
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à 1.6.2 Pharmacologic Treatment
Similaire à 1.6.2 Pharmacologic Treatment (20)
Plus de medicinaudm
Plus de medicinaudm (20)
Dernier
Dernier (20)
1.6.2 Pharmacologic Treatment
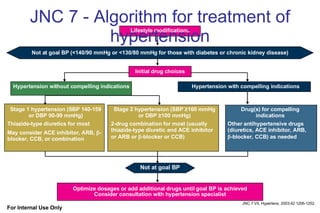
- 1. JNC 7 - Algorithm for treatment of hypertension Hypertension with compelling indications Stage 1 hypertension (SBP 140-159 or DBP 90-99 mmHg) Thiazide-type diuretics for most May consider ACE inhibitor, ARB, -blocker, CCB, or combination Stage 2 hypertension (SBP ≥160 mmHg or DBP ≥100 mmHg) 2-drug combination for most (usually thiazide-type diuretic and ACE inhibitor or ARB or -blocker or CCB) Drug(s) for compelling indications Other antihypertensive drugs (diuretics, ACE inhibitor, ARB, -blocker, CCB) as needed Not at goal BP Lifestyle modifications JNC 7 VII, Hypertens. 2003;42:1206-1252. Not at goal BP (<140/90 mmHg or <130/80 mmHg for those with diabetes or chronic kidney disease) Initial drug choices Hypertension without compelling indications Optimize dosages or add additional drugs until goal BP is achieved Consider consultation with hypertension specialist For Internal Use Only
- 2. ESH/ESC guidelines Pharmacological Treatment of Hypertension Consider : Blood pressure level before treatment Absence or presence of TOD and risk factors Two-drug combination at low dose Choose between : Single agent at low dose If goal BP not achieved : Previous agent at full dose Switch to different agent at low dose Previous combination at full dose Add a third drug at low dose If goal BP not achieved : Two-three drug combination Two-three drug combination ESH/ESC Guidelines. J Hypertens 2003; 21: 1011-1053 For Internal Use Only
- 11. First line therapy Compelling indication for others Compelling indication for others Compelling indication for others - 2 drug combo 2 drug combo Low dose Diuretics Any of 5 (A,A,B,C,D) Thiazide-type Diuretics WHO-ISH ESH-ESC JNC 7 For Internal Use Only JNC 7 Report . JAMA 2003; 289: 2560-2572 ESH/ESC Guidelines. J Hypertens 2003 ; 21: 1011-1053 Guidelines Sub-Committee. 1999 WHO/ISH. J Hypertens 1999; 17:151–183
- 12. Recommended combinations Di ACE I CCB ARB B B WHO-ISH ESH-ESC JNC VII Di + any Di + ACE I/ ARB/ CCB/ B For Internal Use Only JNC 7 Report . JAMA 2003; 289: 2560-2572 ESH/ESC Guidelines. J Hypertens 2003 ; 21: 1011-1053 Guidelines Sub-Committee. 1999 WHO/ISH. J Hypertens 1999; 17:151–183
- 14. SBP Control in Trials * 10604 M FACET Micro HOPE CAPPP INSIGHT HOT VALUE STOP-2 UKPDS LIFE RENAAL IDNT IRMA ABCD 130 140 150 160 170 180 190 200 mmHg 120 Diabetics B T ALLHAT 1 HOPE PROGRESS CAPPP INSIGHT NORDIL HOT STONE STOP-2 LIFE ALLHAT 2 ANBP2 INVEST SCOPE ASCOT VALUE All patients 130 140 150 160 170 180 190 200 mmHg B T * Most patients under ≥ 2 drugs Mancia G and Grassi G, J Hypert 2002;20:1461-1464 For Internal Use Only
- 15. Combination Therapy in Large Trials 0 10 20 30 40 100 90 80 70 60 50 Average VA SYST-EUR STOP-2 STOP-1 SHEP NORDIL MRC II MRC I MAPHY INSIGHT HOT 90 LIFE EWPHE COOPE ANBP 62% 100% 41% 55% 66% 45% 52% 51% 34% 48% 54% 60% 90% 35% 93% 33% % ALLHAT 41% INVEST 82% Updated from Coca A. J Cardiovasc Pharmacol 1999; 34 (Suppl 3): 29-35 For Internal Use Only
- 16. Multiple Antihypertensive Agents Are Often Needed to Achieve Target BP 1 No. of Antihypertensive Agents 2 3 4 SBP 140/DBP 90 ALLHAT 7 SBP 135/DBP 85 IDNT 6 MAP 92 AASK 5 DBP 80 HOT 4 MAP 92 MDRD 3 DBP 75 ABCD 2 DBP 85 UKPDS 1 Target BP (mm Hg) Trial DBP- diastolic blood pressure MAP - mean arterial pressure ; SBP- systolic blood pressure 1. UK Prospective Diabetes Study Group. BMJ. 1998;317:703-713. 2. Estacio RO et al. Am J Cardiol. 1998;82:9R-14R. 3. Lazarus JM et al. Hypertension. 1997;29:641-650. 4. Hansson L et al. Lancet. 1998;351:1755-1762. 5. Kusek JW et al. Control Clin Trials. 1996;16:40S-46S. 6. Lewis EJ et al. N Engl J Med. 2001;345:851-860. 7. ALLHAT. JAMA . 2002;288:2998-3007. For Internal Use Only
- 17. Compliance to Treatment Related to Daily Number of Pills Prescribed Average number of daily pills 0 10 20 30 40 50 60 70 1 2 3 8 Compliance to treatment (%) Mancia G et al. Am J Hypertens 1997 ; 10: 153S-158S For Internal Use Only
- 18. Fixed-dose Combination Therapy Increases Compliance to Treatment Persistence rates of one pill of lisinopril/HCTZ in fixed-combination vs two separate pills of lisinopril and HCTZ 100 95 90 85 80 75 70 65 60 55 50 0 1 2 3 4 5 6 7 8 9 10 11 12 Months Persistence (%) 68.7 57.8 18.8% Lisinopril/HCTZ (1 pill) Lisinopril and HCTZ (2 pills) Dezii CM . Manag Care 2000; 9 (Suppl): s2-s6 For Internal Use Only
- 21. The 3 Classes of Diuretics and Their Primary Sites of Action in the Nephron For Internal Use Only Adapted from: Oparil S and Weber MA. Hypertension.Elsevier/Sanders 2nd ed. 2005; L ip G and Bakris G. Handbook Hypertension Management. CMG 2006
- 25. The Mechanism of Calcium-Channel Blockade For Internal Use Only Adapted from: Oparil S and Weber MA. Hypertension.Elsevier/Sanders 2nd ed. 2005; L ip G and Bakris G. Handbook Hypertension Management. CMG 2006
- 28. The Mechanism of Beta-Blockade Reduced cardiac output Reduced blood pressure Impulse Smooth muscle presynaptic sympathetic neurons Cardiac tissue (contains beta 1 receptors) Increased bronchial resistance and vasoconstriction Impulse Smooth muscle presynaptic sympathetic neurons Tissue of the peripheral blood vessels, smooth muscle cells or lungs (contains beta 2 receptors) Beta-blocker Nonadrenaline or adrenaline Beta 1 receptors Beta 2 receptors Reduced heart rate and force of constriction Beta 1 receptor blocked by beta-blocker Beta 2 receptor blocked by beta-blocker Adapted from: Oparil S and Weber MA. Hypertension.Elsevier/Sanders 2nd ed. 2005; L ip G and Bakris G. Handbook Hypertension Management. CMG 2006 For Internal Use Only
- 31. The Mechanism of Alpha-Blockade Total peripheral resistance increased Blood Pressure rises Constriction of blood vessel Impulse Smooth muscle presynaptic sympathetic neurons Vascular smooth muscle cell Total peripheral resistance decreased Blood pressure falls Blood vessel remains dilated Impulse Smooth muscle presynaptic sympathetic neurons Alpha 1 receptor blocked so muscle cells do not contract Alpha 1 receptor blocker Nonadrenaline or adrenaline Alpha 1 receptors Alpha 2 receptors For Internal Use Only Adapted from: Oparil S and Weber MA. Hypertension.Elsevier/Sanders 2nd ed. 2005; L ip G and Bakris G. Handbook Hypertension Management. CMG 2006
- 33. The Mechanism of Action of ACE-inhibitors Angiotensin I Bradykinin ACE Inhibitor ACE (from lungs) Angiotensinogen (from liver) Renin (from kidney) Angiotensin II Inactive kinins Vasodilation Blood pressure decreases Retention of salt and water Increased aldosterone Increased blood volume Increased total Peripheral resistance Vasoconstriction Blood pressure increase Bradykinin pathway RAA System For Internal Use Only Adapted from: Oparil S and Weber MA. Hypertension.Elsevier/Sanders 2nd ed. 2005; L ip G and Bakris G. Handbook Hypertension Management. CMG 2006
- 35. Mechanism of Action of Angiotensin II Receptor Blockers (ARBs) Adapted from Unger T. Am J Cardiol 2002; 89 (suppl):3A-10A. AT 1 Receptor Na reabsorption Aldosterone release Sympathetic outflow Vasopressin secretion Vasoconstriction Vascular and cardiac hypertrophy Angiotensinogen Angiotensin I Angiotensin II Non-ACE enzymes (cathepsin, chymase) Renin Bradykinin ACE Inactive Fragments AT 2 Receptor Vasodilation Growth inhibition Apoptosis Blood Pressure ARBs For Internal Use Only
- 36. Pharmacologic Characteristics of ARBs HTN HTN, post MI, CHF HTN HTN, Nephropathy T2DM + HTN, Morbi-Mortality reduction and stroke prevention in HTN with LVH HTN HTN, CHF HTN, Nephropathy T2DM + HTN Indications Digoxin no no Rifampin, Fluconazole no no no Drug interract 24h 6h 12-18h 2h 5-9h 9h 11-15h T 1/2 Minimal yes none minimal yes none none Food effect 0.5-1h 2-4h 1-2h 3-4h 3h 3-4h 1.5-2h Tmax 42-58% 25% 26% 33% 13% 15% 60-80% Bioavail Boeh Ingelh Novartis/ Beaufour Menar/Sank MSD Solvay AstZen/Tak SA/BMS Company Telmisartan (Micardis) Valsartan (Diovan) Olmesartan (Benicar) Losartan (Cozaar) Eprosartan (Teveten) Candesartan (Atacand) Irbesartan (Avapro/ Aprovel) For Internal Use Only Oparil S and Weber MA. Hypertension.Elsevier/Sanders 2nd ed. 2005; L ip G and Bakris G. Handbook Hypertension Management. CMG 2006
Notes de l'éditeur
- GLB.IRB.06.12.01