Presentation1.pptx, radiological imaging of cholangiocarcinoma.
•Télécharger en tant que PPTX, PDF•
42 j'aime•7,413 vues

This document discusses radiological imaging techniques for cholangiocarcinoma (bile duct cancer). It provides details on: - Ultrasound, CT, MRI, MRCP, and ERCP are discussed for imaging bile duct cancer. Each modality has benefits for assessing tumor location and extent. - Peripheral, hilar, and intrahepatic cholangiocarcinoma are described along with the Bismuth-Corlette classification system for hilar tumors. - Imaging features of peripheral, hilar, intrahepatic cholangiocarcinoma are shown including enhancement patterns and involvement of bile ducts.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Presentation1.pptx, radiological imaging of cholangiocarcinoma.
Similaire à Presentation1.pptx, radiological imaging of cholangiocarcinoma. (20)
Plus de Abdellah Nazeer
Plus de Abdellah Nazeer (20)
Presentation1.pptx, radiological imaging of cholangiocarcinoma.
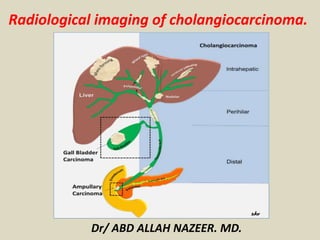
- 1. Dr/ ABD ALLAH NAZEER. MD. Radiological imaging of cholangiocarcinoma.
- 3. Ultrasound (US)Transabdominal(TA US). Endoscopic(EUS). Computed Tomography (CT). Endoscopic Retrograde Cholangiopancreatography(ERCP). Magnetic Resonance Imaging (MRI). Magnetic Resonance Cholangiopancreatography(MRCP). Radiological Imaging:
- 4. Biliary tract cancer is the second most common primary hepatobiliary malignancy after hepatocellular carcinoma. Malignancies may occur along any part of the biliary tract from the ampulla of Vater to the smallest intrahepatic ductules and the gallbladder. The entire biliary tree, including the gallbladder is lined with a simple columnar epithelium and malignant transformation of this epithelium gives rise to predominantly adenocarcinomas. The pathogenesis of biliary tract and gallbladder carcinoma is thought to be secondary to an evolutionary sequence from metaplasia to dysplasia to carcinoma. Metaplasia usually occurs in the setting of inflammation and chronic injury. Dysplasia of the biliary tract, is considered as pre-invasive biliary neoplasia and can occur in up to 40% to 60% of patients with invasive carcinoma, one third of patients with sclerosing cholangitis, and found incidentally in 1 to 3.5% of cholecystectomy specimens
- 5. Classically, the cancers of the biliary tract were separated into three categories: (i) cancer of the intrahepatic biliary tract, (ii) cancer of the gallbladder and extrahepatic bile ducts, and (iii) cancer of the ampulla of Vater. The term cholangiocarcinoma was initially used to refer only to the primary tumors of the intrahepatic bile ducts and is now extended to include intrahepatic, perihilar, and distal extrahepatic tumors of the bile ducts. Gallbladder cancer is defined as cancer arising from the gallbladder and the cystic duct. Ampullary cancers are rare and have better prognosis than cancers of the distal bile duct. Cancers arising from the distal common bile duct immediately adjacent to the ampulla of Vater tend to behave clinically similar to the cancers of the ampulla of Vater, head of pancreas and the duodenal bulb and therefore often considered under the broad category of periampullary carcinomas.
- 6. Cholangiocarcinoma: Pathogenesis and Epidemiology Bile duct cancer arising in the intrahepatic, peri-hilar, or distal biliary tree, exclusive of gallbladder and ampulla of Vater. Originate from epithelial cells of biliary duct 90% adenocarcinoma, 10% squamous cell carcinoma. Highly lethal: often locally advanced at presentation. 5-year-survival rate: 5-10%.
- 7. Risk Factors Primary sclerosing cholangitis Life time risk: 10-15% Average age at time of diagnosis: 30s-50s Fibropolycystic liver disease i.e. Caroli’s syndrome, congenital hepatic fibrosis, choledochal cysts Lifetime risk: 15% Average age at time of diagnosis: 30s-50s Parasitic Infection Liver flukes of Clonorchis and Opisthorchis genera (from undercooked fish) Cholelithiasis and haptolithiasis Toxic exposure Thorotrast Lynch syndrome and biliary papillomatosis Chronic liver disease Viral hepatitis.
- 8. Common Clinical Manifestations Symptoms: Pruritus (66%) RUQ pain (30-50%) Weight loss (30-50%) Fever (20%) Alcoholic stools; dark urine Cholangitis(rare Physical Signs: Jaundice (90%) Hepatomegally (25-40%) RUQ mass (10%) Courvoisier’s sign (rare)
- 9. Tumor Classification. Intrahepatic(Peripheral): small intra hepatic ductules(5-10%)(yellow). Hilar: extrahepatic ductules (including confluence) up to point where common bile duct lies posterior to duodenum(60-70%)Klatskin: involving confluence of left and right hepatic ducts. (blue). Extrahepatic(Distal): originate in extrahepatic biliary duct after CBD travels posterior to duodenum (20-30%).(Orange).
- 10. Drawings illustrate various types of intrahepatic Cholangiocarcinoma as classified by the Liver Cancer Study Group of Japan. (a) Mass-forming intrahepatic Cholangiocarcinoma manifests as a round mass with a distinct border in the liver parenchyma. (b) Periductal infiltrating intrahepatic Cholangiocarcinoma is characterized by tumor infiltration along the bile duct (arrow). It occasionally involves the surrounding blood vessels or hepatic parenchyma. (c) Intraductal intrahepatic cholangiocarcinoma is characterized by papillary or granular growth within the bile duct lumen. It occasionally demonstrates superficial extension (right arrow) or forms a tumor thrombus in an obstructed duct (left arrow). More than one type of cholangiocarcinoma may manifest in a single patient. In such cases, all of the types involved should be
- 11. Bismuth-Corlette Classification Hilar cholangiocarcinomas are further sub-classified based on the specific ducts involved Type I Type II Type IIIa Type IIIb Type IV Type IV is important because it involves both left and right hepatic ducts and therefore is unrespectable.
- 12. Schematic diagram of the Bismuth–Corlette classification scheme for perihilar tumors. Type I: tumor confined to CHD duct, obstructing the duct within 2 cm of the hilum. Type II: tumor of the CHD bifurcation involving both main right and left hepatic ducts, and causing obstruction at the hilum with no communication between the main right and left hepatic ducts. Type IIIa and IIIb: tumors extending into right and left secondary intrahepatic ducts, respectively, with absence of ductal obstruction on the contralateral side. Type IV: tumor involves the secondary and tertiary intrahepatic ducts in both lobes causing bilateral obstruction.
- 13. TNM Tumor Staging Stage Grouping: Stage I: T1 N0 M0 Stage II: T2 N0 M0 Stage IIIA: T3 N0 M0 Stage IIIB: T4 N0 M0 Stage IIIC: any T N1 M0 Stage IV: any T any N T0 No evidence of primary tumor T1 Solitary tumor w/o vascular invasion. T2 Solitary tumor with vascular invasion, or multiple tumors <5cm. T3 Multiple tumors >5cm or tumor involving major branch of portal or hepatic veins. T4 Tumors with direct invasion of adjacent organs other than the gallbladder or with perforation of the visceral peritoneum. N0 No regional lymph node metastasis N1 Regional lymph node metastasis M0 No distant metastasis M1 Distant metastasis
- 15. Cholangiocarcinoma with Hyper-enhancement on Delayed Images
- 16. Peripheral cholangiocarcinoma. (a) Arterial-phase CT scan shows a low-attenuation mass (marker) with rim enhancement. Note the dilatation of the peripheral intrahepatic ducts (arrows). (b) On a portal-phase CT scan, the mass looks smaller because the central portion is now more enhanced. The rim enhancement seen in a is partially washed out. Capsular retraction is also noted (arrow).
- 17. Peripheral mass-forming cholangiocarcinoma (a) Noncontrast multidetector CT scan obtained prior to contrast material administration shows an irregular hypoattenuating lesion in segments VII and VIII of the liver (arrows) with retraction of the posterior liver surface and atrophy of the right lobe. (b) On an arterial phase multidetector CT scan, the lesion is predominantly hypoattenuating with minimal peripheral enhancement posteriorly (arrow). (c) Delayed phase multidetector CT scan shows the lesion with peripheral enhancement (black arrows) and progressive enhancement posteriorly (white arrow), although the center of the lesion remains hypoattenuating (*).
- 18. Peripheral cholangiocarcinoma with involvement of confluence. Infiltrating pCCA of the left hepatic duct (arrow) isodense to liver parenchyma on axial contrast enhanced CT (a) with dilation of the left hepatic ducts. The ductal thickening is hyperintense (arrow) on T2-weighted MRI image (b) with extension to the confluence causing mild dilatation of the right hepatic ducts demonstrated better on MRCP (c).
- 19. peripheral cholangiocarcinoma. (a) Fat-saturated T1-weighted MR image obtained after the intravenous administration of gadolinium-based contrast material shows a heterogeneously enhancing lesion (arrows). (b) On a fat-saturated T1-weighted MR image obtained after the administration of manganese dipyridoxylethylenediamine diacetate bisphosphate, the lesion (arrows) appears hypointense relative to the enhancing liver. The use of this contrast agent increases lesion-liver contrast and lesion conspicuity.
- 20. Peripheral cholangiocarcinoma demonstrates peripheral heterogeneous enhancement. The tumor has been outlined to indicate a region of interest for the calculation of vascularization parameters. The decrease in tumor vascularization after antiangiogenic drug administration, seen in b, was confirmed with transfer constant and extracellular volume fraction calculations.
- 21. Intrahepatic cholangiocarcinoma (iCCA) on ultrasound in two different patients. Mass forming iCCA may present as a well-defined hypoechoic mass (arrow, a) or as an ill-defined heterogeneous isoechoic mass (arrowheads, b).
- 22. Intraductal intrahepatic cholangiocarcinoma in a 53-year-old man. (a) CT scan shows a dilated bile duct in segment VII of the liver (arrows). The bile duct has higher attenuation in the right lobe than in the left lobe. (b) On a T2-weighted MR image, the signal intensity of the right posterior superior intrahepatic duct (B7) (open arrows) is not as high as that of other bile ducts (solid arrows). (c) Photograph of the resected specimen shows granular, friable papillary masses (arrows) in dilated intrahepatic ducts. (Fig 3a and 3c reprinted, with permission, from reference 11.)
- 23. CCA of common hepatic duct with involvement of confluence. Contrast enhanced CT (a), T2-weighted MRI (b) and MRCP (c) images demonstrating thickened and enhancing common hepatic duct (arrow) with involvement of the confluence and upstream dilatation of the intrahepatic ducts. The ductal thickening appears hypointense (arrow) to the surrounding dilated bile ducts on T2-weighted MRI image (b). The involvement of the confluence is demonstrated better on MRCP.
- 24. CCA of common hepatic duct with involvement of confluence. Ultrasound with color flow overlay (a) showing an echogenic mass (arrow) filling the common hepatic duct with upstream dilatation of the intrahepatic ducts. EUS image (b) showing a hilar lymph node and was sampled positive for carcinoma. Contrast enhanced CT in arterial phase (c) and portal venous phase (d) showing enhancing mass (arrow) within the duct and no major vascular involvement. The ductal mass is hyperintense on T2-weighted image (e) and hypointense on T1-weighted image (f) and shows concentric post contrast enhancement (g). MRCP (h) shows the confluence invasion and non- visualization of the common hepatic duct.
- 25. MRCP of a classical Klatskin’s tumor. The confluence, proximal hepatic ducts and proximal common hepatic duct are strictured (arrow). The common bile duct is of normal caliber.
- 26. Hilar CCA presenting as an intraluminal mass with biliary obstruction. The mass is isodense (arrow) on the coronal non-contrast enhanced CT (a) and hypointense on axial T2-weighted image (b) with upstream dilatation of the intrahepatic ducts. ERCP (c) shows a filling defect (arrow) representing the mass extending into the common bile duct with no filling of the intrahepatic ducts.
- 27. Perihilar CCA arising from the cystic duct and proximal gall bladder (arrows) with invasion of common hepatic duct. The pCCA is mildly hyperintense on T2-weighted image (a), hypointense on T1-weighted image (b) and shows post contrast enhancement (c). Both MRCP (d) and ERCP (e) demonstrate the stricture of the common hepatic duct till the confluence above and cystic duct insertion below. The gall bladder is not visualized on ERCP and the irregularity of the proximal cystic duct (arrowhead) is due to the tumor.
- 28. Cholangiocarcinoma. (a) Axial fat-suppressed T2-weighted MR image shows a high-signal- intensity lobulated mass in the right hepatic lobe (arrow). (b, c) Contrast-enhanced arterial phase (b) and equilibrium phase (c) T1-weighted MR images show irregular, ragged rim enhancement (arrows in b) with gradual centripetal enhancement (arrowheads in c).
- 29. Polypoid type iCCA. Axial T2 sections (a, b) and MRCP (c) demonstrating an isointense filling defect (white arrow) in the right hepatic duct and extending into the common hepatic duct with dilation of intrahepatic ducts. Post contrast enhanced T1-weighted images (d-f) shows the mildly enhancing filling defect representing intraductal papillary neoplasm which extended from just under hepatic capsule filling right hepatic ducts to 3 cm below the confluence of right and left hepatic ducts.
- 30. Mixed type iCCA. T2-weighted axial (a), MRCP (b), T1-weighted axial (c) and post contrast T1-weighted axial (d) images demonstrating a predominantly periductal thickening (stricturing iCCA) and also mass forming (arrow) in the right lobe liver. Note the separation of the right intrahepatic ducts on MRCP (arrowheads).
- 31. Cirrhosis of liver with iCCA. T2-weighted axial (a), T1-weighted axial (b) and post gadolinium enhanced T1-weighted axial arterial phase (c), portal venous phase (d) and delayed phase (e) images showing iCCA as an iso- to hyperintense lesion (arrow) in posterior right lobe with typical arterial phase rim like enhancement and progressive central enhancement through delayed phase without any washout. The liver parenchyma is heterogeneous and nodular consistent with cirrhosis.
- 33. Intrahepatic cholangiocarcinoma in a 35-year-old female who presented with right upper quadrant abdominal pain and no prior medical history. There is a large lobulated mass (arrow) in the right lobe of the liver, which, compared to liver parenchyma, is hypointense on the (a) axial T1-weighted (T1W) in-phase spoiled gradient-echo (SGRE) image, and mildly hyperintense on the (b) axial T2-weighted (T2W) fast spin echo (FSE) with fat saturation image. The mass shows heterogeneous rim enhancement on the (c) arterial-dominant phase gadolinium-enhanced axial T1W 3D SGRE image with fat saturation, and fills in heterogeneously on the (d) delayed (15 min) gadolinium-enhanced axial T1W SGRE image. A presumed metastatic nodule (white open arrow) is seen in the lateral segment of the left lobe on an (e) axial T2W FSE with fat suppression image. CT guided biopsy of the dominant mass revealed a cholangiocarcinoma.
- 34. Infiltrating hilar cholangiocarcinoma with tumoral involvement of the right secondary confluence and common hepatic duct. (a) CT scan reveals a high-attenuation tumor on the anterior aspect of the right portal vein (arrowheads). (b) On a subsequent CT scan, the tumor appears as a high-attenuation lesion on the right side of the portal vein (arrowheads). (c, d) CT scans (d obtained at a lower level than c) show the mucosa of the cystic duct with strong enhancement (open arrow), a finding that suggests tumoral involvement. Soft tissue infiltration around the portal vein (arrowheads) and lymphadenopathy (solid arrow) are also noted.
- 35. Perihilar cholangiocarcinoma (Klatskin tumor) in a 62-year-old female presenting with painless jaundice. There is mass (arrow) at the junction of the main right and left hepatic ducts. The mass is seen on (a) an MRCP image as a focal stricture involving the duct bifurcation with dilatation of the intrahepatic ducts, left more than right, due to the presence of a right intrabiliary stent. In (b) T1W in-phase SGRE, the mass is hypointense relative to liver parenchyma, and mildly hyperintense on (c) T2W FSE with fat suppression. A susceptibility artifact from the right intrahepatic stent is demonstrated (asterisk). The mass enhances progressively (d–g) following gadolinium administration: in (d) the arterial-dominant phase, (e) portal- venous phase, (f) interstitial phase (2 min post-gadolinium), and is best depicted on (g) the 15 min post- gadolinium image as a hyperintense mass relative to adjacent liver parenchyma.
- 36. Intraductal infiltrating cholangiocarcinoma of the proximal CBD. (a) Delayed phase contrast-enhanced fat-saturated T1-weighted MR image shows enhancement of the cholangiocarcinoma (arrow). (b) On a diffusion-weighted image obtained at the same level, the lesion (arrow) is hyperintense with restricted diffusion.
- 37. Intraductal cholangiocarcinoma in a 70-year-old male who presented with jaundice. An intraductal mass was found on ERCP. There is a minimally enhancing mass within the right main hepatic duct (arrow) on the (a) axial gadolinium- enhanced T1 SGRE image. The mass extends to the bifurcation of the ducts, and has resulted in intrahepatic ductal dilatation. The intraductal cholangiocarcinoma is seen as a filling defect (arrow) on the (b) coronal T2W SSFSE MRCP images. Cytology and brushings revealed a cholangiocarcinoma.
- 38. Hilar cholangiocarcinoma in a 62-year-old man who presented with jaundice and abdominal pain. (a) Coronal fat-saturated T2-weighted MR image through the liver reveal a mass at the hilum (arrow) with dilatation of the intrahepatic biliary radicals (arrowheads). (b) FDG PET scan through the hilum (arrow) does not show increased activity. The lesion proved to be a cholangiocarcinoma at histopathologic analysis.
- 39. Extrahepatic cholangiocarcinoma at US and ERCP.
- 40. Distal CCA. Common bile duct stricture due to grade 4 invasive carcinoma. Coronal T2-weighted image (a) and MRCP (b) image showing a short segmental narrowing (arrow) with proximal dilatation. ERCP (c) showing a short segmental stricture representing the invasive CCA.
- 41. Distal CCA presenting as a polypoid mass with obstructive jaundice. Contrast enhanced CT axial (a) and coronal reconstruction (b) showing a soft tissue density filling defect in distal common bile duct (arrow) representing the invasive grade 3 adenocarcinoma.
- 42. Polypoid extrahepatic cholangiocarcinoma with diffuse bile duct involvement in a 65-year- old man. (a, b) CT scans (b obtained at a lower level than a) show a dilated common bile duct filled with a papillary tumor (arrow). (c) CT scan shows partial restoration of the ductal lumen in the intrapancreatic portion of the common bile duct. However, small papillary tumors are still evident (arrow). (d) On a CT scan obtained at the level of the distal common bile duct, the lumen is again filled with an intraductal papillary tumor (arrow). (e) Direct cholangiogram shows a large papillary tumor in the proximal two-thirds and the distal portion of the common bile duct (arrows). Because of this extensive tumoral involvement, palliative resection was the only possible treatment.
- 43. Perihilar cholangiocarcinoma in a 64-year- old female who presented with painless jaundice and had focal stenosis of the common bile duct on ERCP. There is a perihilar mass (arrow), which is hypointense to liver on (a) axial T1W in- phase SGRE, mildly hyperintense on (b) T2W FSE with fat saturation, has little to no arterial enhancement on (c) the arterial-dominant phase gadolinium- enhanced axial T1W 3D SGRE, mild enhancement on the (d) 2 min post- gadolinium image, and the tumor becomes mildly hyperintense to liver on the (e) 15 min post-gadolinium image. The tumor surrounds and narrows the main portal vein (white open arrow), and the right main hepatic artery (black open arrow) on a (f) higher slice. (g) Coronal thick slab T2W single shot fast spin-echo (SSFSE) MRCP image demonstrates long segment narrowing of the common hepatic and proximal common bile duct, with a stent traversing the stenotic segment as well as dilation of the intrahepatic bile ducts. (h) A corresponding minimum intensity projection (Min IP) reformatted image demonstrates the mildly enhancing mass surrounding the narrowed segment of common hepatic duct (curved arrow).
- 44. Cholangiocarcinoma. (a) Out-of-phase gradient-echo T1-weighted MR image shows a hypointense lobulated mass in the right hepatic lobe (arrows). (b) On a fat-saturated T2-weighted MR image, the mass appears hyperintense (arrows). (c) Early-phase contrast-enhanced T1-weighted MR image shows irregular peripheral enhancement of the mass (arrows). (d) Delayed phase contrast-enhanced T1-weighted MR image shows progressive heterogeneous enhancement of the lesion (*).
- 45. Cholangiocarcinoma. (a) Fat-saturated T2-weighted MR image shows a hyperintense mass in the left hepatic lobe and extending to the porta hepatis (arrow), with dilatation of the biliary radicals in both lobes (arrowheads). (b) Out-of-phase gradient echo T1-weighted MR image shows the mass encasing the left portal vein (arrow) and extending to the porta hepatis. (c, d) Corresponding contrast-enhanced MR angiograms show encasement of the left hepatic artery (arrow in c) and invasion and non visualization of the left portal vein (arrow in d), which prohibited surgery.
- 46. Cholangiocarcinoma: Non enhanced, arterial, portal venous and equilibrium phase.
- 47. PET-CT of iCCA. Axial PET-CT images showing a large FDG-avid iCCA (arrow) with central photopenia (*) indicating necrosis/fibrosis with FDG-avid portal lymph node (a, arrow head) and aortocaval lymph node (b, arrow head) consistent with lymph node metastases.
- 48. Ampullary carcinoma. Contrast enhanced axial CT (a) and coronal reformat (b) showing a small polypoid mass (arrow) representing carcinoma in the ampulla of the bile duct.
- 49. Ampullary carcinoma. Contrast enhanced axial CT (a) and sagittal reformat (b) showing a small polypoid mass representing carcinoma in the ampulla of the bile duct.
- 50. Biliary Dilatation and CHD Stricture on HASTE MRI
- 51. Dilated Bile Ducts and CHD Stricture on MRCP
- 54. Summary. Radiographic diagnosis, and an even more challenging cancer to treat. 3 classifications of Cholangiocarcinoma: Intrahepatic Hilar(including Klatskin) Extrahepatic Hilar cholangiocarcinomas are further sub-classified based on specific ductal involvement, by the Bismuth-Corlette classification system. Many radiographic modalities are important in the diagnosis of Cholangiocarcinoma. US, CT, ERCP, MRCP, MRI Radiology is helpful in determining surgical respectability, and can influence surgical management.
- 55. Thank You.