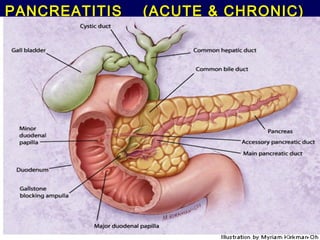
Pancreatitis (acute and chronic )
•
14 j'aime•8,439 vues

Lecture By Dr.Wael Alsadani ER Resident.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Pancreatitis (acute and chronic )
Similaire à Pancreatitis (acute and chronic ) (20)
Plus de MEEQAT HOSPITAL
Plus de MEEQAT HOSPITAL (20)
Dernier
Dernier (20)
Pancreatitis (acute and chronic )
- 1. PANCREATITIS (ACUTE & CHRONIC) 90
- 2. 1-Manage severe acute pancreatitis ► A 34-year-old woman ► is evaluated for continued severe mid-epigastric pain that radiates to the back-nausea-vomiting………5 days after being hospitalized for acute alcohol-related pancreatitis ► She has not been able eat or drink and has not had a bowel movement since being admitted ► On physical examination the temperature is 38.2 °C -blood pressure is 132/84 mm Hg-pulse rate is 101/min-respiration rate is 20/min-no scleral icterus or jaundice-abdomen is distended and diffusely tender with hypoactive bowel sounds
- 3. ► CT scan of the abdomen shows a diffusely edematous pancreas with multiple peripancreatic fluid collections, and no evidence of pancreatic necrosis Which of the following is the most appropriate next step in the management of this patient? A- Enteral nutrition by nasojejunal feeding tube B-Intravenous imipenem C-Pancreatic débridement D-Parenteral nutrition
- 4. ► Enteral feeding is the preferred route of providing nutrition in patients with severe acute pancreatitis ► This patient has moderate to severe acute pancreatitis and after 5 days remains febrile, continues to be in pain, and cannot take in any oral nutrition ► The patient will likely have an extended period before being able to take in oral nutrition ► Two routes are available for providing nutrition in patients with severe acute pancreatitis enteral nutrition-parenteral nutrition ► Enteral nutrition is provided through a feeding tube ideally placed past the ligament of Treitz so as not to stimulate the pancreas ► Parenteral nutrition is provided through large peripheral or central intravenous line ► Enteral nutrition is preferred over parenteral nutrition because of its lower complication rate……..especially a lower infection rate ► Enteral nutrition is associated with a significantly lower incidence of infections-reduced surgical interventions to control complications of pancreatitis-reduced length of hospital stay-faster attenuation of inflammation-fewer septic complications
- 5. ► Imipenem therapy is only helpful in acute pancreatitis when there is evidence of pancreatic necrosis ► Pancreatic necrosis is diagnosed by contrast-enhanced CT scan……….that shows nonenhancing pancreatic tissue ► In patients with noninfected pancreatic necrosis, prophylactic antibiotics may↓incidence of sepsis-↓systemic complications (for example, respiratory failure)-↓local complications (for example, infected pancreatic necrosis or pancreatic abscess) ► antibiotic use in acute pancreatitis of mild to moderate severity shown no benefit from-but may lead to development of nosocomial infections with resistant pathogens ► Similarly pancreatic débridement is recommended only in infected pancreatic necrosis
- 6. 2-Diagnose pancreatic necrosis ► A 44-year-old man with a long history of alcohol abuse is evaluated on the sixth day of hospitalization for acute pancreatitis ► On admission to the hospital he was afebrile-blood pressure was 150/88 mm Hg- pulse rate was 90/min-respiration rate was 16/min ► Abnormal findings were limited to the abdomen, which was flat and tender to palpation -without peritoneal signs-Bowel sounds were normal ► Plain abdominal and chest radiographs were normal ► Abdominal ultrasonography revealed a diffusely enlarged, hypoechoic pancreas -without evidence of gallstones or dilated common bile duct ► He was treated with aggressive intravenous hydration and opioid analgesia ► For the past 2 days, the patient has had repeated febrile episodes-persistent severe abdominal pain-increasing shortness of breath
- 7. ► On physical examination T 38.6 °C -BP 98/60 mm Hg - pulse rate is 112/min- RR 22/min-oxygen saturation is 92% with the patient breathing oxygen 3 L/min-Breath sounds are decreased at the base of both lungs-The abdomen is distended and diffusely tender with hypoactive bowel sounds ► Laboratory studies reveal leukocyte count of 19,800/µL-creatinine 1.4 mg/dL -amylase 388 U/L-lipase 842 U/L. ► Which of the following is the most appropriate next step in the evaluation of this patient? A- CT scan of the abdomen with intravenous contrast B-Endoscopic retrograde cholangiopancreatography C-Endoscopic ultrasonography D-Stool chymotrypsin
- 8. ► CT scan of the abdomen with intravenous contrast is the most sensitive test to diagnose pancreatic necrosis ► Pancreatic necrosis should be suspected in a patient with severe acute pancreatitis ………..whose condition is not improving or is worsening after 5 days or more of treatment ► Pancreatic necrosis on CT scan can be identified as unenhanced areas of the pancreas ► pancreatic necrosis in the setting of acute pancreatitis cannot detect by endoscopic retrograde cholangiopancreatography or endoscopic ultrasonography
- 9. ► Stool chymotrypsin can be measured when chronic pancreatitis is suspected………..to help evaluate for decreased pancreatic function ► Pancreatic necrosis is the most important predictor of poor outcome in acute pancreatitis ► Patients who develop pancreatic necrosis should be given antibiotic prophylaxis, usually with imipenem ► The necrosis should be sampled for the presence of infection………….and if infection is present, surgical débridement is recommended
- 10. 3-Manage gallstone pancreatitis ► A 55-year-old woman ► is evaluated in the hospital for a 2-day history of epigastric abdominal pain - nausea and vomiting - anorexia ► The patient has no significant medical history ► takes no medications ► On physical examination temperature is 38.0 °C - blood pressure is 124/76 mm Hg - pulse rate is 99/min - respiration rate is 16/min - There is scleral icterus and a slight yellowing of the skin - mid-epigastric and right upper quadrant tenderness - no palmar erythema, spider angiomata, or other evidence of chronic liver disease
- 11. ► Abdominal ultrasonography shows a biliary tree with a dilated common bile duct of 12 mm and cholelithiasis but no choledocholithiasis ► Which of the following is the most appropriate next step in the management of this patient? A-CT scan of the abdomen and pelvis with pancreatic protocol B- Endoscopic retrograde cholangiopancreatography C-Hepatobiliary iminodiacetic acid (HIDA) scan D-Magnetic resonance cholangiopancreatography
- 12. ► In patients with gallstone pancreatitis and evidence of biliary obstruction, endoscopic retrograde cholangiopancreatography and stone removal will reduces morbidity and mortality…………..by reducing the risk of biliary sepsis ► This patient has a classic presentation of acute pancreatitis with the acute onset of epigastric abdominal pain, nausea, and vomiting - associated with markedly elevated pancreatic enzymes ► The presence of stones in the gallbladder- dilated bile duct - elevated aminotransferase levels…………….highly suggest gallstones as the cause of pancreatitis ► The presence of scleral icterus – jaundice - elevated bilirubin level…….suggest continuing bile duct obstruction ► Abdominal ultrasonography has a sensitivity of only 50% to 75% for choledocholithiasis ► a common duct stone should be suspected in the correct clinical situation even when ultrasonography does not show a stone ► Endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy and stone removal…..is the most appropriate procedure in patients with acute gallstone pancreatitis and with imaging and biochemical evidence of biliary obstruction from a common duct stone
- 13. ► The procedure can document the diagnosis of choledocholithiasis and remove the gallstones………..which lessens the morbidity and mortality due to biliary sepsis. ► CT scan acute pancreatitis and the presence of a common duct stone=sensitivities ranging from 80% to 100% ► magnetic resonance cholangiopancreatography (MRCP) will show acute pancreatitis and the presence of a common duct stone=sensitivities ranging from 80% to 100% ► ERCP = diagnosis of choledocholithiasis ► Biliary scintigraphy may show obstruction of the cystic or common bile duct…..but will not determine the cause ► However CT - biliary scintigraphy and MRCP………are not be therapeutic for bile duct stones
- 14. 4-Evaluate acute pancreatitis ► A 42-year-old woman ► is evaluated in the emergency department for the acute onset of epigastric pain …that radiates to the back …and is associated with nausea and vomiting ► The patient had previously been healthy ► no history of alcohol or tobacco use ► Her only medication is an oral contraceptive pill ► On physical examination=temperature is 37.2 °C - blood pressure is 158/90 mm Hg - pulse rate is 101/min - respiration rate is 20/min - no scleral icterus or jaundice ► The abdomen is distended with mid-epigastric tenderness - no rebound or guarding - hypoactive bowel sounds
- 15. ► Radiography of the abdomen shows mild ileus ► Which of the following is the most appropriate next step in the evaluation of this patient? A-CT scan of the abdomen and pelvis B-Endoscopic retrograde cholangiopancreatography C-Esophagogastroduodenoscopy D- Ultrasonography of the abdomen
- 16. ► Gallstones=most common cause of acute pancreatitis in the United States - diagnosed with abdominal ultrasonography ► The diagnosis of pancreatitis relies heavily on the serum amylase and lipase…….which are elevated in 75% to 90% of patients ► Serum lipase is more specific and stays elevated longer than amylase ► The two most common causes of acute pancreatitis in the United States are alcohol and gallstones ► this patient who does not consume alcohol , so gallstones are the most likely cause of acute pancreatitis as shown by the pattern of liver enzymes ► Abdominal ultrasonography is the most sensitive test for detecting the presence of gallstones and ductal dilation - can provide indirect evidence for the presence of a retained common duct stone - Ultrasonography = has no risk + widely available + inexpensive
- 17. ► CT scan is less sensitive than ultrasonography for the detection of cholelithiasis ► CT with contrast is indicated in patients with moderate or severe pancreatitis = to confirm the diagnosis - to grade the severity of pancreatitis - to diagnose local complications such as pancreatic necrosis , pseudocyst & abscess ► Magnetic resonance cholangiopancreatography is used if there is a contraindication to intravenous radiocontrast ► Endoscopic retrograde cholangiopancreatography (ERCP) is the most sensitive test for choledocholithiasis - can provide direct treatment by removing common duct stones ► ERCP is indicated in patients with - persisting pancreatitis - persistent elevation of aminotransferase levels - dilated bile ducts suggesting the presence of retained bile duct stones - can do stone extraction with biliary sphincterotomy so improves the outcome, prevents further attacks of acute biliary pancreatitis, and reduces pancreatitis ► But in this patient there is not enough evidence yet that a common duct stone is still present to perform this more invasive test before ultrasonography ► Upper endoscopy = no role in determining the cause of acute pancreatitis
- 18. 5-Diagnose chronic pancreatitis ► A 51-year-old man ► is evaluated for an 8-month history of mid-epigastric pain that is worse after eating - six to eight bowel movements a day usually occurring after a meal - loss of 6.8 kg over the past 6 months ► The patient drinks six to eight cans of beer a day ► He takes no medications ► On physical examination BMI 21 - normal bowel sounds - mid-epigastric tenderness - no hepatosplenomegaly or masses ► Rectal examination reveals brown stool - negative occult blood ► The remainder of the examination is normal ► Plain radiograph of the abdomen shows a normal bowel gas pattern and is otherwise normal
- 19. Which of the following tests is most likely to establish the diagnosis in this patient? A-Colonoscopy B- CT scan of the abdomen C-Measurement of serum antiendomysial antibodies D-Stool for leukocytes, culture, ova, and parasite
- 20. ► Patients with chronic pancreatitis=the three classic findings in chronic pancreatitis are abdominal pain that is usually mid-epigastric - postprandial diarrhea - and diabetes mellitus secondary to pancreatic endocrine insufficiency ► This patient has chronic pancreatitis secondary to alcohol abuse………… SO has resulted in malabsorption ► Malabsorption occurs in patients with chronic pancreatitis when approximately 80% of the pancreas is destroyed ► because the damaged pancreatic gland is no longer producing the pancreatic exocrine enzymes to absorb food so malabsorption occurs that presents with diarrhea and steatorrhea - weight loss - deficiencies of fat- soluble vitamins ► Patients with a typical presentation may not need additional testing ► However, most patients with chronic pancreatitis have only nonspecific abdominal pain ………….so require diagnostic radiographic imaging studies
- 21. ► The presence of pancreatic calcifications on radiographs confirms the diagnosis ► Plain films of the abdomen will show pancreatic calcifications in approximately 30% of patients…………so confirms the diagnosis ► But most patients require abdominal CT scans, which are able to detect pancreatic calcification in up to 90% of patients ► CT scanning can also exclude other causes of pain ► Radiographic evidence of pancreatic ductal dilation – pseudocysts - or mass lesions ………….may also help identify the cause of pain and determine the type of therapy ► Antiendomysial antibodies are a marker for celiac disease ……….. but celiac disease is unlikely in this patient with an evident history of pancreatic malabsorption
- 22. ► colonoscopy is indicated as a screening tool for asymptomatic patients beginning at the age of 50 years - and for patients with a change in bowel habits and weight loss ► But this patient’s history suggests pancreatic malabsorption so colonoscopy is less likely than abdominal CT scan to confirm the diagnosis ► Stool studies are appropriate fordetermining the cause of an acute infectious diarrhea……but this patient has had diarrhea for 8 months …………..so infectious diarrhea is not usually associated with such a degree of weight loss
- 23. 6-Diagnose chronic pancreatitis ► A 42-year-old man ► is evaluated in the hospital for a 1-year history of postprandial abdominal pain that radiates to the back -worse after eating - and is associated with nausea ► He has no (vomiting -weight loss -change in bowel habits) ► The patient has had at least five alcohol-containing drinks a day for 20 years ► he has reduced his intake in the past year because of continued abdominal pain ► On physical examination vital signs are normal - BMI is 24 - mild epigastric tenderness - no guarding or rebound - normal bowel sounds ► Laboratory studies reveal normal complete blood count - normal fasting glucose - normal liver chemistry tests - amylase is 221 U/L and lipase 472 U/L. ► esophagogastroduodenoscopy , AXR, ultrasonography, and CT scan of the abdomen are normal ► Which of the following is the most appropriate next step in the evaluation of this patient? A-Biliary scintigraphy B-Colonoscopy C- Endoscopic retrograde cholangiopancreatography D-easurement of stool elastase
- 24. ► Endoscopic retrograde cholangiopancreatography is the most sensitive imaging test for chronic pancreatitis ► diagnosis of chronic pancreatitis in a patient with early disease can be difficult ► No blood or stool tests are currently available for the accurate diagnosis of early chronic pancreatitis ► This patient’s pain is most likely secondary to chronic pancreatitis with minimally elevated pancreatic enzymes and a history of harmful drinking ► The patient has no evidence of exocrine or endocrine insufficiency and thus likely has early chronic pancreatitis ► Normal liver enzymes, normal upper endoscopy, and a normal abdominal ultrasonography and CT scan of the abdomen make biliary causes and peptic ulcer disease………less likely the cause of pain ► Endoscopic retrograde cholangiopancreatography (ERCP) has a sensitivity of nearly 95% for chronic pancreatitis - can show ductal dilation,strictures and irregularity in both the main duct and its side branches
- 25. ► CT scan of the abdomen =has a sensitivity of up to 90% for diagnosing chronic pancreatitis and should be ordered with thin cuts of the pancreas to improve sensitivity ► Endoscopic ultrasonography=may also be used to diagnose chronic pancreatitis - sensitivities is equal to ERCP for moderate and advanced chronic pancreatitis - but with lower sensitivity and specificity for mild and early chronic pancreatitis ► Magnetic resonance cholangiopancreatography does not have sensitivities or specificities that match ERCP in the diagnosis of mild and early chronic pancreatitis and cannot be routinely recommended ► Biliary scintigraphy is used to diagnose acute cholecystitis - but does not have a role in diagnosing chronic pancreatitis ► Stool elastase can be abnormal in patients with more advanced chronic pancreatitis=particularly those who have malabsorption - but stool elastase has poor sensitivity in patients with early chronic pancreatitis ► Colonoscopy has a low yield in patients with upper abdominal pain
- 26. 7-Treat chronic pancreatitis with pancreatic duct stones ► A 38-year-old man is evaluated for a 2-month history of progressive mid-epigastric pain that is worse after eating - postprandial nausea - 4.6-kg weight loss ► The patient has a 5-year history of chronic pancreatitis ► has six alcohol-containing drinks a day ► His medications are Amitriptyline - oral morphine - and pancreatic enzyme supplements ► On physical examination BMI 20 - appears to be in mild distress - There is epigastric tenderness without rebound or guarding - The liver is slightly enlarged, but there are no palpable masses ► Laboratory studies reveal normal complete blood count - serum amylase of 175 U/L - lipase of 333 U/L ► CT scan of the abdomen and pelvis shows - multiple pancreatic calcifications - a calcified stone in the head of the pancreas within the main pancreatic duct - dilation of the duct in the body and tail of the gland ► In addition to alcohol cessation, which of the following is the most appropriate management for this patient? A-Celiac nerve block B- Endoscopic retrograde cholangiopancreatography with removal of stones C-Increasing the dose of pancreatic enzymes D-Pancreatoduodenectomy
- 27. ► Endoscopic treatment of pain in chronic pancreatitis is performed by removing pancreatic duct stones and placing stents in pancreatic duct strictures ….to decrease pancreatic duct pressure ► Patients with chronic pancreatitis must avoid alcohol ► Patients who continue to drink alcohol have an increase in painful attacks and mortality ► Pain in chronic pancreatitis results from chronic inflammation - chronic noxious stimulation of the nerves to the pancreas - and increased pancreatic intraductal pressure secondary to pancreatic duct stones, calcifications, or strictures ► Large stones in the pancreatic duct can be - crushed with extracorporeal shock wave lithotripsy - Then endoscopic retrograde cholangiopancreatography can remove the stones and place stents in pancreatic duct strictures to decrease pancreatic duct pressure…….so symptom improvement in 11% to 75% of patients and resolution of stricture in 10% to 50%
- 28. ► A surgical pancreatoduodenectomy (Whipple procedure) can be performed to relieve pain - but is effective only in patients who have disease limited to the head of the pancreas and who have failed to respond to medical and endoscopic therapy ► A surgical procedure to divert the pancreatic duct into the small intestine =The procedure involves removing pancreatic tissue that overlies the ductal system in the head of the pancreas - has been used widely in the treatment of patients with a chronic pancreatitis and is effective in many patients…..but a less invasive procedure is preferred to surgical intervention as the next management step ► Celiac nerve block =has been used to treat chronic pancreatitis pain - but is considered by many experts to be an unproved therapy and even in patients who respond, pain returns in 2 to 6 months and significant procedural complications have been reported - Furthermore, it would not be the first procedure of choice in a patient with a pancreatic ductal stone and evidence of obstruction ► Pancreatic enzyme supplements are not effective for pain control in chronic pancreatitis
- 29. THANK YOU DR: WAEL AHMED EL-SADANY ER resident