

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Ngu
Similaire à Ngu (20)
Dernier
Dernier (20)
Ngu
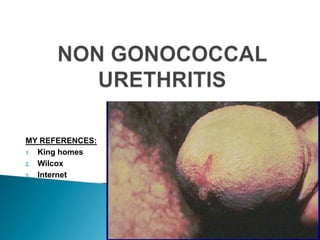
- 1. MY REFERENCES: 1. King homes 2. Wilcox 3. Internet
- 2. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. INTRODUCTION AND HISTORY DEFINITION AEITOLOGY CHLAMEDIA AND PGU MYCOPLASMA SYMPTOMS AND SIGNS IN MALE,FEMALE DIAGNOSIS TREATMENT AND FOLLOW UP COMPLICATIONS IN MALE AND FEMALE TREATMENT OF COMPLICATIONS
- 3. 1800, even prior to the discovery of N. gonorrhoea, the existence of several types of urethritis was already suspected. Gonorrhoea is known since Greek-roman period. Galen coined the word gonorrhoea 1880s◦ The isolation of N. gonorrhoea ◦ introduction of Gram stain ◦ differentiation of gonococcal from Non Gonococcal Urethritis.
- 4. Early part of the twentieth century◦ Intra cytoplasmic inclusions were seen in urethral smears of some men with urethritis suggesting Non gonococcal aetiology. Insight into the etiology of NGU ◦ Discovery of Ureaplasma urealyticum in 1954. 1965-the cell culture isolation techniques for C. trachomatis were developed. 1990-Nucleic acid amplification tests (NAATs) for sexually transmitted diseases (STDs).
- 5. Urethritis: ◦ Characterised by urethral discharge, dysuria, or itching at the end of the urethra, in the response of the urethra to inflammation, of any aetiology. Non gonococcal urethritis (NGU) : ◦ Urethritis caused by any aetiology other than N. gonorrhoea or wherein N.gonorhea is not detected. PGU : ◦ It is NGU occurring after curative therapy for gonorrhoea, is called postgonococcal urethritis (PGU).
- 6. Ch. trachomatis (15-40%) Mycoplasma genitalium (15-25%) OTHERS (20-50%) ◦ T Vaginalis ◦ U Urealiticum ◦ HSV (In absence of skin lesions) ◦ Adeno Virus ◦ Haemophilus
- 7. ◦ Miscellaneousin association with urinary tract infection, bacterial prostatitis, urethral stricture, phimosis, secondary to instrumentation of the urethra, congenital abnormalities, chemical irritation and tumors.
- 8. 13 mycoplasma species known to infect humans four are found in the genital tract: ◦ Mycoplasma hominis, ◦ M. genitalium, ◦ Ureaplasma parvum, and ◦ U. urealyticum.
- 9. Prevelence ◦ M. genitalium - 21.1% in men with chlamydia-negative NGU. ◦ U. urealyticum 18% ◦ U. parvum 9.9%
- 10. C. trachomatis first visualized -1907 by Halberstaedter and von Prowazek Isolated ◦ 25-60% (usually 30-40%) NGU, ◦ 4-35% (usually 15-25%) gonorrhea, ◦ 0-7% men without obvious urethritis Chlamydia pneumoniae -respiratory pathogen of humans, possible cause of CAD.
- 11. S.NO SPECIES SEROVAR DISEASE O1 C. PSITTACI 02 C. PNEUMONIAE 03 C.TRACHOMATIS L1, L2, L3 Lymphogranuloma venereum 04 C. TRACHOMATIS A, B, Ba, C Hyperendemic blinding trachoma 05 C. TRACHOMATIS B, D, E, F, G, H, I, J, K Inclusion conjunctivitis (adult and newborn), nongonococcal urethritis, cervicitis, salpingitis, proctitis, epididymitis, pneumonia of newborns Many unidentified Psitacosis TWAR Respiratory disease
- 12. C. trachomatis 15-40% of NGU. Rationale: ◦ Gonorrhea has a shorter incubation period 2-6days ◦ chlamydial IP 1-5 weeks ◦ so men with both infections can present with gonorrhea while the chlamydial infection is still incubating.
- 13. When gonorrhea is treated and do not eradicate C. trachomatis Hence, concurrently Chlamedial/NGU/PGU develops who have concurrent C. trachomatis infection. Hence PGU - provides assessment of the ability of C. trachomatis to produce urethritis.
- 14. Burning micturition, Dysuria Urethral discharge, meatitis, inguinal lymphadenitis. The symptoms and signs of GU and NGU are similar but differ significantly in severity. Both may cause urethral discharge, dysuria, or urethral itching.
- 15. Discharges - profuse and purulent in men with gonorrhoea, but are generally scanty and mucoid in men with NGU. Discharge may be detected only in the morning or noted as crusting at the meatus or as staining on underwear. Gonorrhoea usually develops 2-6 days after exposure, whereas NGU generally develops between 1 and 5 weeks after the acquisition of infection.
- 16. In urethritis caused by HSV and adenovirus, dysuria is severe. viral urethritis presents with meatitis, but is seen in a minority of cases caused by bacteria. Adenovirus cases tend to occur in the winter and often associated with conjunctivitis.
- 17. Following are seen with primary HSV urethritis. ◦ ◦ ◦ ◦ ◦ ◦ ◦ Regional lymphadenopathy, constitutional symptoms, pain in groin/leg/buttock, scanty discharge, disproportionate dysurea, intra-meatal ulcer, blood stained discharge Asymptomatic urethritis common in chlamydial infections. Constitutes a large reservoir of infection.
- 18. Atypical presentations of NGU a) Meatitis with urethral inflamation b) Lymphadinitis c) Periurethral abscess d) Associated disease manifestations ◦ classic urinary tract infection, ◦ acute prostatitis/flare-up of chronic prostatitis, ◦ acute epididymitis or orchitis hematuria, chills, fever, frequency, hesitancy, nocturia, urgency, perineal pain, scrotal masses, postvoid dribbling, genital pain other than dysuria.
- 19. Gram staining of discharge or sediment of First Voided Urine: (Symptomatic/asymptomatic) ◦ Absence of Gonnorheal Diplococci ◦ Presence of leukocytosis ◦ i.e.more than 5 PMNs per high power field.(in Minimum of 5 fields observed)
- 20. AND / OR Leukocyte esterase testing on FVU or gram stained specimen of centrifuged sediment of FVU with >10 PMNL/x1000 microscopic field. In pts who are symptomatic without evidence of urethritis (i.e., discharge on examination or the presence of PMNL in the stained urethral smear), non sexually transmitted causes of urethritis considered.(-like urinary tract infection)
- 21. Diagnostic Options Chlamydia • • • • Cell Culture Direct Fluorescence Assay Enzyme Immunoassay Hybridisation Assay • Nucleic Acid Amplification Tests
- 22. S.NO Disease 01 Clinical criteria Chlamedial Dysuria, urethral NGU discharge Presumptive diagnosis diagnostic Gram Stain, 5 or more PMN/high power field Or pyuria on FVU Positive culture or NAAT
- 24. • Diagnostic tests for U. ureaplasma, M. genitalium, and T. vaginalis either lack sensitivity or specificity. • Clinical circumstances, identification of C. trachomatis as the cause of NGU is not necessary, as recommended antibiotic therapy currently is the same for both chlamydiapositive and chlamydia negative NGU. (King Homes)
- 25. Disease may be asymptomatic (40%) On examination: • Minimal cervical mucoid/mucopurulent discharge (IUD in situ) • Cervical erosion/cervicitis(OCP users) • Microfollicles in cervical mucosa are diagnostic of chlamedial NGU.
- 26. Bartholinitis Salpingitis Salpingo-oophoritis (PID) Fitz Hugh Curtis syndrome Peritonitis Peri-hepatic adhesions On Glisson's capsule
- 27. Salpingitis is imp complication. ◦ B/L low abdominal pain, involving both adnexae ◦ Often with uterine bleeding, ◦ Constitutional symptoms: fever, headache, vomiting ◦ can lead to ectopic pregnency, Infertility
- 28. Gram stain of Cx smear is of little significance. As pus cells in Cx may even be seen physiologically. Numerous pus cells in absence of Gonococci, may be due to NGU. Male partner should be investigated for NGU.
- 29. STD treatment guidelines from the CDC 2010 and the World Health Organization currently recommends ◦ doxycycline 100 mg twice daily for 7 days. OR • Azithromycin 1G orally Alternatives ◦ Erythromycin base 500mg four times for 7days OR ◦ Ofloxacin 300mg twice daily for 7 days OR ◦ Levofloxacin 500 mg once daily for 7days
- 30. All Sex Partners In Last 60 Days Should Be Evaluated And Treated Sexual abstinence till completion of treatment. Pts with NGU reviewed 2-3 weeks after treatment to confirm resolution of symptoms and treatment of sexual contacts. Should be checked for other STIs including Syphilis and HIV,Results of tests checked during review.
- 31. Abstinence Avoid Self examination, squeezing urethra Ensure Hold visit. from alcohol during treatment partner treatment, and follow up. urine at least for 4 hours before next
- 32. 1 Week- repeat 2 glass test, repeat staining, check test reports. 2/3 week- check 2 glass test and stain smear, clear cured. 4/6weeks-Symptomatic for urethritis recurrent/relapse 3 months- check for syphilis
- 33. Epidydimo-orchitis Reiter's syndrome/sexually acquired reactive arthritis Urethral strictures. Prostatitis Chronic and refractory urethritis.
- 34. 1. Symptoms of urethritis+ O/E: supportive signs of urethritis The following should be checked: Abstinence- chance of re-infection Compliance/drug interaction eg: milk/liver enzyme inducers Self examination: Repeated/habitual milking of urethra by patient or H/O masturbation.
- 35. Wrong diagnosis: a. UTI b. Trichomonal urethritis Stricture: suspect in all chronic cases until proved otherwise. Neurosis: often seen in patients with habitual self examination.
- 36. 2. Iatrogenic: over enthusiastic treatment of pus cells during follow up in asymptomatic patients. Diagnosis: ◦ reinfection/ relapse suspected◦ 2 glass test -abnormal in both glass prostatitis as seat of infection suspect
- 37. Prostatic massage Prostatic massage Gram stain, AFB Culture from Mid Stream Urine (On three successive days) Urethroscopy and IVU- higher seated source of infection anterior urethroscopy 1. stricture 2. reassurance of neurotic patient 3. VUR/hydronephrosis/pyelonephritis
- 38. UTI: C&S followed by antibiotics Trichomoniasis: secnidazole 2g stat Stricture: urology for opinion and Rx Symptoms disproportionate to signs: ◦ Strong reassurance ◦ Test and Strong reassurance
- 39. Reported by Hans Reiter 1916. Described by sir benjamin brodie.
- 40. “Reiter’s Syn. is an infectious induced systemic illness characterized by an aseptic inflammatory joint involvement occurring in a genetically predisposed patient with a bacterial infection localized in a distant organ/system”. Incidence varies widely (1% to 20%). Consists of : ◦ Urethritis ◦ Conjuctivitis ◦ Asceptic arthritis
- 41. Cause unknown Post dysenteric and urethritis Chlamedia Trachomatis ◦ Shigellosis ◦ Salmonellosis ◦ Yersinia enterocolitica ◦ Campylobacter
- 42. h/o sexual exposure/diarhea within 4 weeks S/S Urethritis S/S Cystitis/prostatitis Eye: Conjuctivitis, Episcleritis, Iritis, superficial punctate keratitis, corneal ulceration.
- 43. Arthritis ◦ Recurrent attacks ◦ Constitutional symptoms ◦ Asymmetric polyarthritis ◦ Knee, ankle, feet, sacro-iliac joint. • Inflamation of achiles tendon (MC) • Plantar fascitis
- 44. •Pericarditis,myo carditis, aortic regurgitation •Pleurisy,pulm onary fibrosis •meningoencephalitis •Amyotropic lateral sclerosis •Circinate balanitis •urethritis Conjuctivitis, Episcleritis, Iritis, superficial punctate keratitis, corneal ulceration. Asymmetric polyarthritis Subungual keratosis Peripheral neuropathy sacro-ilitis •Keratoderma blenorrhagica Erosions tongue, palate Plantar fascitis
- 49. Associated with HLA B 27 anemia,leucocytosis, ESR >100 Normal- RA factor, ANA, ASO titre Synovial fluid- >Neutrophils 5-50 X ray => ◦ ◦ ◦ ◦ periosteal newbone formation Sacroiliac joint involvement Fluffy calcaneal spur Periosteitis at the insertion of plantar fasciae.
- 50. Topical steroids-conjunctivitis and uveitis. Urethritis – Rx NGU Keratoderma blenorrhagica-1% hydrocortisone
- 51. • • • Acute – Rest, analgesics- first line of treatment. Splint/ immobilisation Joint aspiration Physiotherapy Chronic/Recurrent • • • DMARDS- sulfasalazine or methotrexate axial involvement-benefit from TNF-alpha blockers. Monoarthritis- steroid injections.
- 52. Thank you
Notes de l'éditeur
- hematuria, chills, fever, frequency, hesitancy, nocturia, urgency, perineal pain, scrotal masses, postvoid dribbling, genital pain other than dysuria.
- NAAT- to identify CH and GN. Tryptophan synthetase coding gene id and responcible NA amplified to detect the organism.Eg. RT-PCR,LCR,Trascrption mediated amplification.ETC