ANS Pharmacology-Cholinergic Agents
•
66 j'aime•6,129 vues

http://www.imhotepvirtualmedsch.com/

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à ANS Pharmacology-Cholinergic Agents
Similaire à ANS Pharmacology-Cholinergic Agents (20)
Plus de Imhotep Virtual Medical School
Plus de Imhotep Virtual Medical School (20)
Dernier
Dernier (20)
ANS Pharmacology-Cholinergic Agents
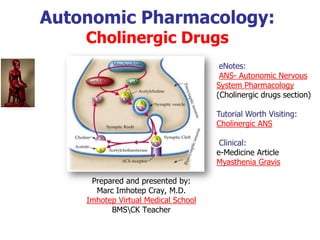
- 1. Autonomic Pharmacology: Cholinergic Drugs Prepared and presented by: Marc Imhotep Cray, M.D. Imhotep Virtual Medical School BMSCK Teacher eNotes: ANS- Autonomic Nervous System Pharmacology (Cholinergic drugs section) Tutorial Worth Visiting: Cholinergic ANS Clinical: e-Medicine Article Myasthenia Gravis
- 2. 2 Reference Resource Principles of Pharmacology: The Pathophysiologic Basis of Drug Therapy Cairo CW, Simon JB, Golan DE. (Eds.); LLW 2012
- 3. 3 Cholinergic Biosynthesis Acetylcoline is formed from two precursors: choline: which is derived from dietary and intraneuronal sources acetyl coenzyme: which is made from glucose in mitochondria of neurons Acetylcholine is synthesized from choline and acetyl-CoA by the enzyme choline acetyl transferase (ChAT) to form acetylcholine, which is immediately stored in small vesicular compartments closely attached to cytoplasmic side of presynaptic membranes ChAT is a selective marker for cholinergic neurons
- 4. 4 Cholinergic Biosynthesis 1) Synthesis of acetylcholine (ACh) from acetyl CoA and choline 2) Storage of ACh in synaptic vesicles 3) Release of ACh ( fusion of synaptic vesicle with presysnaptic membrane and release of ACh into the synapse) 4) Action of ACh by binding to and activating receptors (nicotinic in autonomic ganglia and neuromuscular junction and, muscarinic in many sites) 5) Inactivation by enzymatic breakdown of ACh by acetylcholinesterase (AChE) located in the synapse. ACh is degraded in the synaptic cleft by acetylcholinesterase to choline and acetate
- 5. 5 Cholinergic Agents-Direct Acting and Indirect Acting Choline Esters Acetylcholine Bethanechol (Urecholine) Carbachol Methacholine (Provocholine) Alkaloids Muscarine Pilocarpine (Pilocar) There are three main types of cholinesterase: Short-acting: edrophonium medium-acting: neostigmine (2-4h), pyridostigmine (3- 6h) physostigmine irreversible: organophosphates, dyflos, ecothiopate Agents-Direct Acting Indirect Acting
- 6. 6 Spectrum of Action of Choline Esters Location of cholinergic synapses mainly determine the spectrum of action of acetylcholine and choline esters Cholinergic Synaptic Sites autonomic effector sites: innervated by post-ganglionic parasympathetic fibers some CNS synapses autonomic ganglia and the adrenal medulla skeletal muscle motor endplates (motor nerves)
- 7. 7 Spectrum of Action of Choline Esters(2) Cholinergic influences are prominent in many organ systems: Choline Ester Sensitivity to ACHE Cardio- vascular Gastrointe stinal Urinary Bladder Eye (Topical) Atropine Sensitive Activity at Nicotinic Sites Acetylcholine Methacholine Carbachol No Bethanechol No ? ? No
- 8. 8 Spectrum of Action of Choline Esters(3) Cholinergic Receptors: Cholinergic refers to responses in various systems to the natural transmitter molecule Acetylcholine (ACh) If one looks at a set of responses where ACh is the normal transmitter, observation has shown that those same responses are differently sensitive to the extrinisic molecules Nicotine and Muscarine Nicotine comes from tobacco, Muscarine comes from certain mushrooms
- 9. 9 Spectrum of Action of Choline Esters(4) Based on the different sensitivities shown above, Cholinergic receptors are subclassified into two categories, Nicotinic and Muscarinic, named for the extrinsic compounds that stimulate only that category
- 10. 10 Spectrum of Action of Choline Esters(5) Nicotinic Receptors Stimulated by ACh and nicotine, not stimulated by muscarine Found at all ganglionic synapses Also found at neuromuscular junctions Blocked by hexamethonium
- 11. 11 Spectrum of Action of Choline Esters(6) Nicotinic Receptors The physiological responses to stimulation and block are complex since both sympathetic and parasympathetic systems are affected The final response of any one organ system depends on which system has a stronger tonic influence Example: Under normal circumstances, the heart receives more parasympathetic influence than sympathetic Ganglionic blockade would lower parasympathetic influence more than sympathetic, and thus heart rate would increase
- 12. 12 Spectrum of Action of Choline Esters(6) Muscarinic Receptors Stimulated by ACh and muscarine, not stimulated by nicotine Found at target organs when ACh is released by post-ganglionic neurons (all of parasympathetic, and some sympathetic) Stimulated selectively by Muscarine and Bethanechol etc. Blocked by Atropine
- 13. 13 Spectrum of Action of Choline Esters(7) Muscarinic Receptors Stimulation causes: Increased sweating Decreased heart rate Decreased blood pressure due to decreased cardiac output Bronchoconstriction and increased bronchosecretion Contraction of the pupils, and contraction of ciliary body for near vision Tearing and salivation Increased motility and secretions of the GI system Urination and defecation Engorgement of genitalia
- 14. 14 Cholinergic Receptors: Subtypes, Tissues, Responses and Molecular Mechanisms Muscarinic Receptor Coupling Mechanisms Five types of cholinergic receptors have been identified by molecular cloning methods. The five muscarinic receptor subtypes, M1 - M5, are associated with specific anatomical sites For example: M1 -ganglia; secretory glands M2 - myocardium, smooth muscle M3 , M4 :smooth muscle, secretory glands
- 15. 15 Cholinergic Receptors: Subtypes, Tissues, Responses and Molecular Mechanisms Nicotinic Muscle Receptor Antagonists Tissue Responses Molecular Aspects Tubocurarine alpha-bungarotoxin Neuromuscular Junction Membrane Depolarization leading to muscle contraction Nicotinic (muscle) receptor's cation ion channel opening
- 16. 16 Cholinergic Receptors: Subtypes, Tissues, Responses and Molecular Mechanisms(2) Nicotinic Neuronal Receptor Antagonists Tissue Responses Molecular Aspects Mecamylamine (Inversine) Autonomic Ganglia Depolarization: postsynaptic cell activation Nicotinic (muscle) receptor's cation ion channel openingAdrenal Medulla Catecholamine secretion CNS unknown
- 17. 17 Cholinergic Receptors: Subtypes, Tissues, Responses and Molecular Mechanisms(3) Muscarinic Type M1 Antagonist Tissue Responses Molecular Aspects Atropine Pirenzepine (more selective) Autonomic Ganglia Depolarization (late EPSP) Stimulation of Phospholipase C (PLC): activation of inositol-1,4,5 triphosphate (IP3 ) and diacylglycerol (DAG) leading to increased cytosolic Ca2+ CNS Unknown
- 18. 18 Cholinergic Receptors: Subtypes, Tissues, Responses and Molecular Mechanisms(4) Muscarinic Type M2 Tissue (Heart) Responses Molecular Aspects SA node decreased phase 4 depolarization; hyperpolarization K+ channel activation through ß-gamma Gi subunits; Gi -mediated inhibition of adenylyl cyclase which decreases intracellular Ca2+ levels. (Gi can inhibit directly Ca2+ channel opening) Atrium decreased contractility; decreased AP duration AV node decreased conduction velocity Ventricle decreased contractility
- 19. 19 Signal Transduction: Comparison of Muscarinic and Nicotinic Receptors Nicotinic Receptors Ligand-gated ion channels Agonist effects blocked by tubocurarine Receptor activation results in: rapid increases of Na+ and Ca2+ conductance deplorization excitation Subtypes based on differing subunit composition: See Muscle and Neuronal Classification Discussed in previous slides
- 20. 20 Signal Transduction: Comparison of Muscarinic and Nicotinic Receptors Muscarinic Receptors G-protein coupled receptor system Slower responses Agonist effects blocked by atropine At least five receptor subtypes have been described by molecular cloning
- 21. 21 Muscarinic Receptors: Second Messenger Systems Activation of IP3, DAG cascade DAG may activate smooth muscle Ca2+ channels IP3 releases Ca2+ from endoplasmic and sarcoplasmic reticulum Increase in cGMP Increase in intracellular K+ by cGMP-K+ channel binding inhibition of adenylyl cyclase activity (heart)
- 22. 22 Muscarinic Receptors: Second Messenger Systems(2)
- 23. 23 Direct vs. Indirect-Acting Cholinomimetics A direct-acting cholinomimetic drug produces its pharmacological effect by receptor activation An indirect-acting drug inhibits acetylcholinesterase, thereby increasing endogenous acetylcholine levels, resulting in increased cholinergic response.
- 24. 24 Pharmacological Effects of Cholinomimetics 1)Vasodilation This effect is mediated by muscarinic receptor activation and is especially prominent in the salivary gland and intestines
- 25. 25 Pharmacological Effects of Cholinomimetics (2) Vasodilation cont. The vascular response is due to endothelial cell nitric oxide (NO) release following agonist interactions with endothelial muscarinic receptor Increased NO activates guanylate cyclase which increases cyclic GMP concentrations
- 26. 26 Pharmacological Effects of Cholinomimetics (3) Vasodilation cont. Subsequent activation of a Ca2+ ion pump reduces intracellular Ca2+ Reduction in intracellular Ca2+ causes vascular smooth muscle relaxation Ca2+ complexes with calmodulin activating light- chain myosin kinase Increased cGMP promotes dephosphorylation of myosin light-chains. Smooth-muscle myosin must be phosphorylated in order to interact with actin and cause muscle contraction.
- 27. 27 Nitric Oxide (NO) and Vasodilitation From: http://www.nature.com/nature/journal/v396/n6708/fig_tab/396213a0_F1.html
- 28. 28 Pharmacological Effects of Cholinomimetics(4) 2)Negative chronotropic effect (Decrease in heart rate) Decreases phase 4 (diastolic depolarization) As a result, it takes longer for the membrane potential to reach threshold. Mediated by M2 muscarinic receptors
- 29. 29 Pharmacological Effects of Cholinomimetics(5) 3) Decreased SA nodal and AV nodal conduction velocity Excessive vagal tone may induce bradyarrhythmias including partial or total heart block (impulses cannot pass through AV node to drive ventricular rate in this case, the idioventricular or intrinsic ventricular rate must maintain adequate cardiac output Transmission through the AV node is especially dependent on Ca2+ currents. ACh decreases calcium currents in the atrioventricular node
- 30. 30 Pharmacological Effects of Cholinomimetics(6) 4) Negative inotropism (decreased myocardial contractility) more prominent in atrial than ventricular tissue due to a decrease in Ca2+ inward current in ventricle, adrenergic tone dominates; at higher levels of sympathetic tone, a reduction in contractility due to muscarinic stimulation is noted Muscarinic stimulation reduces response to norepinephrine by opposing increases in cAMP in addition to reducing norepinephrine release from adrenergic terminals
- 31. 31 Clinical Uses Gastrointestinal & Genitourinary Bethanechol (Urecholine) GI smooth muscle stimulant postoperative abdominal distention paralytic ileus esophageal reflux; promotes increased esophageal motility (other drugs are more effective, e.g. dopamine antagonist (metoclopramide) or serotonin agonists (cisapride)
- 32. 32 Clinical Uses(2) Urinary bladder stimulant post-operative; post-partum urinary retention alternative to pilocarpine to treat diminished salivation secondary e.g. to radiation Carbachol not used due to more prominent nicotinic receptor activation Diagnostic tool Methacholine used for diagnostic purposes testing for bronchial hyperreactivity and asthma
- 33. 33 Clinical Uses(3) Opthalmological Uses Acetylcholine and Carbachol may be used for intraocular use as a miotic in surgery Carbachol may be used in treatment of glaucoma Pilocarpine is used in management of glaucoma and has become the standard initial drug for treating the open-angle form. Sequential administration of atropine (mydriatic) and pilocarpine (miotic) is used to break iris- lens adhesions
- 34. 34 Adverse Effects: Muscarinic Agonists Adverse Effects: Muscarinic Agonists salivation diaphoresis colic GI hyperactivity headache loss of accommodation
- 35. 35 Major contraindication to the use of muscarinic agonists Asthma: Choline esters (muscarinic agonists) can produce bronchoconstriction In the predisposed patient, an asthmatic attack may be induced Hyperthyroidism: Choline esters (muscarinic agonists) can induce atrial fibrillation in hyperthyroid patients Peptic ulcer: Choline esters (muscarinic agonists), by increasing gastric acid secretion, may exacerbate ulcer symptoms. Coronary vascular disease: Choline esters (muscarinic agonists), as a result of their hypotensive effects, can further compromise coronary blood flow
- 36. 36 Indirect-acting Cholinomimetic Drugs Acetylcholinesterase Inhibitors There are three classes of anticholinesterase agents 1. Reversible, Short-Acting Anticholinesterases 2. Carbamylating Agents: Intermediate- Duration Acetylcholinesterase Inhibitors 3. Phosphorylating Agents: Long-Duration Acetylcholinesterase Inhibitors
- 37. 37 Reversible, Short-Acting Anticholinesterases 1) edrophonium (Tensilon) and 2) tacrine (Cognex) , associate with choline binding domain The short duration of edrophonium (Tensilon) action is due to its binding reversibility and rapid renal clearance Tacrine (Cognex), being more lipophillic, has a longer duration
- 38. 38 Carbamylating Agents: Intermediate- Duration Acetylcholinesterase Inhibitors Physostigmine Neostigmine are acetylcholinesterase inhibitors that form a moderately stable carbamyl-enzyme derivative The carbamyl-ester linkage is hydrolyzed by esterase, but much more slowly compared to acetylcholine As a result, enzyme inhibition by these drugs last about 3 - 4 h (t ½ = 15 - 30 min). Neostigmine possesses a quaternary nitrogen and thus has a permanent positive charge By contrast, physostigmine is a tertiary amine
- 39. 39 Phosphorylating Agents: Long-Duration Acetylcholinesterase Inhibitors Organophosphate acetylcholinesterase inhibitors, such as diisopropyl fluorophosphate (DFP) form stable phosphorylated serine derivatives For DFP enzyme effectively does not regenerate following inhibition
- 40. 40 Phosphorylating Agents: Long-Duration Acetylcholinesterase Inhibitors(2) Furthermore, in the case of DFP, the loss, termed "aging", of an isopropyl group, further stabilizes phosphylated enzyme The application of terms "reversible" and "irreversible" depends on the duration of enzyme inhibition rather than strictly based on mechanism
- 41. 41 Organophosphate poisoning Parathion Parathion, a low volatility and aqueous-stable, organophosphate is used as an agriculural insecticide. Parathion is converted to paraoxon by mixed function oxidases. Both the parent compound and its metabolite are effective acetylcholinesterase inhibitors (P=S to P=O) Parathion probably is the most common cause of accidental organophosphate poisoning and death The phosphothioate structure is present in other common insecticides: dimpylate, fenthion, and chlorpyrifos
- 42. 42 Tx of Organophosphate poisoning-Pralidoxine Pralidoxine is a cholinesterase activator It is used as an antidote to organophosphates poisoning Unfortunately, pralidoxine does not cross the blood brain barrier to treat central effects of organophosphate poisoning It has to be given very early after poisoning as within a few hours the phosphorylated enzyme undergoes a change (aging) that renders it no longer susceptible to reactivation
- 43. 43 Clinical applications of anticholinesterases They are also used in cases of overdose with either the muscarinic antagonist, atropine, or muscle relaxants (nicotinic antagonists) Pralidoxine is a cholinesterase activator organophosphates poisoning
- 44. 44 Opthalmological Uses of Anticholinesterase Drugs When applied to conjunctiva, acetylcholinesterase inhibitors produce: constriction of the pupillary sphincter muscle (miosis) contraction of the ciliary muscle (paralysis of accommodation or loss of far vision) Loss of accommodation disappears first, while miotic effect is longer lasting During miosis, elevated intraocular pressure (glaucoma) declines due to enhanced flow of aqueous humor In glaucoma, elevation of intraocular pressure can cause damage to optic disc and blindness
- 45. 45 Gastrointestinal and Urinary Bladder Neostigmine is anticholinesterase agent of choice for treatment of paralytic ileus or urinary bladder atony Direct acting cholinomimetic drugs are also useful
- 46. 46 Myasthenia Gravis See e-Medicine Article Myasthenia Gravis Myasthenia Gravis appears to be caused by binding of anti-nicotinic receptor antibodies to nicotinic cholinergic receptor Binding studies using snake alpha- neurotoxins determined a 70% to 90% reduction of nicotinic receptors per motor endplate in myasthenic patients
- 47. 47 Myasthenia Gravis(2) Receptor number is reduced by: increased receptor turnover (rapid endocytosis) blockade of the receptor binding domain antibody damage of postsynaptic muscle membrane
- 48. 48 Myasthenia Gravis(3) Anticholinesterase, edrophonium (Tensilon), is useful in differential diagnosis for myasthenia gravis. In this use, edrophonium (Tensilon) with its rapid onset (30 s) and short duration (5 min) may cause an increase in muscle strength.
- 49. 49 Myasthenia Gravis(4) This change is due to transient increase in acetylcholine concentration at the end plate Edrophonium (Tensilon) may also be used to differentiate between muscle weakness due to excessive acetylcholine (cholinergic crisis) and inadequate drug dosing
- 50. 50 Antimuscarinic Effects on Organ Systems Central Nervous System Effects of Antimuscarinic Agents In normal doses, atropine produces little CNS effect In toxic doses, CNS excitation results in restlessness, hallucinations, and disorientation At very high doses, atropine can lead to CNS depression which causes circulatory and respiratory collapse By contrast, scopolamine at normal therapeutic doses causes CNS depression, including drowsiness, fatigue and amnesia
- 51. 51 Antimuscarinic Effects on Organ Systems Central Nervous System Effects of Antimuscarinic Agents cont. Scopolamine also may produce euphoria, a basis for some abuse potential Scopolamine may exhibit more CNS activity than atropine because scopolamine crosses the blood brain barrier more readily Scopolamine (transdermal) is effective in preventing motion sickness Antimuscarinics are used clinically as preanesthetic medication to reduce vagal effects secondary to visceral manipulation during surgery Antimuscarinics with L- DOPA are used in Parkinson's disease Extrapyramidal effects induced by some antipsychotic drugs may be treated with antimuscarinic agents
- 52. 52 Antimuscarinic Effects on Organ Systems Autonomic Ganglia and Autonomic Nerve Terminals Primary cholinergic receptor class at autonomic ganglia is nicotinic; however, muscarinic M1-cholinergic receptors are also present Muscarinic M1-ganglionic cholinergic receptor activation produce a slow EPSP that may have a modulatory role Muscarinic receptors are also located at adrenergic and cholinergic presynaptic sites where their activation reduces transmitter release Blockade of these presynaptic receptors increase transmitter release
- 53. 53 Opthalmological Muscarinic receptor antagonists block parasympathetic responses of ciliary muscle and iris sphincter muscle, resulting in paralysis of accommodation (cycloplegia) and mydriasis (pupillary dilation) Mydriasis results in photophobia, whereas cycloplegia fixes lens for far vision only (near objects appear blurred) Antimuscarinic Effects on Organ Systems
- 54. 54 Opthalmological cont. Systemic atropine at usual doses does not produce significant ophthalmic effect By contrast, systemic scopolamine results in both mydriasis and cycloplegia Note that sympathomimetic-induced mydriasis occurs without loss of accommodation Atropine-like drugs can increase intraocular pressure, sometimes dangerously, in patients with narrow-angle glaucoma Increases in intraocular pressure is not typical in wide-angle glaucoma Antimuscarinic Effects on Organ Systems
- 55. 55 Antimuscarinic Effects on Organ Systems Cardiovascular System Antagonist Tissue (Heart) Responses Molecular Aspects The dominant effect of atropine or other antimuscarinic drug administration is an increase in heart rate. This effect is mediated by M2- receptor blockade thereby blunting cardiac vagal tone. atropine SA node decreased phase 4 depolarization; hyperpolarization K+ channel activation (hyperpolarizing) through ß-gamma Gi subunits*; Gi -mediated inhibition of adenylyl cyclase* (negative inotropism) (Gi can inhibit directly Ca2+ channel opening) Atrium decreased contractility; decreased AP duration AV node decreased conduction velocity Ventricle decreased contractility Muscarinic Type M2
- 56. THE END 56