1. P A R T N E R S O R T H O P A E D I C
Trauma Rounds
Case Reports from the Mass General Hospital and Brigham & Women’s Hospital
A Quarterly Case Study Volume 2, Fall 2010
Femur Fractures around Hip Implants
David Lhowe, MD findings confirm loosening. Thus, preoperative anesthetic
evaluation should allow for a potentially prolonged procedure.
Approximately 200,000 total hip replacements
Treatment is nearly always surgical, with the exceptions of the
and an equal number of hemiarthroplasties are
Vancouver A patterns or non-displaced B or C patterns in pa-
performed annually in the United States. With
tients who are not surgical candidates. Positioning the patient
the marked success of this procedure, patients
in lateral decubitus on a radiolucent table allows the preferred
are able to maintain active lifestyles for many
lateral approach to the femur to be easily extended to an ante-
more years. Consequently, millions of elderly
rior or posterior hip approach, should a revision of the femoral
are at risk for fracture around their prosthesis.
component be necessary.
Periprosthetic fractures typically result from common house-
Surgery follows established concepts for plate fixation of other
hold falls. The Mayo Clinic reported a 1% prevalence of peri-
long bones - including restoration of proper length, alignment,
prosthetic fracture after primary THR, increasing to 4% follow-
and rotation without devas-
ing revision surgery.1 Barring dramatic improvements in treat-
cularization of fracture frag-
ing osteoporosis or reducing falls in an aging population, peri-
ments. The femoral stem
prosthetic fractures will become an increasing medical and so-
must be adequately exposed
cietal burden.
to confirm its fixation within
Fortunately, the majority of periprosthetic fractures do not re- the proximal fragment.
sult in implant loosening and may be managed without the Anatomic reduction is not
need for implant revision. These fractures include the isolated necessary for comminuted
trochanteric fractures (Vancouver A), diaphyseal fractures about fractures, and the dissection
a well-fixed stem (Vancouver B1), and fractures well below the required to achieve it is det-
distal tip of the stem (Vancouver C). Complex management rimental to fracture healing.
with revision of components is required when the femoral stem Apart from simple 2-part
is loose (Vancouver B2) and loosening is further complicated by fractures where anatomic
inadequate bone stock (Vancouver B3). These variants are ap- reduction and rigid fixation
propriately referred to experienced hip revision surgeons. can be reasonably obtained, a
bridge plating technique is
Evaluation of the periprosthetic femur fracture is best accom-
preferable. Fixation is ob-
plished with plain radiographs of the pelvis and entire femur.
tained proximally and dis-
CT/MR scans are degraded by artifacts from the metal and add
tally without disturbing the
little. Inflammatory markers like ESR and C-reactive protein
fracture fragments, and the
are invariably elevated and of no therapeutic value. Aspiration
plate is sufficiently long to
of the joint or fracture site should be reserved for cases where
obtain adequate fixation – at
infection is suspected by history or clinical signs. If the fixation
least 2 cortical diameters
of the femoral component is questionable, surgery should be
above and below the frac-
planned to include possible revision in the event that operative
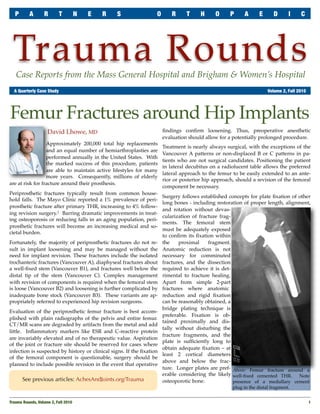
ture. Longer plates are pref- Above: Femur fracture around a
erable considering the likely well-fixed cemented THR. Note
See previous articles: AchesAndJoints.org/Trauma osteoporotic bone. presence of a medullary cement
plug in the distal fragment.
Trauma Rounds, Volume 2, Fall 2010
1
2. P A R T N E R S O R T H O P A E D I C T R A U M A R O U N D S
Fixation of the proximal fragment is com- may be late to appear and may never be
plicated by the femoral stem, but screws visible in cases where the surgeon
may often be passed anterior or posterior achieved anatomic reduction.
to it. Locking screws may provide better
fixation in poor quality bone, but cannot Prognosis for healing of periprosthetic
be angled around an implant as easily as fractures is good if the above principles
standard screws. When adequate screw are maintained during treatment. Risk of
fixation is not obtainable, cerclage cables subsequent implant loosening is in-
passed through eyelets screwed into the creased, with the Swedish national hip
plate will suffice. The absolute number of arthroplasty registry showing a 30% loos-
fixation points for each fragment has not ening rate at 10 years following peripros-
been established, but most critical are thetic fracture.3
those screws or cables closest to and fur-
thest from the fracture zone.2 References:
1. Berry DJ, Epidemiology: Hip and Knee. Orthop Clin
Allograft cortical struts may provide in- North Am 1999; 30:183-190.
creased stability, but require substantial 2. Ricci WM, et al, Indirect Reduction and Plate Fixation
Without Grafting, for Periprosthetic Femoral Shaft Frac-
soft tissue stripping from the fracture and tures About a Stable Intramedullary Implant. J Bone
interpose avascular cortical bone between Joint Surg Am 2006; 88:275-282.
the fracture and its investing musculature 3. Lindahl H, et al., Risk Factors for Failure After Treat-
- an environment which can compromise ment of a Periprosthetic Fracture of the Femur. J Bone
Joint Surg Br 2006; 88:26-30.
fracture healing. The availability of more
rigid and lockable plates with optional
New England Regional Fracture Summit
cable augmentation has supplanted the
Jan 14 - 17, 2011, Stowe, VT
need for structural allografts in nearly all
The AO Fracture Summit will be held January
cases.
14 – 17, 2011 in Stowe, VT. The course features
Rehabilitation begins with hip/knee Trauma Rounds Editor Dr Mark Vrahas, as
range-of-motion and straight leg raises to well as Drs Jesse Jupiter and Raymond White
minimize quadriceps atrophy. Touch- as course co-chairs. The legendary Dr Augusto
Sarmiento will be the course’s Guest Sage.
down weight-bearing should be main- Above: Fracture repaired using a locking
plate, with fixation utilizing both standard The purpose is to inform and educate commu-
tained for a minimum of 6 weeks or longer
bicortical and locking screws, augmented nity orthopaedic surgeons who are actively
when comminution is greater or fixation with a single cable proximally. The involved in the treatment of patients with
less secure. A longer period of protected comminuted fracture zone has been bridged, fractures. The format is informal, discussion-
weight-bearing is necessary when fracture and the medullary cement removed. Callus based, and highly interactive. Participants are
vascularity has been compromised by the is seen forming medially at 6 weeks post-op.
invited to bring their own cases for discussion.
previous surgery or by current repair tech- Sign-up for Email Updates: Registration is still open!
niques. Periosteal new bone formation
AchesAndJoints.org For more information: www.aona.org
Trauma Faculty Michael Weaver, MD — 617-525-8088 Editor in Chief
Mark Vrahas, MD — 617-726-2943 BWH Orthopedic Trauma
Mark Vrahas, MD
Partners Chief of Orthopaedic Trauma mjweaver@partners.org
mvrahas@partners.org David Ring, MD — 617-724-3953 Program Director
Mitchel B Harris, MD — 617-732-5385 MGH Hand & Upper Extremity Service
Suzanne Morrison, MPH
dring@partners.org
Chief, BWH Orthopedic Trauma (617) 525-8876
mbharris@partners.org George Dyer, MD — 617-732-6607 smmorrison@partners.org
BWH Hand & Upper Extremity Service
R Malcolm Smith, MD, FRCS — 617-726-2794
gdyer@partners.org Editor, Publisher
Chief, MGH Orthopaedic Trauma
rmsmith1@partners.org Please send correspondence to: Arun Shanbhag, PhD, MBA
Mark Vrahas, MD / Trauma Rounds
David Lhowe, MD — 617-724-2800 Yawkey Center for Outpatient Care, Suite 3C
MGH Orthopaedic Trauma 55 Fruit Street, Boston, MA 02114
dlhowe@partners.org www.MassGeneral.org/ortho
www.BrighamAndWomens.org/orthopedics
2
Trauma Rounds, Volume 2, Fall 2010