Epistemic Problems in Critical Care Medicine

This document discusses epistemic problems in critical care medicine research. It notes that for interventions with less obvious or immediate effects, evidence from clinical trials is important due to uncertainty. However, many such trials in critical care have problems with non-repeatable positive results and inadequate study power to detect realistic treatment effects. This leads to a situation where the null hypothesis of no treatment effect has stochastic dominance. The document argues that commonly used research practices like setting a low threshold for statistical significance, aiming for high study power, and accurately estimating expected treatment effects are often not followed, undermining the strength of evidence even from large trials.
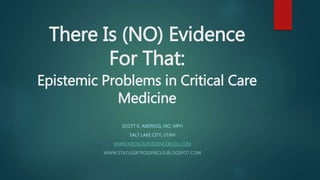
![What Constitutes Knowledge (A
Justified True Belief)?
From Therapeutic Agnosticism: Stochastic Dominance of the Null Hypothesis
Category 1:
ARR high [NNT low]
“Visible” & immediate effects
Causal Pathways “Obvious”
Type I diabetes DKA
Insulin Resolution of DKA
Trials “unethical” – No Equipoise –
High Prior Probability for Ha
Category 2:
ARR low(er) [NNT high(er)]
“Invisible” & delayed effects
Associations Prevalent, CPs Obscure
ICU Hyperglycemia ???
Insulin resolution of hyperglycemia
Trials imperative – Equipoise - Low(er) Prior
Probability for Ha](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (7)
Similaire à Epistemic Problems in Critical Care Medicine
Similaire à Epistemic Problems in Critical Care Medicine (20)
Plus de SMACC Conference
Plus de SMACC Conference (20)
Dernier
Dernier (20)
Epistemic Problems in Critical Care Medicine
- 1. There Is (NO) Evidence For That: Epistemic Problems in Critical Care Medicine SCOTT K. ABEREGG, MD, MPH SALT LAKE CITY, UTAH WWW.MEDICALEVIDENCEBLOG.COM WWW.STATUSIATROGENICUS.BLOGSPOT.COM
- 2. What Constitutes Knowledge (A Justified True Belief)? From Therapeutic Agnosticism: Stochastic Dominance of the Null Hypothesis Category 1: ARR high [NNT low] “Visible” & immediate effects Causal Pathways “Obvious” Type I diabetes DKA Insulin Resolution of DKA Trials “unethical” – No Equipoise – High Prior Probability for Ha Category 2: ARR low(er) [NNT high(er)] “Invisible” & delayed effects Associations Prevalent, CPs Obscure ICU Hyperglycemia ??? Insulin resolution of hyperglycemia Trials imperative – Equipoise - Low(er) Prior Probability for Ha
- 3. Examples: Category 1: No Evidence? Parachutes for Gravitational Challenge Oxygen for severe hypoxia Mechanical Ventilation Antibiotics for sepsis IVF for dehydration Insulin in DKA Knee Replacement Category 2: Evidence? Efficacy of Parachute A versus Parachute B Normocapnia; Heliox Low tidal volume ventilation Duration of antibiotic therapy “Goal Directed Therapy”, fluids for sepsis Anytensive insulin therapy in CCM Arthroscopy scams and shams
- 4. There Is Evidence for…
- 5. Two Problems in Category 2 Therapies in Critical Care Non-repeatability of Positives “Journal Club Biases” Conflict of Interest Single Center (Crabbe Effect) Early Stopping (benefit/futility) Multiple Comparisons Regression to mean/Decline effect Lack of blinding Publication bias “Flexibility” Nothing Works in CCM Stochastic Dominance of the Null Hypothesis Inadequate Study Power/Delta Inflation
- 6. Stochastic Dominance of the Null Hypothesis: The ARDSnet Population of Studies KARMA, n=234, standard , β, δ Stopped for futility n=234, δ(observed) = 1.0%, p=.85 ARMA, n=861, standard , β, δ Stopped for efficacy, n=861, δ = 8.8%, p=0.007 LaSRS, n=180, standard , β; δ 15%, revised mid-study to 20% because of low enrollment Observed δ 0.6%, P=1.0 FACTT, n=1000, standard , β, δ Observed δ 2.9%, p=0.30 ALVEOLI, n=549, standard , β, δ Stopped early; Observed δ 2.6, p=0.48 ARDSnet II ALTA EDEN OMEGA SAILS This “Population” of hypotheses is dominated by Ho; Ho not rejected 90% of the time
- 7. Prior probability of Ho = 1- Ha Held, BMC Medical Research Methodology 2010, 10:21 “A nomogram for p-values” http://www.biomedcentral.co m/1471-2288/10/21 Minimum posterior probability of Ho; 1-Ho = Maximum posterior probability of Ha
- 9. What Ought to be Type I error rate selected – significance threshold - (alpha) Type II error rate selected – Study power – 1-β Estimate of baseline event rate in control group Estimate of treatment effect size – δ (delta) What is 0.05 by convention (Statistical Methods for Research Workers; Fisher, 1925) Usually 80 +/- 10% - dual significance hypothesis testing Prior data consulted for baseline event rate estimate Estimate made of how many patients it is feasible to enroll. Delta back- extrapolated from this number – power calculation in reverse. 10% generally used
- 10. Delta Inflation is to Research as Grade Inflation is to Academics
- 11. NICE SUGAR36 Van Den Berghe9 Bernard11 Brower6 Fagon4 Esteban18 Rivers10 Ronco5 Schiffl13 Predicted Delta (%)
- 12. Conclusions Knowledge has many forms and heirarchies of knowledge are artificial and epistemically dubious (Sorry, User’s Guides.) We face a dual problem of methodologically inadequate positive studies and the “intractability of mortality” in adequate studies Ho has stochastic dominance in critical care research Bayesian analysis reveals that the “strength” of our evidence is much less than we presume The solution to inadequate power, double significance hypothesis testing, has been subverted by delta inflation (both premeditated and subconscious) Saying “There is no evidence for that” is meaningless Saying “There is evidence for XYZ” is equally meaningless