting diabetes”.(7) While the epidemic of DM among First Nations requires interventions that target all age groups, our findings suggest that younger age groups (women in particular), should be the focus of treatment and prevention efforts. Prevalence increased with older age for First Nations males and females. Prevalence was also higher among First Nations females compared to males, though the rate of increase in the prevalence over the 10-year period was more marked for the male population. Similar results are evident with respect to the incidence among the First Nations. Incidence also increased with older age, with rates highest for First Nations females aged 50-74. [Limitation: Age-specific prevalence and incidence rates for First Nations should be interpreted with caution, especially in the oldest age categories, due to unreliable reporting of deaths and small number of cases. AgeAge--Specific Diabetes Prevalence Rates of FemaleSpecific Diabetes Prevalence Rates of Female First Nations and NonFirst Nations and Non--First Nations, 1995 to 2005First Nations, 1995 to 2005 AgeAge--Specific Diabetes Incidence Rates of FemaleSpecific Diabetes Incidence Rates of Female First Nations and NonFirst Nations and Non--First Nations, 1995 to 2005First Nations, 1995 to 2005 AgeAge--Specific Diabetes Prevalence Rates of MaleSpecific Diabetes Prevalence Rates of Male First Nations and NonFirst Nations and Non--First Nations, 1995 to 2005First Nations, 1995 to 2005 AgeAge--Specific Diabetes Incidence Rates of MaleSpecific Diabetes Incidence Rates of Male First Nations and NonFirst Nations and Non--First Nations, 1995 to 2005First Nations, 1995 to 2005 1. Dean HJ, Mundy RL, Moffatt M: Non-insulin-dependent diabetes mellitus in Indian children in Manitoba. Canadian Medical Association Journal 147:52-57, 1992. 2. Dannenbaum D, Verronneau M, Torrie J: Comprehensive computerized diabetes registry - Serving the Cree of Eeyou Istchee (eastern James Bay). Canadian Family Physician 45:364-370, 1999. 3. Hux, J., Booth, G., and Laupacis, A. The ICES Practice Atlas: Diabetes in Ontario. 2002. Institute for Clinical Evaluative Sciences (ICES), and the Canadian Diabetes Association. Available from: www.ices.on.ca/webpage.cfm?site_id=1&org_id=67&morg_id=0&gsec_id=0&item_id=1312&type=atlas 4. Pollex RL, Khan HM, Connelly PW, Young TK, Hegele RA: The metabolic syndrome in Inuit. Diabetes Care 27:1517-1518, 2004. 5. Young TK: Contributions to chronic disease prevention and control: studies among the Kivalliq Inuit since 1990. International Journal of Circumpolar Health 62:323-330, 2003. 6. Mohamed N, Dooley J: Gestational diabetes and subsequent development of NIDDM in aboriginal women of northwestern Ontario. International Journal of Circumpolar Health 57 Suppl 1:355-358, 1998. 7. Godfrey KM, Barker DJ: Fetal programming and adult health. Public Health Nutrition 4:611-624, 2001 0 2 4 6 8 10 12 14 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 Year Rateper100age20+ Non-First Nations First Nations 0 2 4 6 8 10 12 14 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 Year Rateper1000age20+ Non-First Nations First Nations 0 5 10 15 20 25 30 35 40 45 20-34 35-49 50-64 65-74 75+ Age Group Rateper100 First Nations - 1995 Non-First Nations - 1995 First Nations - 2005 Non-First Nations - 2005 0 5 10 15 20 25 30 20-34 35-49 50-64 65-74 75+ Age Group Rateper1000 Non-First Nations - 1995 First Nations - 1995 Non-First Nations - 2004 First Nations - 2004 0 5 10 15 20 25 30 35 40 45 20-34 35-49 50-64 65-74 75+ Age Group Rateper100 First Nations - 1995 Non-First Nations - 1995 First Nations - 2005 Non-First Nations - 2005 Funding provided by: