
Recommandé
Recommandé
Contenu connexe
Similaire à Hsv 6350 Module I Part 1 Neurobiology Of Trauma Dr. Mark Sloane
Similaire à Hsv 6350 Module I Part 1 Neurobiology Of Trauma Dr. Mark Sloane (20)
Plus de benjatchison
Plus de benjatchison (15)
Dernier
Dernier (20)
Hsv 6350 Module I Part 1 Neurobiology Of Trauma Dr. Mark Sloane
- 1. The Impact of Child Trauma &The Impact of Child Trauma & Prenatal Alcohol Exposure onPrenatal Alcohol Exposure on Neurobiological Development &Neurobiological Development & FunctionFunction Western Michigan UniversityWestern Michigan University College of Health & Human ServicesCollege of Health & Human Services HSV 6350-105HSV 6350-105 Special Topics Course: Child TraumaSpecial Topics Course: Child Trauma Module I , Part IModule I , Part I Mark A. Sloane, DO Center for Behavioral Pediatrics WMU Children’s Trauma Assessment Center Kalamazoo, MI
- 3. Western Michigan University SW MI Children’s Trauma Assessment Center
- 4. Module 2Module 2 • Brief review of normal brainBrief review of normal brain developmentdevelopment • Review of “Brain-Behavior Connections”Review of “Brain-Behavior Connections” in FASD & child traumatic stressin FASD & child traumatic stress • Neurodevelopmental Function in FASDNeurodevelopmental Function in FASD & child traumatic stress& child traumatic stress • Treatment overview in FASD & childTreatment overview in FASD & child traumatic stresstraumatic stress
- 6. The Harsh Reality…The Harsh Reality… • Research continually demonstrates theResearch continually demonstrates the harmful effects of child traumatic stress &harmful effects of child traumatic stress & prenatal alcohol exposureprenatal alcohol exposure • We have aWe have a reactivereactive system rather than asystem rather than a proactiveproactive systemsystem • We minimize the impact to these childrenWe minimize the impact to these children toto protect ourselvesprotect ourselves from thefrom the overwhelming awareness of howoverwhelming awareness of how damaging their experiences aredamaging their experiences are
- 7. Exploring the “Why” BehindExploring the “Why” Behind Problematic BehaviorProblematic Behavior • Requires aRequires a reframingreframing of often long-of often long- standing paradigms re the etiology of “badstanding paradigms re the etiology of “bad behavior”behavior” • Multiple factors: This isMultiple factors: This is complexcomplex !!!!!! • Requires aRequires a community-wide shiftcommunity-wide shift ofof thinking differentlythinking differently • The power of theThe power of the trans-disciplinarytrans-disciplinary mindsetmindset
- 8. Paradigm Shift:Paradigm Shift: Reframing Our Understanding of BehaviorReframing Our Understanding of Behavior • ““Bad” behavior in children & adolescents isBad” behavior in children & adolescents is often about faulty & defective brain wiringoften about faulty & defective brain wiring • It is not disrespect because the child isIt is not disrespect because the child is ““BADBAD ”” • Perceived “bad” children:Perceived “bad” children: – DoDo NOTNOT have adequate skills of flexibility/adaptability…have adequate skills of flexibility/adaptability… – Often have low frustration tolerance…Often have low frustration tolerance…
- 10. Our typical response to “bad”Our typical response to “bad” behavior in childrenbehavior in children • These kids get all kinds of labelsThese kids get all kinds of labels – Educational System (special education classifications)Educational System (special education classifications) – Medical System (DSM-IV diagnostic categories)Medical System (DSM-IV diagnostic categories) – Legal System (at-risk teen, juvenile delinquent)Legal System (at-risk teen, juvenile delinquent) • They often get labels that imply they areThey often get labels that imply they are BADBAD oror NAUGHTYNAUGHTY • ADHD, Oppositional Defiant Disorder (ODD), ConductADHD, Oppositional Defiant Disorder (ODD), Conduct Disorder, Bipolar Disorder (& even PTSD)Disorder, Bipolar Disorder (& even PTSD) diagnoses dodiagnoses do NOTNOT capture the full extent of the neurodevelopmental &capture the full extent of the neurodevelopmental & neurobehavioral impact for kids with problem behaviorsneurobehavioral impact for kids with problem behaviors
- 11. These labels just don’t fit!!!
- 12. The challenge of dealing withThe challenge of dealing with difficult children…difficult children… • ““It may be when we no longer know what toIt may be when we no longer know what to do…do… • we come to ourwe come to our real workreal work…… • And…when we no longer know which wayAnd…when we no longer know which way to go…to go… • we have begun ourwe have begun our real journeyreal journey.”.”
- 14. News FlashNews Flash:: We live in strange times!We live in strange times! • Modern Western society hasModern Western society has benefited (beyond the dreams ofbenefited (beyond the dreams of our ancestors) from many advancesour ancestors) from many advances in:in: – TechnologyTechnology – CommunicationsCommunications – TransportationTransportation – Social JusticeSocial Justice – EconomyEconomy …however….
- 15. News Flash:News Flash: We live in strange times!We live in strange times! • Our society seemsOur society seems incapableincapable ofof ensuring that our children grow upensuring that our children grow up in environments that are:in environments that are: – SafeSafe – PredictablePredictable – Rich in positive relationshipsRich in positive relationships – HumaneHumane
- 16. News Flash:News Flash: We live in strange times!We live in strange times! • Hundreds of thousands of children areHundreds of thousands of children are terrorized, abused, neglected, maltreated,terrorized, abused, neglected, maltreated, exposed to alcohol/drugs each yearexposed to alcohol/drugs each year • These kids are atThese kids are at great riskgreat risk for emotional,for emotional, behavioral, social, cognitive, and physicalbehavioral, social, cognitive, and physical health problemshealth problems • The overall costs are incalculableThe overall costs are incalculable • How can we really measure the lost potentialHow can we really measure the lost potential here?here?
- 17. News Flash:News Flash: We live in strange times!We live in strange times! • How “advanced” is our societyHow “advanced” is our society when…when… – We have to create vast expensive governmentWe have to create vast expensive government agencies whose sole purpose is to protectagencies whose sole purpose is to protect children from their parents!children from their parents! – These very agencies (despite our best efforts)These very agencies (despite our best efforts) truly failtruly fail these unfortunate children by…these unfortunate children by… • Recreating the chaos, fragmentation, trauma, andRecreating the chaos, fragmentation, trauma, and neglect these kids experienced in their biologicalneglect these kids experienced in their biological homeshomes
- 18. A Step Closer…A Step Closer… to understanding these kidsto understanding these kids The Brain – BehaviorThe Brain – Behavior ConnectionConnection
- 19. Normal Brain DevelopmentNormal Brain Development and Organizationand Organization
- 20. Brain GlossaryBrain Glossary • Neuron (nerve cell)Neuron (nerve cell) – ““Raw material” of the brainRaw material” of the brain – 100 billion neurons at birth (most of what we100 billion neurons at birth (most of what we will need throughout life)will need throughout life) • SynapseSynapse – The connection between neuronsThe connection between neurons – 1,000 trillion synapses by age 31,000 trillion synapses by age 3 – 500 trillion synapses by adolescence500 trillion synapses by adolescence • Due to “pruning” (discarding)Due to “pruning” (discarding)
- 21. Brain Development / LearningBrain Development / Learning • The process of creating, strengthening, &The process of creating, strengthening, & discarding synapsesdiscarding synapses • Synapses organize the brain by formingSynapses organize the brain by forming neuronal pathways that connect the parts of theneuronal pathways that connect the parts of the brain governing everything we do:brain governing everything we do: – BreathingBreathing – SleepingSleeping – ThinkingThinking – FeelingFeeling
- 22. Neurobiology of DevelopmentNeurobiology of Development • NatureNature PLUSPLUS nurture !!!nurture !!! • ““Hard-wired” genetic programs (blueprints) areHard-wired” genetic programs (blueprints) are continuously modified by the environment (fromcontinuously modified by the environment (from conceptionconception →→ death)death) • Brain “sculpts” itself in response to theBrain “sculpts” itself in response to the environmentenvironment AT THE SAME TIMEAT THE SAME TIME it isit is developing (via genetic blueprints)developing (via genetic blueprints) • ““These interactions organize our brain’sThese interactions organize our brain’s development and thus shape the person wedevelopment and thus shape the person we become”become” (Shore 1997)(Shore 1997)
- 23. From simple to complex:From simple to complex: Hierarchy of brain functionHierarchy of brain function Brain- stem Diencephalon Limbic Neocortex Abstract Thought Concrete Thought Affiliation w/ mate Attachment Sexual Behavior Emotional Reactivity Motor Regulation Arousal Appetite / Satiety Sleep BP / Heart Rate Respiratory Drive Body TemperaturePerry 2006 All sensory input enters here
- 24. Neural systems change in aNeural systems change in a use-use- dependentdependent fashion duringfashion during developmentdevelopment • Healthy organization of all neuralHealthy organization of all neural networks depends upon:networks depends upon: – PatternPattern – FrequencyFrequency – TimingTiming of key experiences during developmentof key experiences during development • ExampleExample: Child must be exposed to language-: Child must be exposed to language- rich environment to develop optimal languagerich environment to develop optimal language functionfunction
- 25. Brain develops in sequential fashion:Brain develops in sequential fashion: from simple to complexfrom simple to complex Brain- stem Diencephalon Limbic Neocortex Development begins here
- 26. The brain develops most rapidlyThe brain develops most rapidly earlyearly in lifein life • By age 4, the brain is 90% of adult size!By age 4, the brain is 90% of adult size! • It is much easier to organize the brain inIt is much easier to organize the brain in healthy ways in early childhood…healthy ways in early childhood… • It is much more difficult to re-organize aIt is much more difficult to re-organize a poorly organized brainpoorly organized brain due todue to traumatic stress and / or FASDtraumatic stress and / or FASD
- 27. Neural systems can be changed…Neural systems can be changed… but some systems are easier to changebut some systems are easier to change Brain- stem Diencephalon Limbic Neocortex Complexity Plasticity & Ease of change
- 28. The Brain-Behavior connection:The Brain-Behavior connection: three primary componentsthree primary components • GeneticsGenetics – What you inherit from both parentsWhat you inherit from both parents • Intrauterine environmentIntrauterine environment – During pregnancyDuring pregnancy • Extrauterine environmentExtrauterine environment – After pregnancyAfter pregnancy
- 29. The Brain-Behavior ConnectionThe Brain-Behavior Connection • GeneticsGenetics – Neurodevelopmental strengths /Neurodevelopmental strengths / weaknessesweaknesses – Temperament / PersonalityTemperament / Personality – Family history of:Family history of: • Attentional disordersAttentional disorders • Learning disordersLearning disorders • Mood disordersMood disorders • Neuropsychiatric disordersNeuropsychiatric disorders
- 30. The Brain-Behavior ConnectionThe Brain-Behavior Connection (cont.)(cont.) • Intrauterine environmentIntrauterine environment – Exposure to drugs (legal / illegal)Exposure to drugs (legal / illegal) – Exposure to alcoholExposure to alcohol – Maternal stressMaternal stress – Maternal nutritionMaternal nutrition
- 31. The Brain-Behavior ConnectionThe Brain-Behavior Connection (cont.)(cont.) • Extrauterine environmentExtrauterine environment – Parental attachment / nurturingParental attachment / nurturing – Parental style / psychopathologyParental style / psychopathology – Overall family climateOverall family climate – Influence of extended family systemInfluence of extended family system – Inadequate nutritionInadequate nutrition – Exposure to violence, natural disastersExposure to violence, natural disasters – Exposure to neglectExposure to neglect – Exposure to abuse (verbal / emotional /Exposure to abuse (verbal / emotional / physical / sexual)physical / sexual)
- 32. Brain-Behavior Connection:Brain-Behavior Connection: Embracing ComplexityEmbracing Complexity Genetic Risk Trauma Prenatal Exposure Genetic Potential Behavior
- 33. Effects of Traumatic Stress onEffects of Traumatic Stress on “Normal” Individuals“Normal” Individuals Normal Gene Normal Behavior normal development Normal Circuit Normal Gene normal development Normal Circuit T R A U M A Normal Behavior Neurodevelopmental Delays Neurobehavioral Symptoms Stahl 2002
- 34. Effects of Prenatal AlcoholEffects of Prenatal Alcohol Exposure on “Normal” IndividualsExposure on “Normal” Individuals Normal Gene Normal Behavior normal development Normal Circuit Normal Gene abnormal development Compromised Circuit Normal Behavior Neurodevelopmental Delays Neurobehavioral Symptoms P A R L E C N O A H T O A L L
- 35. Worst-case scenario:Worst-case scenario: The “Triple-Whammy”The “Triple-Whammy” Vulnerable Gene +MH Family History Development Compromised Circuit Most severe: Neurobehavioral Symptoms Neurodevelopmenta l P A R L E C N O A H T O A L L Abnormal T R A U M A Normal Behavior
- 36. Influence of Prenatal AlcoholInfluence of Prenatal Alcohol ExposureExposure
- 37. Fetal Alcohol SyndromeFetal Alcohol Syndrome •FAS is among theFAS is among the mostmost commoncommon of the knownof the known causes of cognitivecauses of cognitive impairmentimpairment – A major public health problem.A major public health problem. – How common is it? (1-3/1000 liveHow common is it? (1-3/1000 live births in US?)births in US?) – Regional variationsRegional variations – How does it affect the CNS?How does it affect the CNS? – What can we do about it?What can we do about it? – Why don’t more professionalsWhy don’t more professionals know about it?know about it?
- 38. Fetal Alcohol SyndromeFetal Alcohol Syndrome • ““Discovered” in 1968 &Discovered” in 1968 & 19731973 • Specific pattern of facialSpecific pattern of facial featuresfeatures • Evidence of CentralEvidence of Central Nervous System (CNS)Nervous System (CNS) dysfunction / damagedysfunction / damage • Growth deficiencyGrowth deficiency Photo courtesy of Teresa Kellerman
- 39. FAS: only the tip of the iceberg!FAS: only the tip of the iceberg! Fetal Alcohol SpectrumFetal Alcohol Spectrum Disorders (FASD)Disorders (FASD) • Fetal Alcohol SyndromeFetal Alcohol Syndrome • Alcohol-relatedAlcohol-related Neurodevelopmental DisorderNeurodevelopmental Disorder (ARND)(ARND) (“mild-moderate” FAS)(“mild-moderate” FAS) • Prenatal Exposure to AlcoholPrenatal Exposure to Alcohol (clinically suspected to have FAS but(clinically suspected to have FAS but appearappear physically normalphysically normal )) Adaped from Streissguth
- 40. Smooth philtrum Thin upper lip ↓ palpebral fissure (small eyes) FASD: Critical Facial Abnormalities
- 41. Hoyme, H. E. et al. Pediatrics 2005;115:39-47 Assessment of FAS: Lip-Philtrum guides
- 42. Hoyme, H. E. et al. Pediatrics 2005;115:39-47 Measurement of palpebral fissures in FAS
- 43. Chudley, A. E. et al. CMAJ 2005;172:S1-21S FAS Assessment: Measuring palpebral fissure length
- 44. Hoyme, H. E. et al. Pediatrics 2005;115:39-47 Genetic Disorders with some of the Craniofacial Features of FAS Williams Syndrome DeLange Syndrome VCFS
- 45. Fetal Alcohol Syndrome:Fetal Alcohol Syndrome: It doesn’t always look like thisIt doesn’t always look like this
- 46. FASFAS:: It can also look like this!It can also look like this!
- 47. …and this!…clinical examples of FAS: transcending race
- 48. Adapted from Sulik & Johnston, 1982 ……and even this!!!...and even this!!!... Facial features of FAS in a mouseFacial features of FAS in a mouse Small eyes Flat philtrum Normal control mouse FAS mouse
- 49. Courtesy of Ann Streissguth Growing up with FASGrowing up with FAS
- 50. Hippocampus Amygdala Cingulate Hypothalamus Major brain areas affected by prenatal alcohol exposure Thalamus Corpus Callosum
- 51. Sensorimotor Cortex Cerebellum Dorsolateral Pre-frontal Cortex (PFC) Brainstem (Locus Ceruleus, Raphe, Ventral Tegmentum) Other key brain structures also affected by prenatal alcohol exposure Orbital PFC Corpus Callosum
- 52. Severe brain damage caused bySevere brain damage caused by prenatal alcohol exposureprenatal alcohol exposure photo: Clarren, 1986 5-day old infants Severe FAS Normal Brain
- 53. Corpus callosum abnormalities in FASDCorpus callosum abnormalities in FASD Mattson, et al., 1994; Mattson & Riley, 1995; Riley et al., 1995
- 54. Mechanisms of cellular damage byMechanisms of cellular damage by ethanol in FASDethanol in FASD • Timing is everything!Timing is everything! • Binge drinking vs chronic alcohol useBinge drinking vs chronic alcohol use • John OlneyJohn Olney (Wash U. – St. L)(Wash U. – St. L) mouse model:mouse model: – GABA A & glutamate (NMDA) receptor dysfunctionGABA A & glutamate (NMDA) receptor dysfunction – Serotonin system dysfunctionSerotonin system dysfunction – Disrupted synaptogenesis (neurons makingDisrupted synaptogenesis (neurons making connections with other neurons)connections with other neurons) – Results inResults in ↑↑ programmed cellular suicideprogrammed cellular suicide (apoptosis)(apoptosis)
- 55. Risk Factors for FASD:Risk Factors for FASD: Why doesn’t every fetus exposed toWhy doesn’t every fetus exposed to alcohol look the same?alcohol look the same? • Dose of alcoholDose of alcohol (mom’s blood alcohol level =(mom’s blood alcohol level = fetal blood alcohol level)fetal blood alcohol level) • Pattern of exposurePattern of exposure : binge > chronic drinking: binge > chronic drinking • Developmental timingDevelopmental timing of alcohol exposureof alcohol exposure • Genetic variationsGenetic variations • Synergistic reactions with other drugsSynergistic reactions with other drugs • Interaction with nutritional variablesInteraction with nutritional variables • Socio-economic statusSocio-economic status • Possible neuroprotective factorsPossible neuroprotective factors
- 56. Child Traumatic Stress &Child Traumatic Stress & the Developing Brainthe Developing Brain
- 57. Traumatic Stress & the Child’sTraumatic Stress & the Child’s Developing BrainDeveloping Brain • Research reveals aResearch reveals a strong linkstrong link betweenbetween all types ofall types of childchild abuseabuse and theand the subsequent development ofsubsequent development of psychiatricpsychiatric illness in adulthoodillness in adulthood • Until recently, many/most MH professionalsUntil recently, many/most MH professionals felt that these psychiatric conditionsfelt that these psychiatric conditions developed viadeveloped via psychologicalpsychological means:means: – ““software” problems amenable tosoftware” problems amenable to reprogramming (talk therapy) or simply erasablereprogramming (talk therapy) or simply erasable (“Just get over it”)(“Just get over it”)
- 58. Traumatic Stress & the Child’sTraumatic Stress & the Child’s Developing BrainDeveloping Brain • Early childhood traumatic stressEarly childhood traumatic stress to the developing brain results in:to the developing brain results in: – Physical (not always permanent) changesPhysical (not always permanent) changes :: • ““Hard-wired” neurological changesHard-wired” neurological changes • Causes abnormal CNS organization / functionCauses abnormal CNS organization / function • Profound implications re behavior /Profound implications re behavior / development / learning / cognitiondevelopment / learning / cognition • Prevents realization of genetic potentialPrevents realization of genetic potential
- 59. What does traumatic stress changeWhat does traumatic stress change in the brain?in the brain? • AttachmentAttachment • Affect / Emotion RegulationAffect / Emotion Regulation • Information ProcessingInformation Processing
- 60. Hippocampus Amygdala Cingulate Hypothalamus Major brain areas affected by traumatic stress Thalamus Corpus Callosum
- 61. Sensorimotor Cortex Cerebellum Dorsolateral PFC Brainstem (Locus Ceruleus, Raphe, Ventral Tegmentum) Other key brain structures also affected by traumatic stress Orbital PFC Corpus Callosum
- 62. It’sIt’s deja vudeja vu all over again!!!all over again!!! Yogi Berra Famous US philosopher
- 63. Neurobiologic “Controversy”Neurobiologic “Controversy” • Two prominent researchers in FASD (EdTwo prominent researchers in FASD (Ed Riley) & traumatic stress (Martin Teicher)Riley) & traumatic stress (Martin Teicher) recently met and wererecently met and were unableunable toto differentiate their MRI research slidesdifferentiate their MRI research slides • New strategies greatly needed to researchNew strategies greatly needed to research these two groupsthese two groups separatelyseparately • Here is a brief look at some recentHere is a brief look at some recent functional MRI research…functional MRI research…
- 64. Recent Neuroscience ResearchRecent Neuroscience Research • New brain research has dramaticallyNew brain research has dramatically altered our thinking about traumatized /altered our thinking about traumatized / FASD childrenFASD children • New neuroimaging methods have drivenNew neuroimaging methods have driven this research:this research: – Quantitative MRI (Magnetic Resonance Imaging)Quantitative MRI (Magnetic Resonance Imaging) – Functional MRIFunctional MRI – PET (Positron-Emitted Tomography)PET (Positron-Emitted Tomography) – SPECT (Single-Photon Emitted ComputedSPECT (Single-Photon Emitted Computed Tomography)Tomography) – MRS (Magnetic Resonance Spectroscopy)MRS (Magnetic Resonance Spectroscopy) – DTI (Diffusion Tensor Imaging)DTI (Diffusion Tensor Imaging)
- 65. Adult ADHD Neuroimaging StudyAdult ADHD Neuroimaging Study • 8 Adults with ADHD8 Adults with ADHD • 8 Controls8 Controls • George Bush, MD, PhDGeorge Bush, MD, PhD • Functional MRIFunctional MRI • Performed Stroop test while in fMRIPerformed Stroop test while in fMRI scannerscanner
- 66. Stroop TestStroop Test RedRed BlueBlue GreenGreen YellowYellow xxxxxxxx xxxxxxxx xxxxxxxx xxxxxxxx RedRed BlueBlue GreenGreen YellowYellow RedRed BlueBlue GreenGreen YellowYellow
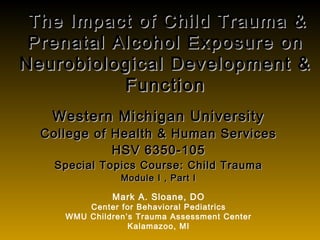
- 67. MGH-NMR Center & Harvard-MIT CITP. Adapted from Bush, et al. Biol Psychiatry. 1999;45:1542-1552. 1 x 10 -3 1 x 10-2 1 x 10 -3 y = +21 mm y = +21 mm Normal control ADHD Anterior Cingulate Cortex Frontal Striatal Insular network fMRI shows decreased blood flow to the anterior cingulate and increased flow in the frontal striatum in adult ADHD patients Neuroimaging and ADHDNeuroimaging and ADHD 1 x 10-2
- 68. OK…it’s time to make it real!OK…it’s time to make it real!
- 69. What does all of this mean toWhat does all of this mean to health professional students?!health professional students?! • 5 CNS pathways to explosive /5 CNS pathways to explosive / inflexible kids:inflexible kids: – Executive Function SkillsExecutive Function Skills – Language-Processing SkillsLanguage-Processing Skills – Emotion regulation SkillsEmotion regulation Skills – Cognitive Flexibility SkillsCognitive Flexibility Skills – Social SkillsSocial Skills Ross Greene, 2005
- 70. Traumatic Stress / FASDTraumatic Stress / FASD and the Developing Brain:and the Developing Brain: Executive Function: Making it realExecutive Function: Making it real • Working MemoryWorking Memory (“RAM” of the brain)(“RAM” of the brain) – Allows efficient multi-taskingAllows efficient multi-tasking • Separation of affectSeparation of affect – Regulating arousal to achieve goals (e.g. learning)Regulating arousal to achieve goals (e.g. learning) • Organization & planningOrganization & planning – Facilitates problem-solvingFacilitates problem-solving • Shifting cognitive setShifting cognitive set – Allows child to smoothly transition from their ownAllows child to smoothly transition from their own agenda to the supervising adult’s agendaagenda to the supervising adult’s agenda
- 71. Traumatic Stress / FASDTraumatic Stress / FASD and the Developing Brain:and the Developing Brain: Language Processing: Making it realLanguage Processing: Making it real • Often unnoticed, often unassessedOften unnoticed, often unassessed • Problems identifying internal emotionsProblems identifying internal emotions • Lack the capacity to “inform the world” thatLack the capacity to “inform the world” that they arethey are frustratedfrustrated • Problems with conflict resolutionProblems with conflict resolution Teacher: “Use your words, young man!”Teacher: “Use your words, young man!” Student: “(expletives deleted)”Student: “(expletives deleted)”
- 72. Traumatic Stress / FASDTraumatic Stress / FASD and the Developing Brain:and the Developing Brain: Emotional Control: Making it realEmotional Control: Making it real • Impaired ability of the right brainImpaired ability of the right brain to communicate w/ the left brainto communicate w/ the left brain – Via Corpus Callosum (connects R with L)Via Corpus Callosum (connects R with L) – Balance problemsBalance problems – Sensory processing problemsSensory processing problems – Anger / explosiveness (Anger / explosiveness (↓↓ self-calming)self-calming) – Loss of logical left brain functionLoss of logical left brain function (language / memory) when stressed(language / memory) when stressed
- 73. Traumatic Stress / FASDTraumatic Stress / FASD and the Developing Brain:and the Developing Brain: Emotional Control: Making it realEmotional Control: Making it real • Traumatized / FASD kids oftenTraumatized / FASD kids often have significant difficultyhave significant difficulty regulatingregulating emotional experienceemotional experience :: – ProblemsProblems expressingexpressing emotions in a safeemotions in a safe mannermanner – ImpairedImpaired modulationmodulation of emotionalof emotional experienceexperience
- 74. Traumatic Stress / FASDTraumatic Stress / FASD and the Developing Brain:and the Developing Brain: Emotional Control: Making it realEmotional Control: Making it real • ““Fight-Flight-Freeze” phenomenon isFight-Flight-Freeze” phenomenon is common & underappreciatedcommon & underappreciated – Hypersensitive / overactive F-F-F system often aHypersensitive / overactive F-F-F system often a daily battle for traumatized / FASD childrendaily battle for traumatized / FASD children – Fear / AnxietyFear / Anxiety ⇒⇒ Anger connectionAnger connection • ““Look in their eyes during a meltdown (if you dare) andLook in their eyes during a meltdown (if you dare) and you will often see fear” …MASyou will often see fear” …MAS – Amygdala is the key player hereAmygdala is the key player here
- 77. Traumatic Stress / FASDTraumatic Stress / FASD and the Developing Brain:and the Developing Brain: Cognitive Flexibility: Making it realCognitive Flexibility: Making it real • Concrete / literal thinkersConcrete / literal thinkers • Rigid behavioral templates for specificRigid behavioral templates for specific situationssituations • Rule-driven (to a fault)Rule-driven (to a fault) • Over-focus on detailsOver-focus on details • Overlap with the autistic spectrumOverlap with the autistic spectrum
- 78. Traumatic Stress / FASDTraumatic Stress / FASD and the Developing Brain:and the Developing Brain: Social Skills: Making it realSocial Skills: Making it real • Impulse control problemsImpulse control problems • Pragmatic language impairmentPragmatic language impairment • Inaccurate interpretation of socialInaccurate interpretation of social informationinformation • Unable to predict social outcomesUnable to predict social outcomes
- 79. Time to find your happy place!
- 80. End of Part 1 / Module 2End of Part 1 / Module 2 • Please proceed to Part 2, Module 2Please proceed to Part 2, Module 2
Notes de l'éditeur
- Background This slide illustrates an extremely important point. Fetal alcohol syndrome only represents one point on what appears to be a continuum of effects from prenatal alcohol exposure. Towards one end may be fetal death and FAS. As one moves to the other end of the continuum, one may find isolated effects resulting from prenatal alcohol: maybe only some of the facial characteristics or maybe only behavioral problems. The point is that FAS represents only a small sampling of the effects of prenatal alcohol. Many more children are included when we consider those with FAE who might or might not have obvious signs of alcohol exposure, and those that do not manifest any physical features of FAS, but have behavioral problems. FAS is only the tip of the iceberg. Interestingly only 10 – 40% of children of chronic alcohol abusers can be diagnosed as having FAS. However, there is very good data suggesting that these non-FAS children are affected, most notably behavioral and cognitive deficits. Even in children with normal IQs who have been exposed to alcohol prenatally, there is evidence that they do not live up to their true potential. Fetal Alcohol Spectrum Disorder (FASD) is now being proposed as a term that encompasses the entire spectrum of fetal alcohol toxicity and is soon to be adopted by several national agencies.
- The pendulum has swung to and fro regarding the nature/nurture argument, i.e., which is more important in the development of behavior in children??? We have finally arrived at a midpoint as it is clear that all of the above elements are important in the shaping of behavior. What is interesting is that the genetic blueprint of personality and temperament is directly affected by both the intra- and extrauterine environment.
- Most at-risk students with learning, attentional, mood, and behavioral problems in the classroom setting have a combination of the above factors (along with a learned behavior component) causing these behaviors.
- Background Fetal alcohol syndrome is among the most common known causes of mental retardation and as such, it is a major public health problem. The purpose of this lecture is to provide a basic overview of what we know about the effects of prenatal alcohol exposure. It is certainly not meant to be comprehensive. For more detailed overview, the following references might be helpful. It is important to remember that as the mother consumes alcohol and her blood alcohol level rises, that alcohol is freely crossing the placenta and the embryo or fetus is being exposed to the same blood alcohol levels. References Stratton, K., Howe, C., & Battaglia, F. (1996). Fetal alcohol syndrome: Diagnosis, epidemiology, prevention, and treatment. Washington, DC: National Academy Press. Streissguth, A. P. (1997). Fetal Alcohol Syndrome: A Guide for Families and Communities. Baltimore: Paul H. Brookes Publishing Co.
- Background What each of these papers described was a common set of features that could occur in the offspring of mothers who drank heavily during their pregnancies. This constellation of features was named the Fetal Alcohol Syndrome in 1973 by Jones and colleagues. In order to be diagnosed as having FAS, the individual MUST meet all three criteria. There is a specific pattern of facial anomalies, which will be shown shortly. There is pre and or postnatal growth deficiency. Usually the children are born small (<25th percentile) and remain small, at least until puberty. Finally, there must be evidence of central nervous system dysfunction. This CNS dysfunction might be physical (e.g. microcephaly) or behavioral (hyperactivity, mental retardation). There are pitfalls in the diagnosis of FAS. Sometimes the complete pattern of anomalies is not present. Various terms have been proposed for these cases (FAE – Fetal alcohol effects, ARBD – Alcohol related birth defects, ARND – Alcohol related neurobehavioral disorder), but each has its limitations and no fixed terminology has been accepted. Another problem relates to the age at which the diagnosis is conducted. It appears to be easier to diagnose this condition in young children, while the diagnosis in the neonatal period may be more difficult. Furthermore, changes in the face may occur as the individual grows into adulthood and obscure the typical facial appearance of FAS. For a more thorough discussion of the diagnosis of FAS and various related conditions, the reader is referred to the IOM report (Stratton et al, 1996). Of concern is the 1) the necessity of documenting the exposure history of the mother, 2) the reluctance of physicians to inquire about the drinking histories of pregnant women, or women contemplating pregnancies, and 3) the fact that many physicians are not well trained or not confident in their ability to recognize these effects.
- Background This slide illustrates an extremely important point. Fetal alcohol syndrome only represents one point on what appears to be a continuum of effects from prenatal alcohol exposure. Towards one end may be fetal death and FAS. As one moves to the other end of the continuum, one may find isolated effects resulting from prenatal alcohol: maybe only some of the facial characteristics or maybe only behavioral problems. The point is that FAS represents only a small sampling of the effects of prenatal alcohol. Many more children are included when we consider those with FAE who might or might not have obvious signs of alcohol exposure, and those that do not manifest any physical features of FAS, but have behavioral problems. FAS is only the tip of the iceberg. Interestingly only 10 – 40% of children of chronic alcohol abusers can be diagnosed as having FAS. However, there is very good data suggesting that these non-FAS children are affected, most notably behavioral and cognitive deficits. Even in children with normal IQs who have been exposed to alcohol prenatally, there is evidence that they do not live up to their true potential. Fetal Alcohol Spectrum Disorder (FASD) is now being proposed as a term that encompasses the entire spectrum of fetal alcohol toxicity and is soon to be adopted by several national agencies.
- Background One model developed by Kathy Sulik uses mice. By exposing pregnant mice to high doses of alcohol during brief periods of gestation, she has been able to produce a mouse with the facial features of FAS. On the left is the control animal and the right the alcohol exposed animal. Note the small eye openings (palpebral fissures) and the long flat area under the nose (philtrum). Utilizing this model, Sulik and colleagues have been able to demonstrate that neural crest cells are especially sensitive to the effects of embryonic alcohol exposure and that the death of these cells may be responsible for the cranial facial defects in FAS. References Kotch, L. E., and Sulik, K.K. Experimental fetal alcohol syndrome: Proposed pathogenic basis for a variety of associate craniofacial and brain anomalies. Am. J. Med. Genet. 44, 168-176, 1992. Sulik, K. K., & Johnston, M. C. (1982). Embryonic origin of holoprosencephaly: Interrelationship of the developing brain and face , Scanning Electron Microscopy (Vol. 1, pp. 309-322).
- Here are two other children with FAS at four different ages. The FAS features are apparent even as these children mature.
- Background The brain on the left was obtained from a 5-day-old child with severe, fatal FAS while the brain on the right is a control. The effects are obvious. The brain on the left suffers from microencephaly (small brain) and migration anomalies (neural and glia cells did not migrate to their proper location in the brain, but instead many of them simply migrated to the top of the cortex). Although it cannot be seen here, there is also agenesis of the corpus callosum and the ventricles are dilated. The corpus callosum is the major fiber tract connecting the two hemispheres of the brain (more on this later). Major findings of other autopsies of children with FAS have found microcephaly, hydrocephaly, cerebral dysgenesis, neuroglial heterotopias, corpus callosum anomalies, ventricle anomalies, and cerebellar anomalies. It must be pointed out, however, that these autopsies have typically been conducted only on the most severe cases, since these children often have enough problems that they do not survive. The interested reader on the pathological changes that occur in FAS is referred to the following articles. References Clarren, S. K. (1986). Neuropathology in fetal alcohol syndrome. In J. R. West (Ed.), Alcohol and Brain Development (pp. 158-166). New York: Oxford University Press. Roebuck, T.M., Mattson, S.N., and Riley, E.P. (1998). A review of the neuroanatomical findings in children with fetal alcohol syndrome or prenatal exposure to alcohol. Alcoholism: Clinical and Experimental Research, 22 (2),339-344.
- Background One anomaly that has been seen in FAS is agenesis of the corpus callosum. While not common, it occurs in FAS cases (~6%) more frequently than in the general population (0.1%) or in the developmentally disabled population (2-3%). In fact it has been suggested that FAS may be the most common cause of agenesis of the corpus callosum. In the top left picture, is a control brain. The other images are from children with FAS. In the top middle the corpus callosum is present, but it is very thin at the posterior section of the brain. In the upper right the corpus callosum is essentially missing. The bottom two pictures are from a 9 year old girl with FAS. She has agenesis of the corpus callosum and the large dark area in the back of her brain above the cerebellum is a condition known as coprocephaly. It is essentially empty space. Most children with FAS do have a corpus callosum, although it may be reduced in size. The reduction in size occurs primarily in the front and rear portions (genu and splenium). One interesting item is that this same pattern of reduction in the genu and splenium has been found in ADHD children. The behavioral problems seen in FAS frequently are similar to those seen in ADHD. References Mattson, S. N., Jernigan, T. L., & Riley, E. P. (1994a). MRI and prenatal alcohol exposure. Alcohol Health & Research World, 18(1), 49-52. Mattson, S. N., & Riley, E. P. (1995). Prenatal exposure to alcohol: What the images reveal. Alcohol Health & Research World, 19(4), 273-277. Riley, E. P., Mattson, S. N., Sowell, E. R., Jernigan, T. L., Sobel, D. F., & Jones, K. L. (1995). Abnormalities of the corpus callosum in children prenatally exposed to alcohol. Alcoholism: Clinical and Experimental Research, 19(5), 1198-1202.
- Background FAS is only the tip of the iceberg in terms of outcomes. In fact, only a minority (10-40%) of the children of chronic alcoholic women are diagnosed with FAS. What makes some individuals more susceptible than others?. What are the risk factors associated with prenatal alcohol exposure? There are a number of factors that may contribute to increased risk to the adverse effects of prenatal alcohol. First, the higher the dose of alcohol, the greater the likelihood that the child will exhibit fetal alcohol effects. The pattern of exposure is also important. Both human and animal studies have found that binge drinking (drinking a large amount of alcohol in a short period of time), which produces high blood alcohol levels, is more damaging to the fetus than chronic alcohol exposure that produces lower blood alcohol levels. Thus, peak blood alcohol level may be an important factor. In addition, the developmental timing of alcohol exposure may influence the outcome. For example, the facial features associated with prenatal alcohol treatment appear to be related to alcohol exposure during the first trimester. Obviously, as different organs undergo development at different times, when the embryo or fetus is exposed is going to be important in determining the outcome. The brain undergoes a very prolonged developmental course and therefore, may be susceptible to fetal alcohol effects throughout gestation. In addition, genetic factors, nutritional factors, parity, and synergistic reaction with other drugs may influence the effects of prenatal alcohol exposure. It is important to realize that some fetal alcohol effects might occur even before a women realizes she is pregnant.
- Trauma causes significant changes to the “hardware” of the brain. Interestingly, these changes are gender-specific. Male infants that are neglected in the first 2 years of life have more profound physical brain changes than female infants. Conversely, female infants, toddlers, and children that are subjected to repeated sexual abuse have more severe physical brain changes.
- These neuroimaging techniques have revolutionized the neuroscience of abnormal childhood behavior essentially “overnight”. fMRI is very “child-friendly” as it does not expose pediatric patients to dangerous radiation and can measure functional activity in the brain while children are awake and completing certain tasks, such as reading. Despite the amazing advances in this field, we are still not able to use these procedures to help us diagnose problems in an individual child. However, soon we will be able to order an fMRI scan for a challenging child and the results will definitely help us decide what is the most appropriate treatment for that child.
- Neuroimaging by 3 separate techniques has demonstrated physiological differences in the brains of patients with ADHD Functional magnetic resonance imaging conducted while subjects performed the counting Stroop task has shown that normal adults show increased blood flow in the anterior cingulate cortex during this task. Patients with ADHD, by contrast, failed to increase blood flow in this structure under the same conditions [Bush 1999] This indicates that during cognitive conflict, more ADHD patients fail to activate the anterior cingulate cortex than do controls PET scanning has been used to examine cerebral metabolism, which is a measure of neuronal activity The results of these studies have shown that adults with ADHD have decreased cerebral metabolism compared with controls [Zametkin 1990] SPECT imaging has been used to visualize the DAT dopamine transporter in the human brain Three studies have shown that untreated adults with ADHD have increased binding of DAT protein compared with controls [Krause 2000] This increase may result in accelerated re-uptake leading to reduced dopamine in the synaptic cleft [Dresel 2000 p1522]