1. It is the progressive state of immunodeficiency, caused by the organism,
HUMAN IMMUNO DEFICIENCY VIRUS (HIV)
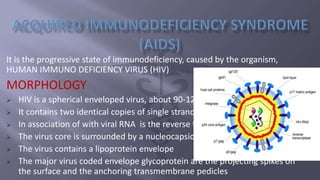
MORPHOLOGY
HIV is a spherical enveloped virus, about 90-120 nm in diameter.
It contains two identical copies of single stranded RNA genome
In association of with viral RNA is the reverse transcriptase enzyme.
The virus core is surrounded by a nucleocapsid composed of protein
The virus contains a lipoprotein envelope
The major virus coded envelope glycoprotein are the projecting spikes on
the surface and the anchoring transmembrane pedicles
2. Sexual contact
Parenteral transmission
Perinatal transmission
CLINICAL FEATURES
HIV infects all cells expressing at their surface the CD4 antigen,
which is the receptor for the virus.
It infects primarily the CD4+ lymphocytes
CLASSIFICATION SYSTEM FOR HIV INFECTIONS
AND AIDS (centre for disease control, USA)
3. Group 1 : acute HIV infection
Group 2 : asymptomatic infection
Group 3 : persistent generalized lymphadenopathy
Group 4 :
Subgroup A : constitutional disease
Subgroup B : neurological disease
Subgroup C : secondary infectious disease
Subgroup D : secondary cancers
Subgroup E : other conditions
ACUTE HIV INFECTIONS
The illness is chacterised by acute onset of fever, malaise, sore throat, myalgia, arthralgia, skin rash and lymphadenopathy
ASYMPTOMATIC INFECTIONS
This includes all infected persons who are usually well. They show positive HIV antibody tests, and are infectious
PERSISTENT GENERALISED LYMPHADENOPATHY
Enlargement of lymph nodes is seen
SYMPTOMATIC HIV INFECTIONS
When CD4+ lymphocytes count falls below 400 mm3, the patient may develop symptoms like fever, diarrhoea, weight loss, night sweats
and opportunistic infections
OPPORTUNISTIC INFECTIONS AND MALGNANCIES COMMONLY ASSOCIATED WITH HIV
INFECTIONS
BACTERIAL
1. Mycobacterial infections – tuberculosis and non tuberculosis infections
2. M. avium complex
3. Salmonellosis
5. 2. Cryptosporidiosis
3. Isosporiasis
4. Generalised strongyloidiasis
MALIGNANCIES
1. Kaposi’s sarcoma
2. B cell lymphoma or non Hodgkins lymphoma
ORAL MANIFESTATIONS
1. Patients with AIDS are at greater risk for bacterial, viral, fungal infections of the mouth
2. Dental caries and gingivitis may occur
3. Acute ulcerative gingivitis may act as an indicator that the patient may hav aids
4. Herpes simplex infections may be present as multiple, deeper, more painful oral lesions in
patients with aids
5. Hair leukoplakia is an early sign of immunodefeciancy, induced by Epstein barr virus
6. Candidiasis may be present in most patients with HIV infections, asymptomatic
erythematous lesions of candidiasis, angular chelitis, mucocutaneous candidiasis are seen
6.
7. RANGE OF SURGERY IN HIV PATIENTS
1. ANORECTAL DISEASE: It is the most frequent reason for surgical treatment in HIV patients, seen
commonly in homosexuals, grouped together as “ AIDS ANUS SYNDROME”
CAN BE CLASSIFIED AS :
a. Anal warts, diarrhoe
b. Incontinence in homosexuals
2. ABDOMINAL PAIN: it is due to gastrointestinal oppurtinistic infection, usually caused by
cytomegalovirus. It is a type of colitis, produces abdominal pain, cramps, loose stools, blood and mucous
in stools
a. APPENDICITIS: is alsocommon due to CMV
b. ABDOMINAL LYMOHOMA , with involvement of liver and spleen also causes abdominal pain
c. SEVERE ABDOMINAL PAIN: may be due to perforation of small or large bowel which should be treated
as an emergency
3. LYMPHOMA & KAPOSI’S SARCOMA: they are due to reduced cellular immunity, due to following
reason:
a. Immunosuppresion used in organ transplantation
b. Severe malnourishment
c. HIV infection
d. Lymphoproliferative disease
Kaposi’s sarcoma can affect skin surface, gastro intestinal tract from mouth to anus, lungs etc. It present
as pigmented multifocal skin lesions
10. 4. OESOPHAGAL ULCERS: can present and odynophagia. Endoscopy should de done by using a
glove & the scope should be washed thoroughly with soap & water and immersed in cetremide
solution for 15 min
5. Very often surgeons are called for lymph node biopsy for evaluation of fever or generalized
lymphadenopathy.
DIAGNOSIS OF AIDS
An individual with opportunistic infections, lymphopenia, low CD4 but relatively normal CD8 in
the pheripheral blood, raised IgG & IgA levels & poor skin tests to common recall antigens may
well have AIDS, particularly if they come from group at risk
LABORATORY DIAGNOSIS
1. Antigen detection , p24 is the earliest virus marker to appear in the blood. ELISA can be used
for detection of this antigen
2. Detection of virus nucleic acid, through polymerase chain reaction(pcr)
3. Antibody detection
a. Screening tests
ELISA TEST
RAPID TEST
SIMPLE TEST
b. Supplemental tests
WESTERN BLOT TESTS
11. PROPHYLAXIS
No effective vaccine has yet been found out. High rate of mutation of virus has made difficulty
in developing the vaccine
ANTIRETROVIAL THERAPY (ART)
Specific treatment with antiretroviral drugs is the mainstay in the management of HIV infections. HIGHLY ACIVE
ANTIRETROVIAL THERAPY (HAART) is effective in inhibition of HIV replication in most of the HIV infected individuals
NUCLEOSIDE REVERSE TRANSCIPTASE INHIBITORS
ZIDOVUDINE
LAMIVUDINE
STAVUDINE
NON NUCLEOSIDE REVERSE TRANSCRIPTASE INHIBITORS
NEVIRAPINE
DELAVIRIDINE
PROTEASE INHIBITORS
SAQUINAVIR
RITONAVIR
LOPINAVIR
INDINAVIR
TIPRANAVIR
12. UNIVERSAL PRECAUTIONS TO BE FOLLOWED ARE
IN OUTPATIENT DEPARTMENT
Any patients with open wounds, gloves are worn when examining thepatient
Hand gloves and eye protection durng flexible endoscopy
Use disposable instruments
Reusuable instruments like endoscope are washed with soap & water and immersed in gluterldehyde
soln
No surgical procedures involving sharp instruments is performed in the OPD
IN OPERATING ROOM
Operation room is covered with single sheet of polythene
The no of threatre personel is reduced to minimum
The staff with abrasions & lacerations on their hands are not allowed inside the threatre
SURGICAL TECHNIQUE
Avoid sharp injury
Prefer scissors to scalpel
Use skin clips
Avoid needle stick injury
Proper autoclaving at the end of surgery