Acute vs chronic scrotal swelling
•Télécharger en tant que PPTX, PDF•
54 j'aime•18,573 vues

Houseman level

Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Acute vs chronic scrotal swelling
Similaire à Acute vs chronic scrotal swelling (20)
Plus de Kochi Chia
Plus de Kochi Chia (9)
Dernier
Dernier (20)
Acute vs chronic scrotal swelling
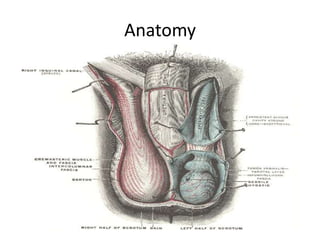
- 1. Anatomy
- 6. ACUTE vs. CHRONIC scrotal swelling Acute Chronic •Torsion of spermatic cord/testis •Torsion of appendix, epididymis •Acute epididymitis/orchitis •Mumps orchitis •Henoch-Schönlein purpura (painless) •Trauma •Insect bite •Thrombosis of spermatic vein •Fat necrosis •Hernia •Folliculitis •Dermatitis, acute •Hydrocele (painless) •Hernia (painless) •Varicocele •Spermatocele •Sebaceous cyst •Tumor (painless)
- 7. Acute • Characteristic Pain Swelling Erythema Sudden onset • Always an EMERGENCY!!!
- 8. Why EMERGENCY? • Potential for testicular loss and infertility • Legal action can be taken • Accurate diagnosis limited by similarity of presentation and physical findings of different causes • Radiological techniques is helpful, but may delay treatment • Operation may be needed for Dx and Tx purposes
- 9. Chronic • Long standing • Slow growing (>6 weeks) • Pain/painless • Incidental finding
- 10. Testicular torsion • Torsion of the testis (spermatic cord) → strangulation of gonadal blood supply → testicular necrosis and atrophy. • Window of opportunity to salvage - within 6 hours! • Acute scrotal swelling in children indicates torsion of the testis until proven otherwise _________________________________________________________ • Acute-onset agonising pain over hemiscrotum, groin, lower abdomen • Nausea and vomiting • Scrotal swelling with erythema • High lie of testis, palpable thickening tender cord • May occur at rest or may relate to sports or physical activities (sometimes upon straining at stool, coitus, during sleep) • May describe similar previous episodes, which may suggest intermittent testicular torsion (spontaneous detorsion) • No voiding problems or painful urination • Difficulty in ambulation
- 11. • Predisposing causes 1. Inversion of testis – transverse lie/upside down 2. High investment of tunica vaginalis 3. Separation of epididymis from body (long mesorchium) – torsion without involving cord, confined to pedicle that connect testis with epididymis • 2 types of torsion: • Extravaginal (5%) - testis rotates freely prior to fixation of testis - more common in neonates • Intravaginal (16%) : Bell Clapper deformity - lack of fixation (testis freely suspended within tunica vaginalis) - peak incidence at adolescence age 13
- 12. • Incidence – Most common between 10-25yo (1:4000) • Pathophysiology : Violent contraction of abdominal muscles → contraction of cremaster → favors rotation around vertical axis • Torsion of 3-4 turns : irreversible changes (necrosis) within 2 hours • Torsion of 1 turn (360:) : well tolerated for 12 hours (20% viability) necrosis after 24 hours • Torsion of 90: : well tolerated for 7 days L P SONDA, J LAPIDES in Surgical Forum (1961)
- 14. • O/E – Extremely tender, enlarged – High riding testis – Reactive hydrocele – Scrotal wall erythema – Ecchymosis – Cremasteric reflex • if present, no torsion • if absent 66% rule in torsion • Ix – UFEME : TRO UTI/epididymorchitis, ↑leucocytes in 30% patients – FBC : ↑TWC in 60% patients – US Doppler scrotum/testis – Contrast MRI : evidence of torsion knot or whirlpool patterns – Nuclear testicular scan/scintigraphy • to ddx torsion from acute epididymitis by demonstrating cold spot and ring signs. * Radiologic techniques are helpful but may delay treatment*
- 15. US Doppler scrotum/testis • Sensitivity 80 - 90% Specificity 100% • The case on the left shows a testicular torsion of the left testis. • Complete absence of intratesticular blood flow and normal extratesticular blood flow on color Doppler images is diagnostic, if the flow is normal in the contralateral testis.
- 16. Nuclear testicular scan/scintigraphy - Technetium-99 (99mTc-pertechnetate) to trace testicular blood flow - Requires 1-2 hours - 86-100% accuracy
- 18. • Management 1. Alleviation of symptoms – Analgesic : IV/IM pethidine – Antiemetic : IV stemetil 10mg, IV maxolon – Anxiolytic : IV valium 2. Manual Detorsion • Rotate testicle in medial to lateral direction “open the book” • usually 1-2 complete turns • relief of pain • return of blood supply to testicle (confirmed with US) • additional time before OR • patient may not tolerate. 3. Surgical exploration • Bilateral orchidopexy – to prevent future torsion • Orchidectomy + contralateral orchidopexy 4. Placement of testicular prosthesis – after 6 months of orchidectomy via inguinal incision
- 20. • Prognosis – < 6 hours, 90% salvage – > 6 hours, 20% viability likelihood for orchidectomy – > 24 hours, 100% loss and atrophy • Complications – Testicular atrophy : may occur days-to-months after the torsion has been corrected. – Severe infection of the testicle and scrotum is also possible if the blood flow is restricted for a prolonged period.
- 21. Epididym-/orchitis • Most common cause of acute scrotum(75-80%) • Acute : < 6 weeks (CDC, STD treatment guidelines) • Young men – hx of STD exposure (Chlamydia trachomatis, Ureoplasma urealyticum, Neisseria gonorrhea) • Children : UTI, urinary tract structural anomalies (E. coli, Streptococci, Staphylococci, Proteus) • Older men : BPH, post vasectomy, post urological operative procedure/instrumentation, indwelling catheter, infectious prostatitis, TB • Orchitis : Syphillis, leprosy • Viral cause : Mumps (18% males), usually a/w parotid swelling
- 22. • Chronic tuberculous epididymo-orchitis usually insidious onset a/w “cold” abscess discharge • Syphillis – usually affects body of testis 1. Bilateral orchitis : congenital syphillis 2. Interstitial fibrosis → painless destruction of testis 3. Gumma : unilat. painless slow growing swelling • Leprous orchitis : testicular strophy in 25% male lepers.
- 23. • S/Sx – Acute progressive onset of scrotal/ groin pain (>24hr) – Gradual swelling, erythematous, shiny scrotum – Febrile fever – Dysuria – Difficulty in ambulation – Urethral discharge – Hx of recent instrumentation/indwelling CBD
- 24. • O/E – Scrotal swelling (secondary hydrocele), enlarged, erythematous and indurated – Indistinguishable testis (in later stage) – Cremasteric reflex is usually present – Prehn sign positive : elevation of the scrotum may provide relief of pain. – Pyuria
- 25. • Ix : – UFEME : ↑leucocytes > 10 visual field – MSU C&S/pus C&S : bacterial growth – Venereal disease screening : for sexually active men – Immunofluorescent antibody test, if suspected mumps – US scrotum/testis – Flex CU : to detect structural anomalies – Scrotal exploration or aspiration (rare) • If torsion cannot be ruled out • Complications eg. abscess, pyocele, testicular infarction • Failed conservative treatment in 48-72 hours
- 26. US scrotum/testis (sensitivity 82-100%, specificity 100%) • The case on the left shows the typical features of epididymitis. • Swollen, heterogeneous, hyperemic • Hydrocele • Scrotal wall thickening. • With color doppler there is increased flow. A normal epididymis has only limited colorflow.
- 27. • Diagnostic Criteria for Epididymitis – Gradual onset of pain – Dysuria, discharge, or recent instrumentation/CBD – History of genitourinary abnormality (UTI, neurogenic bladder, hypospadias, etc.) – Fever > 38:C – Tenderness and induration at epididymis – Abnormal UFEME (>10 leucocytes visual fields/RBC) • 3 or more findings present - definite Epididymitis • 2 findings present - probable Epididymitis • 1 finding present - possible Epididymitis
- 28. • Management 1. Antibiotic therapy : if UFEME/MSU C&S positive for infection – Suspect STD : IV rocephine + T. doxycycline x 10/7 – Suspect UTI : IV/T. ciprobay x 10/7 – Others : Azithromycin, Bactrim, Gentamicin, 2. Bed rest/scrotal elevation : if UFEME/MSU C&S negative → sterile chemical epididymo-orchitis (structural anomalies) 3. Supportive therapy : ice packs, cool Sitz bath 4. Analgesia : opioids, NSAIDs 5. Orchidectomy : if complications developed
- 29. • Complications – Abscess – Pyocele – Testicular infarction – Testicular atrophy – Infertility
- 30. • Prognosis – Resolution of sx in 2-4 weeks if properly treated – Chronic epididymoorchitis may have frequent mild attacks, may have lumps in scrotum due to fibroplasia – May have threat of infertility
- 31. Torsion of testicular/epididymal appendage • Remnant of Wolffian(epididymis)/Mullerian(testis) duct • Can be twisted → torsion • o/e : testis palpable with normal lie, edematous, torsed appendage palpable over upper pole of testis, “blue-dot sign” if ecchymotic • US Doppler : normal testicular perfusion with hyperemia over appendage • Self limiting (infarct → atrophy)
- 33. Testicular trauma • Damage occurs when the testis is forcefully compressed against the pubic bones • Traumatic epididymitis : noninfectious inflammatory condition occurs within a few days after a blow to the testis. Treatment is same like nontraumatic epididymitis. • Scrotal trauma can also result in intratesticular hematoma, hematocele or laceration of the tunica albuginea (testicular rupture). • US Doppler : imaging technique of choice.
- 34. Degree of testicular trauma 1. Blunt (85%) : direct external force to testicle 2. Penetrating (15%) : sharp objects, high velocity missiles 3. Degloving : Scrotal skin sheared off • Genital self-mutilation : if testis vital, reimplantation is possible • Pathophysiology : rupture → intratesticular hemorrhage in tunica vaginalis → HEMATOCELE! → extends up to epididymis → bleeding → SCROTAL HEMATOMA!
- 35. • O/E – Swelling – Tenderness – Ecchymosis – Scrotal wall thickening • Palpable testis : unlikely rupture • Difficulty in palpation : US urgent to determine degree of testis injury
- 36. • Management 1. Bed rest 2. Scrotal support 3. Pain relief 4. Testicular debridement 5. Closure of tunica albuginea • Penetrating trauma : urgent exploration to assess degree of injury and control intratesticular hemorrhage • Degloving injury : often need debridement, skin closure may not be possible
- 37. • Indications for scrotal exploration include the following: – Uncertainty in diagnosis after appropriate clinical and radiographic evaluations – Clinical findings consistent with testicular injury – Disruption of the tunica albuginea – Absence of blood flow on US Doppler studies • Complications – Testicular infection – Testicular atrophy – Testicular necrosis – Infertility – Disruption of male hormonal functions
- 38. Incarcerated inguinal hernia • Irreducible inguinal hernia a/w pain • A surgical emergency • Scrotal swelling, groin pain/swelling, abdominal pain, constipation, fever, nausea/vomiting • Ix : FBC, US scrotum, CT • Mx : surgical exploration, herniotomy/hernioplasty
- 39. Hydrocele • A collection of serous fluid in the tunica vaginalis • Congenital : occurs in infants due to patent processus vaginalis peritoneal fluid can enter the scrotum Primary. (idiopathic) • Develop slowly • Large • Hard & tense • No defined cause • Over 40s Secondary • Develop rapidly • Small • Lax • Underlying cause • younger age group(20-40)
- 40. • Congenital hydrocele: processus vaginalis is patent & connects to the peritoneal cavity. In children <3yrs • Infantile hydrocele: the tunica and processus vaginalis are distended to the superficial inguinal ring. There is no connection. Occurs in all ages • Hydrocele of the cord: swelling near the spermatic cord. Ddx hernia, lipoma of the cord
- 41. • O/E often bilateral • Can “get above it” • Testes cannot be felt separately • Transluminates • Fluctuant • Fluid thrill • Not compressible or pulsatile • Can’t be reduced • Normal skin color & temp • Not tender if primary (may be tender if secondary) • Size can be reach up to 10-20cm in diameter • Surface smooth
- 42. • Ix : US scrotum to ddx from other causes • Management : • If congenital hydrocele persists beyond the age of 1year, surgical treatment is indicated. This involves the division and ligation of the processus. • In an adult with primary hydrocele Surgery Opening the tunica vaginalis longitudinally Emptying hydrocele Everting the sac Suturing it behind the cord thus obliterating the potential space Aspiration recurance In elderly patient who are not fit for surgery • Secondary hydrocele treat the underlying cause
- 43. Testicular tumor • Rare 1–1.5% of male cancers. • mainly affects younger men of 30 – 40yo • 90 - 95% arise from germ cells and are either seminomas (45%) or nonseminomas(50%). (Nonseminoma : choriocarcinoma, embryonal carcinoma, teratoma, and yolk sac tumors) • 5% are lymphomas, sertoli cell tumours or leyding cell tumours. • Prognosis is good particularly if there was no lymph node involvement
- 44. • Incidence and frequency – Seminomas in 30-40y. – Teratomas in 20-30y. – Imperfectly descended testes have a 20-30 times increased incidence of malignancy.
- 45. Recommended pathologic classification (EUA, 2011) Germ cell tumours • Intratubular germ cell neoplasia, unclassified type • Seminoma (including cases with syncytiotrophoblastic cells) • Spermatocytic seminoma (mention if there is a sarcomatous component) • Embryonal carcinoma • Yolk sac tumour • Choriocarcinoma • Teratoma (mature, immature, with malignant component) • Tumours with more than one histologic type (specify percentage of individual components) Sex cord/gonadal stromal tumours • Leydig cell tumour • Malignant Leydig cell tumour • Sertoli cell tumour (lipid-rich variant, sclerosing, large cell calcifying) • Malignant Sertoli cell tumour • Granulosa (adult and juvenile) • Thecoma/fibroma group of tumours • Other sex cord/gonadal stromal tumours (incompletely differentiated, mixed) • Tumours containing germ cell and sex cord/gonadal stromal (gonadoblastoma) Miscellaneous nonspecific stromal tumours • Ovarian epithelial tumours • Tumours of the collecting ducts and rete testis • Tumours (benign and malignant) of nonspecific stroma
- 46. • Classification 1. Germ cell tumors (90%) - Seminoma 90% - Embryonal carcinoma 20% - Choriocarcinoma <1% - Teratoma 5% - Teratocarcinoma 40% (teratoma + embryonal carcinoma) 2. Gonadal stromal tumor (5%) - Leydig cell tumor - Sertoli cell tumor 3. Secondary tumor (5%) • Lymphoma • Leukemia
- 47. Risk factors for testicular cancer Epidemiologic risk factors • History of cryptorchidism • Klinefelter syndrome • Testicular cancer in first-grade relatives • Contralateral tumour • Testicular intraepithelial neoplasia or infertility Pathologic prognostic risk factors for occult metastatic disease (stage I) 1. Seminoma • Tumour size (4 cm) • Invasion of the rete testis 2. Nonseminoma • Vascular/lymphatic invasion or peritumoural invasion • Proliferation rate (MIB-1) >70% • Percentage embryonal carcinoma >50% Clinical risk factors (metastatic disease) • Primary location • Elevation of tumour marker levels (AFP, B-HCG) • Nonpulmonary visceral metastasis*
- 48. • Dx is made based on 1. Clinical examination of the testis 2. General examination to exclude enlarged nodes or abdominal masses 3. US to confirm testicular mass.
- 49. Signs • can “get above it” • Testes cannot be felt separately • Harder than normal testis • Dull to percussion hydrocele • No pain • Irregular, different sizes • Surface usually smooth (sometime irregular or nodular)
- 50. Symptoms • Painless swelling of the testis • Heaviness in the scrotum • Maybe history of trauma delays diagnosis • Tiredness, LOW ,LOA • Abdominal pain if lymph nodes are enlarged • Swelling of legs caused by lymphatic or venous obstruction • Infertility • Secondary hydrocele
- 51. • O/E – Painless unilateral mass in the scrotum or the casual finding of an intrascrotal mass. – Gynaecomastia (common in nonseminomatous tumor) – Back and flank pain (rarely)
- 52. Ix : US testis CXR – to see cannon ball lesion if metastasized Tumour markers: AFP, βHCG, LDH CT TAP CT brain CT spine Bone scan US liver
- 53. • Serum tumour markers : prognostic factors used in diagnosis and staging (LDH). • The lack of an increase does not exclude • testicular cancer • LDH levels are elevated in 80% of patients with advanced testicular cancer, therefore should always be measured in advanced cancer • Tumour markers must be reevaluated after orchidectomyto determine half-life kinetics. • The persistence of elevated serum tumour markers 3 wk after orchidectomy may indicate the presence of disease, whereas its normalisation does not indicate absence of tumour. • Tumourmarkers should be assessed until they are normal, as long as they follow their half-life kinetics and no metastases • During chemotherapy, the markers should decline; persistence has an adverse prognostic value.
- 55. Management • Inguinal exploration and orchidectomy • If the diagnosis is unclear, a testicular biopsy (enucleation of the intraparenchymal tumour) should be taken for HPE • If metastasized : delay orchidectomy 1. If seminoma: Start radiotherapy plus chemotherapy. 2. If teratoma: combination chemotherpay 3 drugs(etoposide, vinblastine, methotrexate, bleomycin, cisplastin)
- 56. Organ-preserving surgery • Synchronous bilateral testicular tumours, metachronous contralateral tumours, or in a tumour in a solitary testis with normal preoperative testosterone levels, provided tumour volume is <30% of testicular volume • Radiotherapy may be delayed in fertile patients who wish to father children • must be carefully discussed with the patient