1. Approach to Proteinuria KIV Urine phase contrast & U/S kidneys as indicated
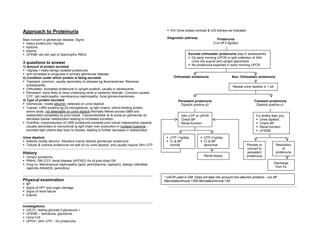
Diagnostic pathway
Main concern is glomerular disease. Signs: Proteinuria
heavy proteinuria >3g/day (Cut off 0.5g/day)
lipiduria
edema
UFEME red cell cast or dysmorphic RBCs Exclude orthostatic proteinuria (esp in adolescents)
Do early morning UPCR or split collection of 24hr
3 questions to answer urine into supine and upright specimens
No proteinuria expected in early morning UPCR
1) Amount of protein excreted
<2g/day = likely benign isolated proteinuria
amt correlates to prognosis in primary glomerular disease
2) Condition under which protein is being excreted Orthostatic proteinuria Non- Orthostatic proteinuria
Transient: common, usually secondary to stresses eg fever/exercise. Resolves
subsequently Repeat urine dipstick in 1 wk
Orthostatic: increased proteinuria in upright position, usually in adolescents.
Persistent: more likely to have underlying renal or systemic disorder. Common causes:
CCF, IgA nephropathy, membranous nephropathy, focal glomerulosclerosis
3) Type of protein excreted Persistent proteinuria Transient proteinuria
Glomerular: mostly albumin, detected on urine dipstick Dipstick positive x2 Dipstick positive x1
Tubular: LMW proteins eg β2-microglobulin, Ig light chains, retinol-binding protein,
amino acids, not detectable on urine dipstick.Normally filtered across GBM and
reabsorbed completely by prox tubule. Tubulointerstitial dz & some pri glomerular dz 24hr UTP or UPCR F/u 6mths then yrly:
decrease tubular reabsorption leading to increased excretion. Check BP Urine dipstick
Overflow: overproduction of LMW proteinuria exceeds prox tubule reabsorptive capacity. Renal function Check BP
Usually secondary to monoclonal Ig light chain over production in multiple myeloma – Renal function
excreted light chains also toxic to tubules, leading to further decrease in reabsorption UFEME
Urine dipstick: UTP <1g/day UTP ≥1g/day
Detects mostly albumin, therefore mainly detects glomerular proteinuria. Cr & BP Cr & BP
Tubular & overlow proteinuria not well dx by urine dipstick, and usually require 24hr UTP normal abnormal Persists or Resolution
convert to of
History persistent proteinuria
Urinary symptoms Renal biopsy proteinuria
PMHX: DM /CCF /renal disease (APCKD) /hx of post strep GN
Drug hx: Membranous nephropathy (gold, penicillamine, captopril), allergic interstitial Discharge
nephritis (NSAIDS, penicillins) from f/u
* UACR used in DM. Does not take into account non-albumin proteins – cut off:
Physical examination Macroalbuminuria >300 Microalbuminuria >30
BP
Signs of HPT end organ damage
Signs of renal failure
Edema
Investigations
U/E/Cr, fasting glucose if glycosuria +
UFEME – hematuria, glycosuria
Urine C/S
UPCR / 24hr UTP – for proteinuria
2. Mx
1) BP control
ACEI in DM type1
ARB in DM type 2
Monitor for RAS: check Cr 2 wks after starting ACEI/ARB. Stop if Cr increase
>20%
2nd line Rx: CCB (verapamil, diltiazem). Avoid beta-blockers w CCB – risk of
heartblock
2) RAS
Suspect if HPT + IHD/LVH + PVD
Invx: MRA / doppler
3) Hyperlipidaemia
statin
4) Decrease smoking
Digitally signed by DR WANA HLA SHWE
DN: cn=DR WANA HLA SHWE, c=MY,
o=UCSI University, School of Medicine, KT-
Campus, Terengganu, ou=Internal Medicine
Group, email=wunna.hlashwe@gmail.com
Reason: This document is for UCSI year 4
students.
Date: 2009.02.24 10:20:51 +08'00'