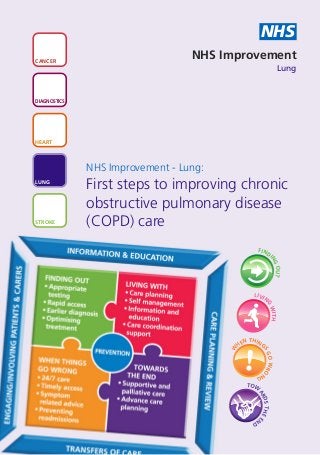
First steps to improving chronic obstructive pulmonary disease (COPD) care
•
1 j'aime•598 vues

A basic guide to the key principles every area should be adopting to provide good COPD care – if you do nothing else, start with these ten things and make sure they are in place for all your patients. This may be a helpful starting point for those new to commissioning for COPD services or for a stocktake for a local respiratory team. (October 2012)

Recommandé
Recommandé
Contenu connexe
Plus de NHS Improvement
Plus de NHS Improvement (20)
Dernier
Dernier (20)
First steps to improving chronic obstructive pulmonary disease (COPD) care
- 1. NHS CANCER NHS Improvement Lung DIAGNOSTICS HEART NHS Improvement - Lung: LUNG First steps to improving chronic obstructive pulmonary disease STROKE (COPD) care FIND I NG OUT LIVI N G WITH N THING HE W SG ! O WRO NG TO W AR DS THE E ND
- 2. FIND First steps to improving chronic obstructive pulmonary disease (COPD) care I NG O UT What you can do Why it matters How to do it 1. Identify, Many people are diagnosed with • Audit practice information diagnose and COPD late in the disease systems to identify people intervene progression. If we can diagnose who receive multiple early and intervene earlier we can prescriptions for oral steroids better manage the impact on and/or antibiotics. patients and the burden of • Consider which patients disease. Studies have shown should be assessed for COPD that in the two to ten years prior or other conditions so that to diagnosis, people are likely to you can start them on the have consulted in primary care appropriate treatment pathway. on multiple occasions for lower • Discuss with patients what respiratory complaints and lower the disease is, and what they respiratory tract infections, and can do, including advice to have received multiple about smoking and exercise. prescriptions for oral steroids • Back this up with written and/or antibiotics. This suggests information for the patient, there is scope for earlier but do not rely on leaflets assessment and diagnosis. alone. 2. No Misdiagnosis is very common • Check practice registers – all diagnosis and means patients are not on COPD diagnoses should have without optimal treatment. This wastes spirometry undertaken and quality medicines, time and money and recorded within the last 15 means that the patient’s months. assured condition may not be effectively • Review those with dual spirometry managed. diagnosis of COPD and asthma. Spirometry is an essential • Train staff in undertaking component of accurate quality assured spirometry diagnosis, but must be and ensure only appropriately performed correctly, according trained people undertake and to existing guidelines, and interpret results. interpreted accurately to be • Calibrate your spirometer. valid. • Ensure you have a local pathway for referral to your Spirometry is not the only specialist services for diagnostic test that should be additional tests when there is undertaken for a correct diagnostic doubt. diagnosis – other tests may be needed such as CT scan. 2
- 3. LIVIN First steps to improving chronic obstructive pulmonary disease (COPD) care G WIT H What you can do Why it matters How to do it 3. Talk with Patients live with their condition • At diagnosis and review, plan to patients every day and understand what spend more time with patients about self they can do to manage its ensuring they understand the management impact on their life, the less condition and what they can to reliant they will be on health do to improve life with it. services. Self management is • Refer appropriate patients to not just about developing an pulmonary rehabilitation which action plan, but about the supports effective self management. process of planning and • Look at how much time is understanding the requirements currently spent in primary care and aspirations of the patient. seeing people with COPD and co-morbidities in the course of Take time to understand their the year. Consider whether you motivation, aspirations, fears can organise care to provide a and behaviour to help initiate care planning appointment to change. address a number of concerns and proactive intervention up front. This needs to be 30 minutes plus but may save time over the course of the year. 4. Check Poor inhaler technique is • Make inhaler technique checks inhaler extremely common and part of every review. technique at substantially reduces the • Take time with patients to every effectiveness of the inhaled understand how they actually use drug. If staff do not their medication and why, and opportunity demonstrate technique correctly what you can do to help them. and check regularly, patients are • Ensure all staff have regular unlikely to use their devices updates in use of devices and effectively or get maximum demonstration of inhaler potential benefit from their technique. medication. If medicines appear • Use trainer devices for an not to be working, patients may objective assessment and to be prescribed additional help patients acquire and medication that could be maintain optimum technique. avoided and which could even • Work with your local be harmful. pharmacists who can perform inhaler technique checks as part of medicines use reviews, to enhance impact. 3
- 4. LIVIN First steps to improving chronic obstructive pulmonary disease (COPD) care G WIT H What you can do Why it matters How to do it 5. Help Patients who understand their • Ensure all appropriate patients patients to own symptoms, recognise have rescue medication and recognise and changes and respond understand how and when to respond to accordingly by starting use it. medication and seeking advice • Ensure patients have a contact exacerbations early can manage exacerbations number for advice if they are more effectively. uncertain what to do. If they don’t, they will revert to A&E or This can reduce demand for urgent appointments. urgent appointments, A&E • Ensure all patients are followed attendance and admissions. up after admission – acute units can advise primary care of admissions/discharges and follow up arrangements. • Record exacerbations in primary care so that you can identify patients whose condition and treatment may need review. 6. Review People with severe COPD are • Ensure you are assessing and people often not reviewed frequently recording disease severity according to enough. This can lead to poor accurately and consistently. their disease management and more • Check that patients are on the frequent exacerbations. appropriate treatment severity in a pathway for the severity of timely manner their disease. Treatment choice depends on symptoms as well as FEV1 (NICE guidelines 2010). • Check that patients who are eligible have been referred for pulmonary rehabilitation and are offered support to stop smoking as these are effective interventions for COPD. 4
- 5. LIVIN First steps to improving chronic obstructive pulmonary disease (COPD) care G WIT H What you can do Why it matters How to do it 7. Do not Home oxygen is a treatment for Promote the message to staff prescribe chronic hypoxaemia and NOT a and patients that ‘oxygen is not oxygen for treatment for breathlessness. It a treatment for breathlessness’ ‘breathlessness’ is a drug and should only be and that there are often more prescribed where clinically appropriate ways to manage and ensure indicated otherwise it is of NO breathless patients. prescribing benefit and potentially harmful remains to some patients. Ensure only patients who have clinically been assessed by a specialist appropriate In PCTs that have introduced a service are prescribed oxygen and and cost review of their oxygen registers that they receive ongoing review. effective coupled with the introduction of This involves measuring both through a formal assessment service up oxygen saturations and blood formal to £400,000 has been saved in gases and reviewing other clinical one year. If the scale of savings data together with supplier data assessment were replicated across England, on usage, flow rate, duration and ongoing it is estimated that they could and equipment. review amount to between £10-20m. Rationalise therapy in line with clinical need and undertake supported withdrawal of oxygen providing no clinical benefit. 8. Oxygen Some patients with COPD or Oxygen alert cards and 24% alert cards other long term chest conditions masks (recommended in the should be can become sensitive to medium BTS 2008 guideline) can avoid provided for or high doses of oxygen. This hypercapnic respiratory failure does not happen to everyone by alerting healthcare at risk with these conditions, only a professionals that patients are patients small number, therefore, if sensitive to oxygen. Oxygen oxygen is needed by these alert cards should be issued patients, it should be given in a to all at risk patients on controlled way and monitored discharge as part of the carefully. discharge planning process. 5
- 6. N THING First steps to improving chronic obstructive pulmonary disease (COPD) care HE S W ! G N GO WRO What you can do Why it matters How to do it 9. Specialist Early senior review can reduce Identify how many people are review for length of stay and prevent not on the respiratory pathway / every patient avoidable admission. Only 53% respiratory ward or do not admitted for of patients are looked after by a receive specialist care. respiratory physician during their COPD inpatient stay. Demand and capacity analysis can exacerbation help identify how you can reduce within 24 the time until specialist review hours occurs. Look at processes for patient assessment, review and discharge planning. 6
- 7. G TO W First steps to improving chronic obstructive pulmonary disease (COPD) care A RD ND S THE E What you can do Why it matters How to do it 10. Discuss COPD is a terminal illness, but • Discuss end of life care needs end of life care progression and deterioration is with appropriate COPD needs with often unpredictable due to patients appropriate disease trajectory. • Give timely information and offer the opportunity to COPD patients Proactive approaches are patients to decide how they and ensure important to ensure that want their care to be they are patients, carers and professionals delivered at end of life included on are prepared for end of life and • Raise the topic with patients end of life that informed choices are made. during a period of wellness as registers opposed to an acute care setting following an acute exacerbation • Ensure COPD patients are included on end of life registers. Prognostic indicators e.g. GSF should be used in primary care to regularly assess COPD patients to determine eligibility for being added to the end of life care register. Typically, COPD patients should make up around 14% of the care registers. 7
- 8. NHS CANCER NHS Improvement DIAGNOSTICS NHS Improvement HEART NHS Improvement’s strength and expertise lies in practical service improvement. It has over a decade of experience in clinical patient pathway redesign in cancer, diagnostics, heart, lung and stroke and demonstrates some of the most leading edge improvement work in LUNG England which supports improved patient experience and outcomes. Working closely with the Department of Health, trusts, clinical networks, other health sector partners, professional bodies and charities, over the past year it has tested, implemented, sustained and spread quantifiable improvements with over 250 sites across the country as well as providing STROKE an improvement tool to over 2,000 GP practices. NHS Improvement 3rd Floor | St John’s House | East Street | Leicester | LE1 6NB Telephone: 0116 222 5184 | Fax: 0116 222 5101 www.improvement.nhs.uk Publication Ref: IMP/LUNG0003 - August 2012 ©NHS Improvement 2012 | All Rights Reserved Delivering tomorrow’s improvement agenda for the NHS