1. Anaemia
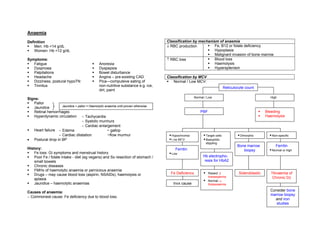
Definition Classification by mechanism of anaemia
Men: Hb <14 g/dL ↓ RBC production Fe, B12 or folate deficiency
Women: Hb <12 g/dL Hypoplasia
Malignant invasion of bone marrow
Symptoms: ↑ RBC loss Blood loss
Fatigue Anorexia Haemolysis
Dyspnoea Dyspepsia Hypersplenism
Palpitations Bowel disturbance
Headache Angina – pre-existing CAD Classification by MCV
Dizziness, postural hypoTN Pica—compulsive eating of Normal / Low MCV:
Tinnitus non-nutritive substance e.g. ice,
Reticulocyte count
dirt, paint
Normal / Low High
Signs:
Pallor
Jaundice + pallor = Haemolytic anaemia until proven otherwise
Jaundice
Retinal hemorrhages PBF Bleeding
Hyperdynamic circulation ∼ Tachycardia Haemolysis
∼ Systolic murmurs
∼ Cardiac enlargement
Heart failure ∼ Edema ~ gallop
∼ Cardiac dilatation ~flow murmur Hypochromia Target cells Dimorphic Non-specific
• Postural drop in BP Low MCV Basophilic
stippling
Bone marrow Ferritin
History: Ferritin biopsy Normal or high
Fe loss: GI symptoms and menstrual history. Low
Poor Fe / folate intake - diet (eg vegans) and Sx resection of stomach / Hb electropho-
small bowels resis for HbA2
Chronic diseases
FMHx of haemolytic anaemia or pernicious anaemia
Fe Deficiency Raised: β Sideroblastic ?Anaemia of
Drugs – may cause blood loss (aspirin, NSAIDs), haemolysis or
thalassaemia Chronic Dz
aplasia Normal: α
Jaundice – haemolytic anaemias Invx cause thalassaemia
Causes of anaemia: Consider bone
marrow biopsy
∼ Commonest cause: Fe deficiency due to blood loss.
and iron
studies
2. High MCV Low MCV Fe deficiency (commonest Thalassaemia
cause) Sideroblastic anaemia (rare)
Check Hx: Normal MCV Haemolysis Bone marrow failure
EtOH Anaemia of Chronic Dz Renal failure
Liver dz Pregnancy Hypothyroidism
FMHx pernicious anaemia High MCV B12 / folate deficiency Reticulocytosis eg haemolysis
Hypothyroid Antifolate drugs eg phenytoin Myelodysplastic syndromes
Drugs Alcohol Marrow infiltration
Prev. abdo Sx Liver disease Cytotoxics
Hypothyroidism
*Haemolytic anaemias may be normo- or macro-cytic. Suspect if
reticulocytosis is present
PBF + Reticulocyte count
Investigations – Anaemia workup:
• FBC • U/E/Cr
Hypersegmented polymorphs Drugs/cytotoxics • Reticulocyte count • LFT – liver dz & ↑LDH in haemolytic anaemia
• PBF • TFT
• Fe / TIBC / Ferritin • Fecal occult blood
• Folate + B12 • Direct Coomb’s test – Haemolytic anaemias
Folate, B12 levels Low Invx & treat • Hb electrophoresis • ± OGD for UGI bleed/colonoscopy for LGIB
• ±Bone marrow biopsy
Target cells, stomatocytes LFT
Interpreting Plasma Iron Studies
Iron TIBC Ferritin
Dysplasia / cytopenia ?Myelodysplasia Fe deficiency ↓ ↑ ↓
Marrow Anaemia of Chronic dz ↓ ↓ ↑
Chronic haemolysis ↑ ↓ ↑
Dimorphic ?Sideroblastic Haemchromatosis ↑ ↓/N ↑
Pregnancy ↑ ↑ N
Sideroblastic anaemia ↑ N ↑
Polychromasia / High Retic count
?Bleeding ↑ Bilirubin & LDH
Haemolytic anaemias
- look for fragments
3. Iron Deficiency Anaemia Sideroblastic Anaemia
Causes: 1. menorrhagia 6. diverticulitis Dyserythropoiesis + iron loading (bone marrow + haemosiderosis ie
2. oesophagitis haemorrhoids endocrine, liver and cardiac damage)
3. PUD 7. hookworms Causes: Idiopathic, Congenital (rare, X-linked), EtOH or lead excess,
4. GI CA 8. poor diet / special diet myeloproliferative disease, malignancy, malabsorption, anti-TB drugs
5. colitis 9. malabsorption (celiac dz) Hypochromic RBC on PBF + sideroblasts in marrow.
Rx: Oral iron (eg Fe sulfate 200mg/12-8h PO) – should
increase Hb by 1 g/dl/week. SE: constipation, black stools
Haemolytic Anaemias
Causes:
Membrane problems Hereditary spherocytosis
Elliptocytosis
Enzyme problems G6PD deficiency
Pyruvate kinase deficiency
Hb problems Thalassaemia
Sickle cell disease
Others Infection: Malaria, HUS
Hypersplenism
Mechanical heart valves
Autoimmune Ab (AIHAs)
Snake venom
Investigations
↓ Hb ↑ Unconjugated Bilirubin
↑ LDH ↑ Reticulocyte count
↓ haptoglobulin DCT: + in AIHA
Anaemia of Chronic Disease
Causes: Infection, collagen vascular dz, rheumatoid arthritis,
malignancy, renal failure
Rx: treat underlying cause. Recombinant erythropoietin for renal
Digitally signed by DR WANA HLA SHWE
failure DN: cn=DR WANA HLA SHWE, c=MY, o=UCSI University,
School of Medicine, KT-Campus, Terengganu, ou=Internal
Medicine Group, email=wunna.hlashwe@gmail.com
Reason: This document is for UCSI University, School of
Medicine students.
Date: 2009.03.08 09:31:58 +08'00'