Inspiring Doable Tech Training for Healthcare
•
1 j'aime•1,923 vues

Basic records management to improve input and output, integration and interoperability in health care systems for providers, systems creators, implementation and managers. Training advice-moving from paper to digital charting systems. Key functions, terms.

Recommandé
Recommandé
Contenu connexe
Similaire à Inspiring Doable Tech Training for Healthcare
Similaire à Inspiring Doable Tech Training for Healthcare (20)
Dernier
Dernier (20)
Inspiring Doable Tech Training for Healthcare
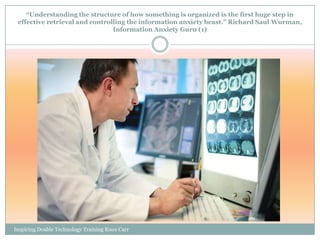
- 1. “Understanding the structure of how something is organized is the first huge step in effective retrieval and controlling the information anxiety beast.” Richard Saul Wurman, Information Anxiety Guru (1) Inspiring Doable Technology Training Knox Carr
- 2. Inspiring, Doable Technology Training, Implementation and Deployment Suggestions for Health Care Organizations © 2009 W. J. KNOX CARR AHE 232, INTRODUCTION TO INFORMATION TECHNOLOGY SYSTEMS IN HEALTHCARE NORTH SEATTLE COMMUNITY COLLEGE SEATTLE, WASHINGTON 9 DECEMBER, 2009
- 3. Data ―› Information ―›Knowledge ―› Wisdom Electronic medical records can facilitate many administrative, clinical, regulatory and management functions in health care organizations. With them, we can provide better care, make better decisions and communicate with more people with greater clarity, speed and efficiency. Inspiring Doable Technology Training Knox Carr
- 4. Medical records in the U.S. have been federally mandated to be available in electronic form (on computers) by 2014. We can do it! Inspiring Doable Technology Training Knox Carr
- 5. We are expected to collect data and input it electronically to create usable and reliable records Data –written, oral, film-becomes a Document, becomes a Record, becomes usable and reliable Information through human and technological procedures and processes.(2) Inspiring Doable Technology Training Knox Carr
- 6. What processes do records go through? Creation Retention Use (Retrieval, Reading, Examination, Communication) Evaluation and Disposition (Deaccession, Storage, Destruction, &c.) We do these steps with all formats of data and records throughout our jobs Inspiring Doable Technology Training Knox Carr
- 7. Why “technology?” Technology is about tools that make Even library card catalogues were work easier for people. ―data bases‖ ― coordinated lists. Inspiring Doable Technology Training Knox Carr
- 8. When computers came along, computer databases made keeping track of books and other formats of materials in libraries much easier to work with than they had been in card catalogues. How about patients and procedures? Inspiring Doable Technology Training Knox Carr
- 9. “Don’t I have enough to do already?” People, both clinical health workers and our clients, are NOT machines! We know what symptoms of ―media overload‖ or ―input overload‖ are in our own lives – and it’s happening to the healthcare system, too.(3) Is a symptom a “problem” in itself, or an indicator of a systemic imbalance that needs attention You know the answer to that and care? question better than anyone! Inspiring Doable Technology Training Knox Carr
- 10. Records Systems, throughout all of their phases, must be RELIABLE, SYSTEMATIC AND COMPREHENSIVE AND MUST HAVE: INTEGRITY AND COMPLIANCE IN ORDER TO BE OF USABLE VALUE. (4) Inspiring Doable Technology Training Knox Carr
- 11. Systems: Working together. You can’t just mend someone’s broken toe (skeletal system) and expect them to be healthy if they have chronic heart disease or other disorders, too. Maybe splinting big toes is what you’re good at, and it helps the patient feel better; but look at the Big Picture, too: Cardiologists, dieticians , physical therapists, nurses, the community and the patient’s family have to work together if HEALTH is really the goal of healthcare! Inspiring Doable Technology Training Knox Carr
- 12. SYSTEMS! We work in big organizations with a lot of functions, or we work in smaller organizations with many interconnected (integrated and interoperable) processes and people… Inspiring Doable Technology Training Knox Carr
- 13. What does THAT mean? Systematics: Verb1. systematise - arrange according to a system or reduce to a system; "systematize our scientific knowledge‖ systematize, systemise, systemize order - bring order to or into; "Order these files" digest - systematize, as by classifying and summarizing; "the government digested the entire law into a code" codify - organize into a code or system, such as a body of law; "Hammurabi codified the laws‖ (5) Inspiring Doable Technology Training Knox Carr
- 14. Data and Record: Creation Retention Use Evaluation And Disposition Happen all the time! Inspiring Doable Technology Training Knox Carr
- 15. We want to keep our jobs, do them well and help the healthcare system work better. The goal of healthcare is health. ―The creation of a culture of safety requires a nonpunitive environment in which errors, near misses, and potential problems can be reported without fear of reprisal,‖ (6) that is, losing our jobs or being demoted financially or within our organizations. Nurses are involved in care at all levels. Sometimes computerized provider order entry (CPOE) feels awkward, especially at first. (7) We are dealing with the ―artificiality of indexing systems… The human mind does not work that way. It operates by association.‖ (8) Inspiring Doable Technology Training Knox Carr
- 16. Our Health Electronic Health Record Information (EHR) mgt & Computerized System is Sick! Provider Order Entry can We need: help get us back on track… Reliable, Systematic and Comprehensive Creation, Retention , Use, Evaluation and Disposition of data with Integrity and Compliance… Inspiring Doable Technology Training Knox Carr
- 17. Information Technology (IT) Training Comprehensive training in electronic health care recordkeeping among clinical (nursing, departmental, medical), information technology, business and administrative staff of healthcare organizations of all sizes and types will have to occur such that required, interoperable recordkeeping systems’ integration, reporting and functionality standards can be met to satisfy federal regulations. (9) Inspiring Doable Technology Training Knox Carr
- 18. ―Despite the advances in technology that make personalisation possible, the challenge for lecturers remains to develop a learning environment that encourages, confronts, and adapts to the personal preferences and needs of the Everyone learns different ways! individual I want to be spending time with my clients, student.‖(10) not in front of a computer!(11) Inspiring Doable Technology Training Knox Carr
- 19. It is important to: Monitor and Evaluate throughout the procedures of: Creating Handling and Preserving records Inspiring Doable Technology Training Knox Carr
- 20. Inspiring Doable Technology Training Knox Carr
- 21. Start small, do your best, ask questions, have technological procedures and systems presented to you in ways you can understand, and MOVE FORWARD That’s the best we can do! as a TEAM: Inspiring Doable Technology Training Knox Carr
- 22. …beginning wherever we are… Inspiring Doable Technology Training Knox Carr
- 23. Inspiring, Doable Technology Training QUESTIONS? COMMENTS? DISCUSSION? BASICS OF HEALTH CARE RECORDS CREATION AND MANAGEMENT IN THE UNITED STATES ON A CLINICAL LEVEL TOWARDS YEAR 2014 FOR PHYSICIANS, MEDICAL TRAINERS, NURSES, SUPERVISORS, IT MANAGERS AND SYSTEM ADMINISTRATORS
- 24. Inspiring, Doable Technology Training Endnotes 1. UBC-SLAIS, Heather MacNeill, Luciana Duranti, Terry Eastwood, Susie Stephenson, Rick Kopak et al. (Instructors); Recordkeeping, Records Management, Archival Diplomatics, Data Base Design et al.; University of British Columbia School of Library, Archives and Information Studies; Vancouver, B. C., 2002 – 2005, as interpreted and recorded by Wyndy J. Knox Carr, MFA, MLIS. 2. UBC-SLAIS, ibid. 3. Campbell EM, Guappone KP, Sittig DF, Dykstra RH, Ash JS, PubMed and Springer fulltext, http://www.springerlink.com/content/e2k000q063j14767/fulltext.ht ml (online), ―Computerized provider order entry adoption: implications for clinical workflow,‖ (accessed 22 November 2009), Department of Medical Informatics and Clinical Epidemiology, Oregon Health & Science University, Portland, OR, J Gen Intern Med. 2009 Jan;24(1):21-6. Epub 2008 Nov 20. 4. UBC-SLAIS, op cit. Inspiring Doable Technology Training Knox Carr
- 25. Endnotes (continued) 5.Farlex Free dictionary, (online), ―systematics, taxonomy‖ http://www.thefreedictionary.com/taxonomy (accessed 22 November, 2009), Based on WordNet 3.0, Farlex clipart collection. 2003-2008 Princeton University, Farlex Inc. 6. Hebda, Toni; and Patricia Czar; Handbook of informatics for nurses & health care professionals, 4th ed., Upper Saddle River, N.J. : Pearson Prentice Hall, c2009, p. 21. 7. Darbyshire P., PubMed, ―'Rage against the machine?': nurses' and midwives' experiences of using Computerized Patient Information Systems for clinical information,‖ (online) http://www.ncbi.nlm.nih.gov/pubmed/14687289 (accessed 22 November 2009), Women's & Children's Hospital, University of South Australia, Adelaide, Australia, J Clin Nurs. 2004 Jan;13(1):17-25.(Comment in: * J Clin Nurs. 2006 Feb;15(2):237. * J Clin Nurs. 2008 Aug;17(15):2090-1). Inspiring Doable Technology Training Knox Carr
- 26. Endnotes (continued) 8. Bush, Vannevar; 1945, How Information is Organized, quoted by Rick Kopak, UBC-SLAIS, in Database Design class handout, op cit., 2005. 9. Abdelhak, Mervat, et al., Health information : management of a strategic resource, 3rd ed., St. Louis, Mo. : Saunders/Elsevier, c2007, Cprs. 1 - 3. 10. Cox, Sharon; ―Introduction- Learning Activities Model—Local Area Networks". Learning Styles in Online Environments, Tomei (ed), Lawrence A., Encyclopedia of Information Technology Curriculum Integration. IGI Global, 2008. (King Co. Libraries online resources), Books24x7. <http://common.books24x7.com/book/id_18674/book.asp> (accessed November 20, 2009). 11. Anonymous retired Ob-Gyn nurse’s report (Swedish Hospitals, Seattle WA) from her friends still on the job. To author present at a meeting, 10 November, 2009. Inspiring Doable Technology Training Knox Carr
Notes de l'éditeur
- What Needs to be Done? Systems Integration and InteroperabilityLarge organizations like metropolitan hospitals, the Veterans’ Administration (VA) and regional managed care or cooperative programs have been working steadily to organize medical records electronically for their own use and to facilitate records management, third-party and government billing, and reporting for public health surveillance since at least 1973 due to advances in personal computing (PC) technology, lowered costs of equipment and software, integration and interoperability of local and wide-area network servers/services and the Internet, and the Health Maintenance Organization Act of that year. The processing of collected data into Electronic Health Records (EHRs) is already occurring in many milieus, but has a long way to go before it will reach the comprehensive quality functionality required to produce results up to standards. According to Millwood in Health Affairs, 2005, (see Appendix 1), only 12% of medical groups in the US had adopted the EHR at that time. Large organizations, particularly those gathering data electronically already, have surely expanded that 12%, but the top to bottom integration of each of these organizations is still coming about, to say nothing of the interoperability of organizations nationally. (Wikipedia, (online), “Managed Care,” http://en.wikipedia.org/wiki/Managed_care (accessed 27 November, 2009). Contributors include Harvard Medical, EWJF, aware.com, California Health Care Foundation, US Dep. HHS-ONC, Digital Preservation Europe, HHRQ, ICMCC et cetera.)
- Why? The Bottom to Top and Back Again Business Case: The Carrot and the StickSmall to medium-sized organizations, however, have been creating and integrating electronic systems as they have been financially and physically able to do so, with many organizations operating with essentially “hybrid” --both paper and electronic-- systems that are neither private nor secure, to say nothing of integrated internally and interoperable externally with other organizations.The American Recovery and Reinvestment Act and the economic stimulus package (HITECH Act) passed by the US Congress of 2009 have jump-started progress towards a requirement that “doctors … show ‘meaningful use’ of an EHR system,” which means a comprehensive effort toward training in health information management systems (HIMS). The “carrot” is being offered in the form of financial and educational incentives, and the “stick” will arrive in the form of fines and/or legal restrictions for organizations who do not comply by 2014. This “stick” is arriving for workers at all levels in terms of discomfort, a steep learning curve, and possible layoffs if they are not willing or able to follow organizational procedures for processing data into records and information electronically to feed into the federal system. (Op. cit. Wikipedia, “Electronic Health Record.”)
- What? A Usable, Reliable, System-wide Electronic Health Record (EHR)This power point is an example of one of many forms of teaching tools Information Technology workers can use to cope with the many staff people who have input into and can benefit from using systems who need some kind of orientation and training.The Association of College and Research Libraries of the American Library Association posits that: “…An information literate individual is able to:Determine the extent of information needed Access the needed information effectively and efficiently Evaluate information and its sources critically Incorporate selected information into one’s knowledge base Use information effectively to accomplish a specific purpose Understand the economic, legal, and social issues surrounding the use of information, and access and use information ethically and legally”
- How Do Information Literacy, Technology and the Digital Divide Affect this Nationwide Project?The ACRL of the ALA continues, saying:“…Information literacy, while showing significant overlap with information technology skills, is a distinct and broader area of competence.” (ACRL/ALA 2009)A large number of front-end health care workers are barely literate in English on a reading and writing level, to say nothing of information literacy. Both a U.S. Department of Health, Center for Disease Control survey and Nursing Assistant Certified texts admit that though NACs are “the eyes and ears” of RNs, LPNs, technicians and physicians on hospital, clinical and resident care levels; they are on the bottom of the educational and financial hierarchy. All of the data measurements and collections in the world do not outweigh the observations, actions, reactions – both healing and harmful -- of human beings. If “The goal of health care is health,” we need to pair our information literacy and technology training with real individuals on the clinical level, which is where my interest lies.(Author’s personal experience in Nursing Assistant Certified (CNA-NAC) training at North Seattle Community College, Summer Quarter, 2009; during clinical practice at a Seattle care and rehabilitation center, and especially at the written and skills testing center (WA State Department of Health (DOH)) 4 October, 2009.(U.S.) Center for Disease Control (CDC), (online pdf doc), “An Introduction to the National Nursing Assistant Survey,” http://www.cdc.gov/nchs/data/series/sr_01/sr01_044.pdf (accessed 4 December, 2009), March, 2007 the National Center for Health Statistics; and Robertson, Beverly, Nursing Assistants: A Basic Study Guide, 9th edition, Spokane, WA, First Class Books, 2009.)
- Why Information Technology and Literacy Training? What are the Contributions of Health Information Management Systems andElectronic Medical Records Management EMRM (Electronic Medical Records Management):Longitudinal e-Record of Medical Treatment and ResultsBillingDrug History/ Allergy dataQuick ReferenceEase of Management/ SpeedArchiving IMPORTANCE:Health care (HC) Orgs SizeNumber of Clients, Personnel, RecordsExpense and Number of Paper RecordsBreadth of Research and AnalysisRapidly Changing Field(UBC-SLAIS, Heather MacNeill, Luciana Duranti, Terry Eastwood, Susie Stephenson, Rick Kopak et al. (Instructors); Recordkeeping, Records Management, Archival Diplomatics, Data Base Design et al.; University of British Columbia School of Library, Archive and Information Studies; Vancouver, B. C., 2002 – 2005, as interpreted and recorded by Wyndy J. Knox Carr, MFA, MLIS.)
- What do Information Technology Professionals Need to Keep in Mind While Planning, Designing, Implementing and Modifying Systems?It is important to:Monitor andEvaluatethroughout the prescribed procedures of:CreatingHandling andPreserving records.OUR SYSTEMS AND TRAINING CAN MAKE THESE TASKS EASY OR DIFFICULT FOR HUMANS TO DO.(UBC-SLAIS, ibid.)
- The Why and How – The Business Case for Well-Planned and Thought Out, Functional, User-friendly TechnologyLuciana Duranti taught me that there are Six Phases of Procedures or Transactions (Archival Diplomatics):InitiativeInquiryConsultationDeliberationDeliberation ControlExecutionThree Purposes of Classification:Maintain the archival bond and contextFacilitate retrieval (in context – create thesaurus &c. have copies to access)Disposition and retention (schedule) (timely and systematic so as to preserve the records and their long-term value)(UBC-SLAIS, ibid.)
- Who? We KNOW What the Government Regulatory Boards and Commissions Will Want from our Supervisors and Clients on a Business Level – Now How Do We Act as Mediators to Make that Happen on a Clinical, Human Level?“When computers came along, computer databases made keeping track of books and other formats of materials in libraries much easier to work with than they had been in card catalogues. How about patients and procedures?”You can see that I used a lot of entertaining and eye-catching clip art for this slide, because I’m right on the edge of some very important points for front-line workers. If I didn’t lose my audience in the first few text-heavy slides, they’ll still be with me for this one and the next…
- Efficiently and With Integration and Interoperability in Mind… The “prime mover” behind much of this federal regulation is the waste and inefficiency of the present patchwork of healthcare systems which are feeding electronic information in nationwide, regionally and enterprise-wide. If we are going to get our return on investment (ROI) from this massive project, assessment of its functionality needs to be thoroughly exercised from the beginning throughout the project in a disciplined manner. (We heard this very clearly and repeatedly from Patrick Dolan about the UW Medical CHARMS project.)It appears very important to adequately and honestly assess the organizational needs involved in training all front-end users all the way up through top management and administrators previous to and during the deployment of a new information technology system, as well as having included multidisciplinary representatives on steering committees responsible for IT selection and assessment as early as possible in the process. (Dolan, Patrick; CHARMS Project Coordinator, project for systems upgrade, (online), “Quarterly Interim U-TAC Project Status, CHARMS, July – September 2009,” www.washington.edu/provost/utac/status/2009/.../CHARMS_2009_Q3.pdf (accessed 4 December 2009), also in a presentation to our class (AHE 232) 3 December, 2009.Hebda and Czar, op. cit., p. 184-186.)
- Analysis -- "If you fail to plan, you plan to fail.” ... Benjamin FranklinBecause of the scope of the health provision system in the U.S., each organization will have to break down our own organization’s workflows into functions, and assess what forms and data are coming now into paper and electronic formats, and how they are going to come or are already coming into integrated and interoperable electronic media. Hebda and Czar recommend, after choosing a steering committee of diverse, multidisciplinary decision-makers and developing a common vision, “a thorough understanding of how information is currently collected and processed… assessing the internal environment…to determine what information is used, who uses it, and how it is used,” qualitatively and quantitatively. (Hebda, ibid., p. 187.)
- This Means: If We Have Analyzed the What and the Where Technologically,Have We Also Located and Included the Who? If we identify key players, departmental educators and “super users” from the outset to serve on committees, and if we act as a user-friendly bridge for communications and training, we will have a better chance of implementing functional systems and seeing our projects succeed.This kind of inclusive planning can make the training and rollout much more “doable.” The training, however, is even more personal than that to the individual organization and department; and more complex in terms of matching the trainers, materials and training methods to the workflows and learning styles of the different healthcare providers.
- Who, Who, Who and Who…. Communications, Team and Learning Styles“When users are frustrated,” we have to be patient, find out “what they’re actually doing,” “explain and communicate,” because they are often “fearful and embarrassed.” These are some of the suggestions that were implied or said outright by Sahar Far, Support Analyst of Harborview Hospitals’ IT Department, in her talk to our IT for Healthcare introductory class. As someone responsible for enterprise resource planning in an organization with 10,000 end users, nurses and user supply terminals; it is not surprising that she trolls the hallways and cubicles for actual names and titles to attach business functions and e-mails to; as well as the break and lunchrooms for warm, human bodies she can solicit complaints and suggestions from face-to-face. If she is responsible for user training and 100 e-mails a day as well as for the receiving and requisitioning report log fed to her through Pathway Financial Management and Intellishelf inventory control systems and popup reminders, it is imperative that she see herself as an in-house and system-wide consultant as well as an IT analyst. She states that 75% of her phone calls are about software questions, particularly logins and passwords.(Far, Sahar, Support Analyst, Harborview Medical Center and Hospitals, Seattle WA, Lecture to AHE 232, Introduction to Medical Software/ Information Technology Systems, North Seattle Community College, 21 October, 2009, Seattle, WA.)
- We Know What an IT System is and How it Does What it Does – But We Cannot Assume that our Users DoChris Dimickis a staff writer at the Journal of AHIMA (American Health Information Management Association) who notes, “More and more, HIM professionals are being called upon to conduct in-house training. Electronic health record (EHR) implementations, quality assurance measures, privacy and security compliance, and coding regulations have increased the amount of new knowledge HIM professionals must share both within their departments and throughout their facilities…That can be a tall order, because many have never formally been trained on how to train others.”(Dimick, Chris, AHIMA (American Health Information Management Association), (online), “Tips for Trainers,” http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_035108.hcsp?dDocName=bok1_035108 AHIMA Journal, (accessed 17 October, 2009).)
- Whether we call them Data, Information or Records;We are the Ones Training the People Feeding them in to the EHRData are “facts about people, things and events,” or, more technically, “groups of information that represent the qualitative or quantitative attributes of a variable or set of variables.” In medicine, a lot of data are technical, quantitative observations about measurable events or parts of humans, but we should never forget how much of it comes about in a “qualitative” manner.(Microsoft, GO! (text for BUS 169), “Access,” Chapters 12, 13, 14, Seattle, WA, 2009.Wikipedia – The Free Encyclopedia, (online), “Data,” http://en.wikipedia.org/wiki/Data (accessed 4 December, 2009).Robertson, op. cit.Dimick, Chris, (American Health Information Management Association), (online), “Tips for Trainers,” http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_035108.hcsp?dDocName=bok1_035108 (accessed 17 October, 2009).
- We Understand the Importance of Standardized, Classified Data Entry According to Protocols, Processes and Procedures, but Many of Our Users Do NotThis harks back to the root cause of all our work: The goal of healthcare is health. As Patrick Dolan of UW Medical also said, unlike the banking industry or auto manufacturing, we “can’t standardize our products (patients’ health).” Data Analyst and consultant Frank Bray considered his training skills exercised through summary charting as a major value offered at the highest levels to executives who all too often went with their “gut feeling,” due to the information provided to them from “the two or three people in the room,” and not from the breadth of IT data analysis he could provide. If, in this corporate or professional culture, that is true, and that evidence-based practice and the push for patient safety are behind our technological and financial goals as well; then the IT department needs to insert ourselves on the decision-making level, in administrative offices AND on the clinical floor in front of the input monitors with the front-end users too. (Dolan, Patrick, op.cit.Bray, Frank, Health Data Analyst in lecture to AHE 232, Introduction to Medical Software/ IT Information Systems, NSCC, 2 December, 2009.)
- Keep Goals in Mind –Empathize with Your Clients as a Consultant and Fellow EmployeeThis is a balancing point for the last step. There are limits to your knowledge, time, budget, equipment, software and capabilities; but “allow the patron to see you as a human being…you sympathize with them…set the patron at ease.” Gorman believes “it’s crucial for IT leaders to enable themselves and their organizations to engage clients in a trusted partnership, shifting their role from ‘order taker’ or ’technology wizard’ or even ‘naysayer’ or ‘bottleneck’ to the role of ‘problem-solving partner.’ …putting their capabilities together to build an optimum solution with which both sides are happy.”I do this in my power point by using clip art and natural-language quotes that show that I empathize with my clients’ irritations and ordinary responses to tech training. It’s like getting inoculated so we don’t get sick with a bigger problem! It’s like symptoms and calling in consultants and healing and being satisfied with a task well done. -- Getting the big concepts behind these bumps in their workflow is easier if they see themselves as part of a bigger system, team and cost-saving environment, too. They’re not going to be left behind or crushed in the cogs – we’re all going to move forward in “the Big Wave.” Hence, the rah-rah “you make a difference here” attitude, because they do! Systems, software, you, your budget, time and your area of expertise have limits where you shouldn’t “over-promise,” because the flip side of empathy and collegiality is not wanting to betray co-workers’ trust in you and your abilities.(Anderson, Craig, “How to be a person: Tips and tricks for virtual reference,” College and Research Libraries News, ACRL-ALA, Chicago, IL, vol. 70, no. 10, Nov. 2009, pp. 577-580.Gorman, XXXXX op. cit.
- Who and How? The IT Department as a Service where We are Consultants.We may or may not like it, but the IT Services Department is a service to all the people in and connected with our organizations; a service to the third-party payers, vendors and other organizations in our enterprise, system or region; and/or a service to the state or nation if we are employed by a part of the government to help implement an interoperable EHR system. In Leading IT Transformation – The Roadmap for Success,Oulette & Associates Consulting, Inc. describes “What Good Service Looks Like,” differentiates it from “servitude,” and suggests moving toward “A Client-Focused IT Culture” in 10 ways:Identify and avoid the service sins you commit when under pressure.Document who your clients are, as well as which services you provide to them.Define the levels of service you are willing and able to provide.Elicit feedback on the levels of service you choose to provide.Clarify problems before you start fixing them.Know what your clients' expectations are before trying to meet them.Learn something new about one of your clients (goals, hot buttons, concerns).If the service you provide is virtual, spend more time thinking about and creating touch points (Web sites, voicemail boxes) than if you were on-site.Ask clients for feedback on one self-service tool (or try it out yourself).Talk to a client and ask, "What is your biggest frustration with IT?" “What is the best thing IT does?(Oulette & Associates Consulting, Inc., Leading IT Transformation: the Roadmap for Success, “24/7: Science & Tech,” (online) http://library.books24x7.com/toc.asp?bookid=29166 (accessed 20 November 2009), King Co Library System, Seattle, WA, Kendall Hunt Publishing Co., 2009.)
- What? For Knowledge Workers, too,The Goal of Healthcare is HEALTHPeter Drucker, who coined the term “knowledge worker” in 1959 and was one of the Twentieth Century’s most brilliant “management gurus,” recognized early on what this creation of an optimal learning and training environment meant on the business and economic level. “Drucker also was influenced, in a much different way, by John Maynard Keynes, whom he heard lecture in 1934 in Cambridge. ‘I suddenly realized that Keynes and all the brilliant economic students in the room were interested in the behavior of commodities,’ Drucker wrote, ‘while I was interested in the behavior of people.’Over the next 70 years, Drucker’s writings would be marked by a focus on relationships among human beings, as opposed to the crunching of numbers. His books were filled with lessons on how organizations can bring out the best in people, and how workers can find a sense of community and dignity in a modern society organized around large institutions.” (Wikipedia, -- The Free Encyclopedia, “Peter Drucker,” http://en.wikipedia.org/wiki/Peter_Drucker (accessed 5 December, 2009), Beatty, Jack, The World According to Peter Drucker, New York : Free Press, p. 163, 1998, and Drucker, Peter F., The Ecological Vision, p. 75-76, (1993).)
- Working With the Human Mind… and Everything Else Attached to It!Not only we, but the providers of all kinds to whom we offer training and information, need friendly communication and courageous leadership skills as well as technical ones.Hebda and Czar advocate “the creation of a culture of safety (which) requires a nonpunitive environment in which errors, near misses, and potential problems can be reported without fear of reprisal.” That is, especially the reprisals of peer or supervisor pressure, losing our jobs or being demoted financially or within our organizations. This is towards an optimal learning and training environment, where all users’ positions in the workflow as knowledge workers are respected and brought into the equation. (Hebda, Toni; and Patricia Czar; op.cit., p. 21.)
- 1.“Welcome the patron like a real person (no scripts).”Search, retrieval and accurate consultation depend on standardized input to databases and logical methodology. This is the “interface” between clinical data management and human “resources” management: training that emphasizes the importance of timely, accurate and standardized data and information that will add up to authentic and usable knowledge in a user-friendly system. We will never “train ourselves out of our jobs,” because there will always be new employees and new systems, but our interest in and understanding of “people skills,” human nature and unique learning styles, will go a long way in making our jobs easier and more pleasant, and our systems successful.(Anderson, op. cit., )
- 2. “Get some background info.” Says Anderson.Who? Working With the Human Mind… and Everything else Attached to It!If we are going to not only train thousands of people to implement an integrated and interoperable national EHR system, but inspire them to want to do so in a “reliable, systematic and comprehensive” manner, “observing, reporting and charting” in standardized terminology in a context of classification within our IT systems, we are doing more than forcing rote memorization of tasks.(Anderson, op. cit., )
- 3.”Let them know how long this will be.”Once again, there are limits to the capabilities of the IT department, our own skills and the learning styles of our trainees – be honest about time and focal boundaries.4.”Do not be afraid of smileys.” ;-)We will never “train ourselves out of our jobs,” because there will always be new employees and new systems, but our interest in and understanding of “people skills,” human nature and uniqueness, will go a long way in making our jobs easier and more pleasant, and our systems successful.5.”Never leave them wanting more.”If you have a training session, call for info, e-mail turnaround or presentation; always clarify that you’ve answered their question, gone over the task structure or given them the resources that enable them to pursue their goals. They can come back tomorrow and ask again if what you told them doesn’t work. “You never want the patron to feel uncomfortable when asking for a little more help,” says Anderson, “it is a simple matter to come across as a fellow human being.”(Anderson, op. cit., p. 579.)
- Inspiring, Doable Information Technology Training Towards 2014In the classification schemes of libraries, archives, and the medical coding and terminology which rest on the sciences; search, retrieval and accurate consultation depend on standardized input to databases and logical methodology. This is the “interface” between clinical data management and human “resources” management: training that emphasizes the importance of timely, accurate and standardized data and information that will add up to authentic and usable knowledge in a user-friendly system. I have tried to show a mid-level power point designed to appeal to many of these levels of users, and pick out some of the most empathetic focus points to bridge between the world of information technology and clinical health care. My focal points are about the necessity to plan thoroughly with a needs assessment conducted with key “super users” and stakeholders to identify places and processes where data is recorded and becomes information, a broad design with the steps for systematic creation of the EHR repeated and understandable to all, cues about problem-solving and evaluation along the way, and a general review of the scope and cooperation necessary to make this integration and interoperability happen. Good luck and unity to us all!