The Most Attractive Hyderabad Call Girls Kothapet 𖠋 6297143586 𖠋 Will You Mis...
Spondylolisthesis
1. Cardiff School of Engineering
Coursework Cover Sheet
Personal Details
Student No: 1056984
Family Name: Divecha First Name: Hiren
Personal Tutor: Prof Sam Evans Discipline: MMM
Module Details
Module Name: Surgical Practice Module No: ENT547
Coursework Title: Weekend 3 Assignment - Define and classify spondylolisthesis and
discuss the management of high grade slips
Lecturer: Mr S Ahuja
Submission Deadline: 3/3/2012
Declaration
I hereby declare that, except where I have made clear and full reference to the work of
others, this submission, and all the material (e.g. text, pictures, diagrams) contained in it, is
my own work, has not previously been submitted for assessment, and I have not knowingly
allowed it to be copied by another student. In the case of group projects, the contribution of
group members has been appropriately quantified.
I understand that deceiving, or attempting to deceive, examiners by passing off the work of
another as my own is plagiarism. I also understand that plagiarising another's work, or
knowingly allowing another student to plagiarise from my work, is against University
Regulations and that doing so will result in loss of marks and disciplinary proceedings. I
understand and agree that the University’s plagiarism software ‘Turnitin’ may be used to
check the originality of the submitted coursework.
Signed: …..…………………………………….………... Date: ……………………
2. Define and classify spondylolisthesis
and discuss the management of high
grade slips
Hiren Maganlal Divecha
Candidate Number: 1056984
ENT547 – Surgical Practice
Word count – 2193
3. Contents
Definition of Spondylolisthesis ............................................................................................................1
Classification.......................................................................................................................................2
1. Wiltse-Newman Classification .................................................................................................2
I. Dysplastic.............................................................................................................................2
II. Isthmic .................................................................................................................................3
III. Degenerative .......................................................................................................................4
IV. Traumatic.............................................................................................................................4
V. Pathologic ............................................................................................................................4
VI. Iatrogenic.............................................................................................................................4
2. Meyerding Classification..........................................................................................................5
Management of high grade slips .........................................................................................................6
1. Child/ Adolescent ....................................................................................................................6
2. Adult .......................................................................................................................................7
References........................................................................................................................................ 10
4. Definition of Spondylolisthesis
Spondylolisthesis is the anterior (or posterior) displacement of a vertebra (with the vertebral column
above) relative to the vertebra below. The origin of this word is from Greek, spondylos – vertebra and
olisthos – slipperiness [1]. Spondylolisthesis was first described in 1782, by the Belgian obstetrician
Herbiniaux, as an osseous narrowing of the birth canal. Kilian was the first to use the term
spondylolisthesis in 1854.
1
5. Classification
1. Wiltse-Newman Classification
The Wiltse-Newman classification [2] is the most commonly used clinical classification system of
spondylolisthesis (see Table 1) according to aetiology.
Type Description
I Dysplastic
II Isthmic
A – Spondylolysis
B – Pars elongation
C – Acute fracture
III Degenerative
IV Traumatic
V Pathologic
VI Iatrogenic
Table 1: Wiltse-Newman classification of spondylolisthesis
I. Dysplastic
This is a rare form of spondylolisthesis (14-21% [3]) and results from congenital malformation
of the neural arch or inferior facets of the L5 vertebra and/ or the upper part of the sacrum.
This can be associated with spina bifida. Typical structural abnormalities that predispose to
anterolisthesis of L5-S1 include a rounded sacrum, trapezoidal L5 vertebral body, hypoplastic
inferior L5 facets that subluxate anteriorly. The pars interarticularis and pedicles may appear
attenuated/ elongated but will only have a defect in severe slips.
2
6. II. Isthmic
The lesion in this type of spondylolisthesis occurs in the pars interarticularis.
A. Spondylolysis – refers to a fatigue fracture of the pars interarticularis with
histological features of fibrocartilaginous pseudoarthrosis. Wiltse et al. [4] proposed
that this defect arose from chronic loading of a genetically predisposed pars
interarticularis. It is never seen in newborns or non-ambulant individuals. Activities
resulting in repeated hyperextension of the lumbar spine have been associated with
higher incidences (diving, gymnastics, fast-bowlers, weight lifters, javelin throwers,
ballet dancers). This is the most common type of spondylolysis in the under 50yr age
group. It is more common in males, but severe slips are more common in females.
Based on a North American Caucasian population study, Fredrickson et al. [5]
reported an incidence of spondylolysis of 4.4% at 6yrs rising to 6% by early
adulthood. They also noted that only 25% of these developed spondylolisthesis.
Other ethnic groups are reported to have higher prevalence of spondylolysis (Alaskan
Inuit >30%; Japanese >40%). The L5 vertebra is most commonly affected (90%)
followed by L4 (5%) and L3 (3%). The higher lumbar levels tend to be more
symptomatic.
B. Pars elongation – a stress fracture of the pars interarticularis may go on to heal,
resulting in pars elongation that will allow some anterior slip.
C. Acute fracture – an acute hyperextension type injury can result in a pars
interarticularis fracture with a resulting spondylolisthesis. The “Hangman’s fracture”
of C2 is an example in the cervical spine.
3
7. III. Degenerative
This is the most common form of spondylolisthesis in patients over 50yrs [6]. The neural arch
and pars interarticularis remain intact. With degenerative disc disease, facet joint
arthropathy develops. Remodelling of the facet joints allows forward slip to occur. L4/5 is
more commonly affected (facets are more sagittally orientated).
IV. Traumatic
This results from an acute fracture to the neural arch not involving the pars interarticularis.
These are very rare and involve the pedicles/ posterior elements [7].
V. Pathologic
Bony metastases, osteoporosis, Paget’s disease, tuberculosis and giant cell tumours can lead
to lytic pars interarticularis defects.
VI. Iatrogenic
Wide laminectomy or facetectomy procedures can destabilise that vertebra and result in
spondylolisthesis.
4
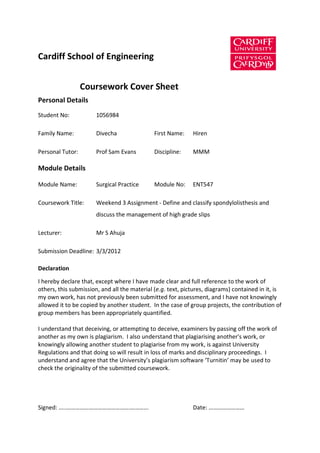
8. 2. Meyerding Classification
Spondylolistheses can be classified according to the amount of anterior translation/ slip. Meyerding
[8] classified this into Grades I – V (see Figure 1). The superior endplate of the vertebra below is
divided into quarters and the position of the posterior edge of the vertebral body above is
determined. A slip of more than 50% is considered high grade.
Figure 1: Meyerding Classification of Spondylolisthesis - (x/y = % slip). Grade I - 0-24%; Grade II - 25-49%; Grade
III - 50-74%; Grade IV 75-99%; Grade V - >100% (spondyloptosis). ( [9])
5
9. Management of high grade slips
1. Child/ Adolescent
A high-grade slip results in decreased lumbosacral lordosis and a progressive kyphotic deformity. It
has been suggested that these patients are best treated with fusion [10]. An in situ postero-lateral
fusion from L4 to S1 can be performed with placement of graft between the sacral alae and the
transverse processes. This forms a large fusion mass that prevents further slippage (after a period of
brace immobilisation). Long-term results with in situ postero-lateral fusion suggest maintenance of
symptom control and no obvious accelerated degenerative changes at the levels above [11]. For
older adolescents/ adults (especially with neurological symptoms/ cauda equina), it has been
suggested that wide decompression from L4 to S2 can be performed followed by insertion of a fibula
strut graft as a dowel between the S1 and L5 vertebral bodies. A postero-lateral fusion is then
performed to give a circumferential fusion. In a long-term follow up, Smith & Bohlman [12] reported
good results in a small cohort treated in this manner.
An argument for reduction and fusion can be made based on the following advantages – restoration
of sagittal balance/ biomechanics, better cosmesis, improvement of spinal stenosis symptoms and
reduced shear forces across fusion mass (theoretically reduces chances of pseudoarthrosis).
Furthermore, instrumented fusion allows for earlier mobilisation/ rehabilitation whilst maintaining
reduction. Patients with high-grade dysplastic spondylolistheses in particular may be at higher risk of
non-union and therefore benefit from reduction and instrumented fusion. Interestingly, Poussa et al
[13] found similarly good outcomes when comparing reduction with in situ fusion, but higher
complications with reduction (neurological and increased blood loss). The majority of nerve root
strain occurs at the end of reduction. Therefore, a partial controlled reduction with posterior
6
10. instrumentation (neurophysiological monitoring throughout) and postero-lateral fusion has been
suggested to be a safer alternative [14].
Management of spondyloptosis in children/ adolescents can be done with an in situ circumferential
fusion [12] and has the lowest chance of neurological injury. Alternative, a Gaines procedure can be
performed. The first stage involves an anterior L5 vertebrectomy. The second stage involves excision
of the L5 laminae/ pedicles and posterior instrumented reduction of L4 to S1. Neurological injury can
occur in 1/3rd of patients with this procedure [15].
2. Adult
Some adults may present with little or no pain despite having a high-grade spondylolisthesis. They
may describe more mechanical low back pain. A trial of physiotherapy and nerve root injections if
required may be attempted. Failing this, operative intervention may be considered.
Reduction remains controversial, as there is an increased risk of neurological injury (usually L5 nerve
root, occasionally cauda equina). Some studies have demonstrated improved fusion rates compared
to non-instrumented in situ fusion, though there have been no reports of improved clinical outcome
with reduction as compared to fusion in situ.
There are a number of surgical fusion options described, which can be instrumented or not:
posterolateral in situ fusion
posterior interbody lumbar fusion (PLIF) – laminectomy, discectomy and interbody fusion
(cage, fibula allograft)
anterior lumbar interbody fusion (ALIF) – trans-l/ retro-peritoneal approach, discectomy,
interbody fusion (cage/ structural graft)
7
11. transforaminal lumbar interbody fusion (TLIF) – posterior approach through foramen,
therefore avoids handling of cauda
circumferential fusion – combined ALIF + posterolateral fusion
posterior trans-sacral interbody fusion (fibula strut or screw)
Gaines procedure – for spondyloptosis
Postero-lateral in situ fusion has been the preferred treatment until recently. Whilst this can be
performed without instrumentation, there is a risk of pseudoarthrosis (up to 40%) or of the fusion
mass bending, resulting in further slippage (26%) [10] (note – these were reported in an adolescent
group). Posterior instrumentation is therefore recommended from L4 to S1 with/ without L5 pedicle
screws.
A study by Helenius et al [16] compared the outcomes for posterolateral fusion, ALIF and
circumferential fusions, all performed in situ without instrumentation. The circumferential fusion
group had the best functional outcome (pain VAS, Oswestry Disability Index, SRS-22) with the least
progression of deformity over the follow-up period. Interestingly, complications were lower in the
circumferential fusion group.
In a retrospective study of posterior trans-sacral interbody fusion using Hollow Modular Anchorage
(HMA) screws filled with cancellous graft, supplemented with postero-lateral fusion and posterior
instrumentation, Lakshmanan et al [17] found circumferential fusion was achieved in all 12 patients
with 11 experiencing resolution of leg pain. Pain and SF-36 scores improved and there were no
neurological complications. The authors concluded that a stable circumferential fusion was achieved
with this technique and the potential complications of using a fibula strut graft (donor site morbidity,
fracture) are avoided.
8
12. It seems that large, randomised, controlled, comparative studies with long-term follow-up are lacking
in the area of surgical management of high-grade spondylolisthesis. There are numerous
retrospective studies reported, but the lack of large comparative studies makes interpretation and
application to every-day clinical management difficult. It would seem that the recent literature
favours partial reduction of high-grade spondylolistheses and circumferential fusion techniques
supplemented with instrumentation to protect the fusion site and allow early mobilisation.
9
13. References
[1] “Spondylolisthesis,” Random House, Inc, [Online]. Available:
http://dictionary.reference.com/browse/spondylolisthesis. [Accessed 29 January 2012].
[2] L. L. Wiltse, P. H. Newman and I. Macnab, “Classification of spondylolysis and spondylolisthesis,”
Clin Orthop Relat Res, vol. 117, pp. 23-9, 1976.
[3] P. H. Newman, “The etiology of spondylolisthesis,” J Bone Joint Surg Br, vol. 45, pp. 39-59, 1963.
[4] L. L. Wiltse, E. H. Widell and D. W. Jackson, “Fatigue fracture: The basic lesion in isthmic
spondylolisthesis,” J Bone Joint Surg Am, vol. 57, pp. 17-22, 1975.
[5] B. E. Fredrickson, D. Baker, W. J. McHolick, H. A. Yuan and J. P. Lubicky, “The natural history of
spondylolysis and spondylolisthesis,” J Bone Joint Surg Am, vol. 66, pp. 699-707, 1984.
[6] K. Majid and J. S. Fischgrund, “Degenerative lumbar spondylolisthesis: Trends in management,” J
Am Acad Orthop Surg, vol. 16, pp. 208-15, 2008.
[7] H. Miyamoto, M. Sumi, O. Kataoka, M. Doita, M. Kurosaka and S. Yoshiya, “Traumatic
spondylolisthesis of the lumbosacral spine with multiple fractures of the posterior elements,” J
Bone Joint Surg Br, vol. 86, no. 1, pp. 115-8, 2004.
[8] H. W. Meyerding, “Spondylolisthesis,” Surg Gynecol Obstet, vol. 54, pp. 371-7, 1932.
[9] “Spondylolisthesis - Degenerative,” Alphatec Spine, Inc, [Online]. Available:
http://www.agingspinecenter.com/content/spondylolisthesis-degnerative. [Accessed 29 January
2012].
[10] D. Boxall, D. S. Bradford, R. B. Winter and J. H. Moe, “Management of severe spondylolisthesis in
children and adolescents,” J Bone Joint Surg Am, vol. 61, pp. 479-95, 1979.
[11] A. Grzegorzewski and S. J. Kumar, “In situ posterolateral spine arthrodesis for grades III, IV and V
10
14. spondylolisthesis in children and adolescents,” J Paediatr Orthop, vol. 20, pp. 506-11, 2000.
[12] M. D. Smith and H. H. Bohlman, “Spondylolisthesis treated by a single stage operation combining
decompression with insitu posterolateral and anterior fusion: An analysis of eleven patients who
had long-term follow-up,” J Bone Joint Surg Am, vol. 72, pp. 415-21, 1990.
[13] M. Poussa, D. Schlenzka, S. Seitsalo, M. Ylikoski, H. Hurri and K. Osterman, “Surgical treatment of
severe isthmic spondylolisthesis in adolescents: Reduction or fusion in situ,” Spine, vol. 18, pp.
894-901, 1993.
[14] L. G. Lenke and K. H. Bridwell, “Evaluation and surgical treatment of high grade isthmic
dysplastic spondylolisthesis,” Instr course lect, vol. 52, pp. 525-32, 2003.
[15] S. M. Lehmer, A. D. Steffee and R. W. Gaines, “Treatment of L5-S1 spondyloptosis by staged L5
resection with reduction and fusion of L4 onto S1 (Gaines procedure),” Spine, vol. 19, pp. 1916-
25, 1994.
[16] I. Helenius, T. Lamberg, K. Osterman, D. Schlenzka, P. Tervahartiala, S. Seitsalo, M. Poussa and V.
Remes, “Posterolateral, anterior, or circumferential fusion in situ for high-grade
spondylolisthesis in young patients: a long-term evaluation using the Scoliosis Research Society
questionnaire.,” Spine, vol. 31, no. 2, pp. 190-6, 2006.
[17] P. Lakshmanan, S. Ahuja, M. Lewis, J. Howes and P. R. Davies, “Transsacral screw fixation for
high-grade spondylolisthesis,” Spine, vol. 9, pp. 1024-9, 2009.
11