Git Disorders2( Need To Review Changes)
•Télécharger en tant que PPT, PDF•
9 j'aime•3,841 vues

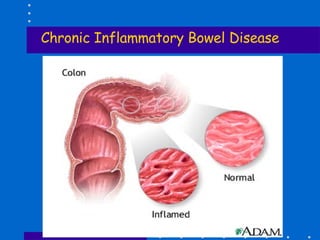
![Chronic Inflammatory Bowel Disease ,[object Object],[object Object],[object Object],[object Object],[object Object],[object Object],[object Object],[object Object],[object Object],Diagnostic test : x-ray, sigmoidoscopy, colonoscopy, occult blood in the stool, fecalysis – pus, mucus](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Git Disorders2( Need To Review Changes)
Similaire à Git Disorders2( Need To Review Changes) (20)
Dernier
Dernier (20)
Git Disorders2( Need To Review Changes)
- 1. Chronic Inflammatory Bowel Disease
- 12. Management of Chronic Inflammatory Bowel Disease
- 13. Diverticulum
- 42. GRADE I - bleeding on defecation, - no prolapse GRADE II – there’s prolapse but reduce spontaneously
- 43. GRADE III – with prolapse and reduced manually GRADE IV – cannot be reduced, incarcerated
- 52. Etiology and Risk factors (cont.) B. Neurogenic Factor Paralytic Ileus – lack of peristaltic activity - prevents forward flow of intestinal contents - commonly occurs after abdominal surgery C. Vascular Factors - when the blood supply to any part of the body is interrupted, the part ceases to function 1. Complete occlusion ( Mesenteric infarction) Mesenteric thrombosis - usual cause is an embolus - causes intense abdominal pain –-- due to ischemia bowel necrosis and gangrene and sepsis - other s/sx: fever, WBC, signs of shock - surgical intervention must be done immediately 2. Partial occlusion (Abdominal angina) - usually results from atherosclerosis of the mesenteric arteries - pain develop 15-30 mins after eating - need for O2 - manifestation arise when interruption in blood flow/supply is sufficient to compromise bowel function
- 61. Duke’s Classification of Colorectal Cancer Stage A: confined to bowel mucosa- 5 year survival rate Stage B: invading muscle wall Stage C: lymph node involvement Stage D: metastases
- 77. Colostomy Care: a. skin care - use of effective skin barriers or wafers to prevent skin irritation; cleanse with mild soap and water using cotton cloth b. odor control - avoid foods known to cause odor; dairy products, fish, eggs, and cabbage; use of pulverized charcoal, sodium bicarbonate, deodorant tablet c. control of gas -avoid carbonated beverages and gas forming foods d. diet - avoid overeating; chew food thoroughly; prevent diarrhea or constipation e. colostomy irrigation- to stimulate peristalsis; to establish a regular pattern of evacuation
- 81. Functions of the Liver(cont.) 3. Bilirubin Metabolism Hemoglobin Globin Heme Iron Protoporphyrin indirect or converted by liver enzyme unconjugated bilirubin glucoronyl transferase (fat-soluble, cannot be excreted by the kidneys) direct or conjugated bilirubin (water soluble) secreted in the bile to the duodenum reabsorbed by the liver bilirubin metabolized to urobilinogen excreted into the urine (by bacterial action) excreted into the feces as stercobilin
- 102. Viral Hepatitis 4 types: Hepatitis A, Hepatitis B, non-A, non-B hepatitis, Delta hepatitis
- 135. Cholesterol Stones
- 136. PIGMENT STONES
- 152. Acute Pancreatitis (cont.) Summary of major Pathologic events that occur in Acute Pancreatitis Altered glucose Stress response Metabolism cardiac (hyperglycemia) contractility Release of Acute Pancreatitis release of Insulin kinin Vasodilation (activated by trypsin) Obstruction of edema, distention of Shock bile flow capsule, obstruction of pancreatic flow Exudate of blood and protein into Hypovolemia Altered bilirubin peritoneal space metabolism Pain Peritonitis gastrointestinal Fever function