Call Girl In Pune 👉 Just CALL ME: 9352988975 💋 Call Out Call Both With High p...
19 Insulin Types
1.
2.
3. A more difficult question is when to use
General principles of insulin therapy in diabetes mellitus insulin in patients with type 2 diabetes.
This disorder is characterized by both :
o insulin resistance and
INTRODUCTION — Insulin is used in the treatment of patients o relative insulin deficiency
with diabetes of all types. The need for insulin depends upon the
balance between :
o insulin secretion and Therapy should begin with diet, weight reduction, and exercise, which
o insulin resistance can frequently induce normoglycemia if compliance is optimal.
All patients with type 1 diabetes need insulin treatment
permanently, unless they receive an islet or whole organ Patients with persistent hyperglycemia are often started on one or
pancreas transplant more oral hypoglycemic drugs.
many patients with type 2 diabetes will require insulin as their
Metformin is a good early choice, based on its safety profile, neutral
beta cell function declines over time
effect with regard to weight gain, and ability to lower glycemia.
WHICH PATIENTS NEED INSULIN — Insulin is added if goal glycemic control is not attained.
o all patients with type 1 diabetes
o patients with secondary diabetes due to pancreatic
insufficiency
o many patients with type 2 diabetes to manage hyperglycemia
Initiation of insulin therapy, however, is often unnecessarily
delayed, owing to physician or patient reluctance and other
The peak incidence of type 1 diabetes is around the time of factors, thus exposing patients to the physiological
puberty, but about 25 percent of cases present after 35 years of consequences of prolonged hyperglycemia.
age [1]
Patient preconceptions about use of insulin need to be addressed
[3] . Patients should be made aware that initiating insulin does not
represent a personal "failure" and that most patients with type 2
diabetes will eventually require exogenous insulin, due to decline in
Clinical features which, if present in a patient with diabetes endogenous insulin production.
at any age, suggest the need for insulin therapy include :
o marked and otherwise unexplained recent weight loss
(irrespective of the initial weight),
o a short history with severe symptoms, and
o the presence of moderate to heavy ketonuria
Diabetic ketoacidosis at first presentation usually indicates that the
patient has type 1 diabetes and will require lifelong insulin treatment.
However, some patients with type 2 diabetes, especially
in the Afro-Caribbean populations (so-called "Flatbush
diabetes"), may present with ketoacidosis [2] .
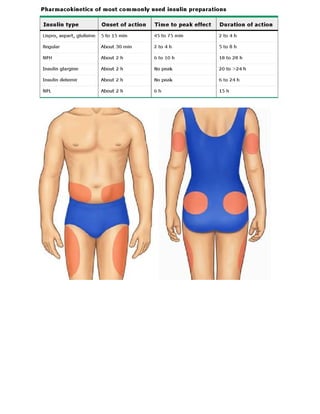
4. INSULIN PREPARATIONS To produce an insulin preparation with :
o a faster onset and
o shorter duration than regular insulin (clear zinc
insulin, CZI)
Standard preparations —
modifications have been made in the insulin molecule to prevent it
divided into two basic categories: from forming hexamers or polymers that slow absorption and delay
action [4] .
Intermediate- to long-acting preparations
These rapid-acting insulins :
(NPH, neutral protamine lispro [NPL], detemir, or glargine)
(insulin lispro, aspart, and glulisine)
are typically administered once or twice daily to provide basal insulin
Have :
levels that suppress hepatic glucose production and maintain near
normoglycemia in the fasting state. o an onset of action within 5 to 15 minutes,
o peak action at 30 to 90 minutes, and
o a duration of action of two to four hours [5-8]
Intermediate-acting insulin conventional insulin therapy =
(NPH)
simpler insulin regimens, such as single daily injections, or two
also provides some peak coverage for breakfast and lunch intake, injections per day of regular and NPH insulin, mixed together in the
although not as physiologic as replacement with faster-acting same syringe and given in fixed amounts before breakfast and dinner.
insulin given at mealtimes.
intensive insulin therapy =
Basal insulin levels can also be achieved by
continuous infusion of regular insulin via an more complex regimens that separate basal insulin delivery (given as
insulin pump, used almost exclusively in type one to two daily injections of intermediate- or long-acting insulin)
1 diabetes.
with superimposed doses of short acting or rapid acting insulins three
or more times daily.
Short acting
While intensive regimens were initially used for patients
o (regular) or with type 1 diabetes, they are now frequently used for
o rapid-acting (lispro, aspart, or glulisine) insulin patients with type 2 diabetes as well.
are typically provided as a premeal bolus to cover the extra
requirements after food is absorbed.
Conventional insulin therapy is unlikely to
achieve target A1C levels in patients with
type 1 diabetes, and may provide
suboptimal glycemic control for patients
with type 2 diabetes as beta cell function
declines.
5. 2..The peak action also varies directly with the
proportion of regular insulin in the combination.
Both glucose and insulin metabolism
One study, as an example, compared the time course of serum
are altered in patients who have chronic insulin concentrations with two mixtures of different NPH-to-regular
insulin ratios: 50/50 (equivalent to 10.5 units of each preparation in
renal failure. The changes in the insulin a 70 kg patient) and 70/30 (equivalent to 14.7 units of NPH and 6.3
units of regular insulin) [12] .
regimen that must be made in these
The former, which contained more regular insulin, resulted in
patients are discussed separately. higher serum insulin concentrations in the first six hours
Changes in the proportion of NPH-to-regular insulin in these
premixed combinations are often not sufficient to improve
postprandial glycemic control [13] .
Premixed insulins — In addition, because of the variability in peak effect, it may be
more difficult to achieve excellent glycemic control with premixed
The use of premixed insulins is not recommended for patients
insulins even though they are easier to use [14] .
with type 1 diabetes, as intensive regimens require frequent
adjustments of the premeal bolus of short acting or rapid acting
insulin.
Premixed Lispro/NPH in type 1 diabetes may be of some
benefit for patients who will not comply with an
intensive regimen [9] . Many patients with type 2 diabetes can use pre-mixed
preparations with reasonable effect. However, if
the aim is
to truly vary the dose of fast-acting insulin
o Some patients with type 2 diabetes who require premeal insulin in
before a meal, patients would do best to give the fast-
addition to basal insulin prefer premixed insulins for acting and intermediate-acting insulins as separate injections.
convenience.
o Some premixed (biphasic) insulin preparations are commercially
available, but patients may also draw up their premeal and basal
If near normoglycemia is the goal, it is preferable to
insulins in the same syringe prior to injection.
keep basal and premeal insulin injections separate and to adjust
them independently.
However, there are problems with mixing
different insulin preparations:
1..When drawing up both insulin preparations in the same syringe,
serum insulin concentrations tend to approach a single peak.
This is less of a problem when a rapid-acting insulin rather than regular
insulin is mixed with NPH and injected immediately after mixing [10] .
It is also less of a problem with premixed insulins, such as Lispro
Mix25 (25 percent insulin lispro and 75 percent of an intermediate-
acting insulin) [11] .
6. ADA guidelines for mixed-insulin — DETERMINANTS OF INSULIN EFFICACY —
We almost never recommend commercially premixed Effective use of insulin requires an understanding of the major
variables that affect the degree of glycemic control.
insulins in the treatment of type 1 diabetes.
These include :
o the insulin preparation,
When commercially or self-mixed insulins are used o the size of the subcutaneous depot,
o injection technique,
for patients with type 2 diabetes, the following o the site of injection, and
guidelines adapted from the American Diabetes Association o subcutaneous blood flow
(ADA) should be followed [15] .
1..Patients who are well-controlled on a self-mixed regimen should Type of insulin —
continue the same procedure for preparing their dose.
o The time of onset,
o peak activity, and
o duration of action
2..Insulin glargine and insulin detemir should not be
of subcutaneous insulin preparations :
mixed with other insulins due to the low pH of the diluents.
can only be approximated, since the usually quoted data are
3..After mixing NPH with regular insulin, the formulation should based upon the administration of small amounts of insulin to a few
be used immediately normal subjects
4..Rapid-acting insulin can be mixed with NPH. When this is Furthermore, the degree of absorption of any dose, both among
done, the mixture should be injected within 15 minutes prior to a meal. patients and in the same patient,
can vary from day to day
by as much as 25 to 50 percent, leading to unexplained
fluctuations in glycemic control [18,19] .
This effect is greatest with longer-acting insulins and least with
Inhaled insulin — regular, lispro, aspart, and glulisine insulin.
An inhaled form of rapid-acting insulin was available for a short time but
was discontinued in 2007.
Thus, a dose of NPH insulin given before the
Other inhaled insulin preparations are in clinical trials but are not
currently available. evening meal may be sufficient to last
through the night in one patient but may
dissipate in another, resulting in fasting
Studies have shown that inhaled insulin causes a very rapid
rise in serum insulin concentration (similar to that after
hyperglycemia.
subcutaneous insulin lispro and aspart, and faster than that
after subcutaneous regular insulin) [16,17] .
Part of the day-to-day variability in the absorption of NPH insulin may
However, due to its inefficient absorption, higher doses of insulin must be
be due to incomplete mixing of the suspensions of insulin and
administered to achieve a therapeutic response.
protamine or zinc. However, the absorption of long-acting insulin
analogs such as insulin glargine also seems to vary [20] . There is
some suggestion that day to day variability of absorption is less
with insulin detemir, but the clinical significance of this has not
been established [21] .
7. Size of subcutaneous depot — Injection technique —
The variability in absorption is increased and net absorption is reduced Injection technique is the same with insulin syringes and
with increasing size of the subcutaneous depot [18] .
with pen injectors. Both the angle of needle entry and the
This can become a limiting factor in patients who are insulin depth of penetration affect the rate of insulin absorption.
resistant and require large doses given several times per day.
Very shallow insertion can cause a painful intradermal
injection that is not well absorbed.
Conversely, one of the reasons why continuous subcutaneous insulin In comparison, a perpendicular injection in a lean area may
infusions may serve to smooth blood glucose control is that only regular
result in an intramuscular injection, from which absorption
insulin is used and the size of the subcutaneous depot is very small (since
the reservoir is held in a syringe or other chamber, outside the body) is more rapid [26,27] .
[22] .
Another approach to reduce the size of the subcutaneous
Patients should be referred to a certified diabetes educator to be
depot and thereby increase insulin absorption is to use taught proper insulin injection technique. The recommended
high pressure jet injectors [23] . technique is to use an area of the body in which about 2.5 cm (one
inch) of subcutaneous fat can be pinched between two fingers.
The syringe, with a 0.5 inch microfine (27G) or ultrafine (29G) needle, is
These devices lead to a more rapid fall in blood glucose inserted perpendicular to the pinched skin up to the hilt and the
concentrations and a shorter duration of insulin action [24] , insulin is then injected.
although there is no evidence that the variability in insulin
absorption is improved. The syringe barrel should not be pulled back before injection or the
needle removed if blood is obtained. The needle should be held in
Jet injectors may also cause less pain than traditional needles and place for several seconds before being withdrawn. This is especially
syringes. However, they are expensive, difficult to maintain, and
important when using pen injectors, to avoid insulin leakage after
are not recommended for routine use.
withdrawal of the needle.
The common practice of cleaning the skin with an alcohol swab
A variety of pen injectors, used with pre-filled cartridges, are now before injection may not be necessary.
available which are more convenient than conventional syringes
and bottles, but are more expensive. When small doses of regular In a crossover study of 50 patients who received over 13,000
insulin (less than five units) are being given, the error in measuring injections, there was no difference when the usual manner of
the dosage is almost 50 percent less when using pen injectors than injection was compared with injections through clothing [28] .
with conventional insulin syringes [25] .
The only problem with the latter was an occasional blood stain on
the clothing.
8. Site of injection —
Potential sites for insulin injection are the :
Alterations in subcutaneous blood flow —
o upper arms, The degree of insulin absorption is also determined by the rate of
o abdominal wall, subcutaneous blood flow.
o upper legs and
o buttocks Thus, insulin absorption is :
o reduced by smoking [30] and
o increased by any increases in skin temperature [31] induced
A common cause of day-to-day variability in insulin action is the by exercise, saunas or hot baths, and local massage [32-35] .
random rotation of injection sites from one region of the body to
another.
Insulin is absorbed : These variations are more marked with regular and rapid-
o fastest from the abdominal wall, acting insulins than with longer-acting insulins [34] .
o slowest from the leg and buttock, and
o at an intermediate rate from the arm
at any of these sites, the rapidity of insulin absorption
varies inversely with subcutaneous fat thickness [19,29] . SUMMARY AND RECOMMENDATIONS
Insulin therapy is essential in all patients with type 1 diabetes, and
In a study using radiolabeled regular insulin, the
percent of the dose that disappeared at two hours was
approximately 49 percent in the abdomen, 37 percent in is also often used in patients with type 2 diabetes.
the arm, and 26 percent in the leg [29] .
The postprandial rise in plasma glucose concentration
varied inversely with the rate of insulin absorption,
being 30 to 50 mg/dL (1.7 to 2.8 mmol/L) less after
Although initial treatment for type 2 diabetes should be diet
abdominal than after leg injection; the values after arm
injection were intermediate between these responses. modification and exercise, followed by oral agents if normoglycemia is
not achieved, insulin therapy is often indicated and its use should not
be delayed when it becomes necessary.
These differences can be useful clinically.
While intensive insulin therapy, utilizing a basal insulin with multiple
Premeal regular or rapid-acting insulin should be rapidly premeal injections of a very rapidly acting insulin, has become
absorbed, and injection into the abdominal wall may standard therapy in type 1 diabetes, simpler regimens are often used
in type 2 diabetes.
therefore be preferable.
On the other hand, slower absorption from
the leg or buttock may be desirable with the
pre-evening meal dose of intermediate-acting We suggest not prescribing premixed insulin for type 1 diabetes
(Grade 2C).
insulin to ensure a duration of action that lasts
Premixed insulin may be considered in some patients with type 2
through the night. diabetes for convenience.
Specific guidelines should be followed for premixing to avoid
changes in speed of absorption and peak action.
Commercially available premixed insulins are a reasonable choice
if the insulin ratio is appropriate to the patient's insulin requirement.
9. Addressing patient resistance to
Effective use of insulin requires an understanding of the
major variables that affect the degree of glycemic control:
insulin therapy for patients with
the insulin preparation, the size of the subcutaneous depot, type 2 diabetes
injection technique, the site of injection, and subcutaneous
blood flow Patient concerned with pain from injection
o Minimal with thinner, smaller needles
o Use of insulin pens
Insulin absorption is variable between patients and in the Patient worried that starting insulin signifies worsening
same patient, especially for longer acting preparations. diabetes
o Diabetes is a progressive disease
o Taking insulin will control blood glucose and help prevent
complications
o Taking insulin may slow down the rate of beta cell failure
Variability is greater with larger injection doses Patient believes that need for insulin signifies patient failure
to follow treatment regimen
o Diabetes is a progressive disease; beta cell activity
Injections should be given into an area of pinched skin, declines over time
o Not related to patient compliance
with needle inserted perpendicular and up to the hilt; the o Patient fears low blood sugar reactions
barrel should not be pulled back. o Explain that severe hypoglycemia is rare in type 2
diabetes
Precleaning skin with alcohol is unnecessary and may o Self-monitoring glucose levels
o Explain how to avoid and how to treat hypoglycemia
increase the pain of an injection.
Patient concerned that taking insulin will upset daily routine
o Address specific concerns
Absorption is fastest from injections into the abdominal o Taking insulin may be less intrusive than complicated
wall, which may be a preferable site for premeal insulin. drug regimens
Patient believes that insulin will decrease his/her quality of life
Slower absorption from the leg or buttock may be
appropriate for evening doses of intermediate-acting o Benefits from glucose control: more energy, better sleep,
insulin. overall well-being
o Patient thinks insulin will lead to diabetic complications
o Discuss role of insulin in reducing risk of diabetic
complications
Patient concerned that he/she will be treated differently by
friends and family
o Educate friends and family: offer reading materials on
diabetes, support groups for family
o Patient has heard insulin causes weight gain
o Role of diet and exercise
Patient wants a more natural alternative therapy
o Insulin is the most natural therapy for diabetes. It is
replacing the hormone that the patient does not make
enough of.