Cardiac murmur 2011-13 management guide
•
36 j'aime•20,803 vues

Neonatal guidelines NHS 2011 2013

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Cardiac murmur 2011-13 management guide
Similaire à Cardiac murmur 2011-13 management guide (20)
Plus de palpeds
Plus de palpeds (8)
Dernier
Dernier (20)
Cardiac murmur 2011-13 management guide
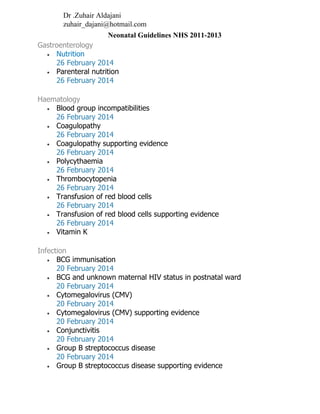
- 1. Cardiac murmur 2011-13 Symptomatic or >grade 3* murmur or signs Normal Cardiac murmur detected at routine postnatal examination In grade 1–3* systolic murmurs only, asymptomatic 24–36 hr after examination Oximetry on right arm and leg Check femoral pulses SpO2 ≥95% SpO2 <95% Review in 18–24 hr Check femorals again No murmur and normal femorals Murmur persists and normal femorals Before discharge: Pulse oximetry Check femorals Inform parents to watch for poor feeding, poor weight gain, breathing difficulties, colour change Paediatric follow-up in 2 weeks Murmur persisting but asymptomatic, keep under review Transfer to NNU for ECG, CXR and echo (if available). Contact cardiologist Abnormal Absent femorals Discharge Symptomatic or >grade 3* refer to paediatric cardiologist Repeat oximetry Symptoms • Tachypnoea or abnormal breathing pattern • Not taking feeds • Slow to feed (>30 min) • Sweaty or tachypnoeic during feeds • Colour change Signs of congenital heart disease • Central cyanosis • Tachypnoea • Other respiratory distress • Tachycardia • Hyperdynamic precordium • Abnormal volume or character of pulse • Hepatomegaly • Abnormal heart sounds • Heart murmur • Absence of femoral pulses CARDIAC MURMURS * Grade 1 – barely audible Grade 2 – soft but easily audible Grade 3 – moderately loud, no thrill Grade 4 – louder, with thrill Grade 5 – audible with stethoscope barely on the chest Grade 6 – audible with stethoscope off the chest Dr. Zuhair Aldajani zuhair_dajani@hotmail.com Neonatal Guidelines NHS 2011-2013
- 2. Cyanotic 2011-13 CYANOTIC CONGENITAL HEART DISEASE INCLUDING HYPOPLASTIC LEFT HEART SYNDROME (HLHS) (AND OTHER DUCT-DEPENDENT LESIONS DIAGNOSED ANTENATALLY) DEFINITION ‛Blue’ refers to central cyanosis (e.g. colour of tongue and gums). It is very difficult to see with the naked eye before the ductus arteriosus reaches a critical closing point Any baby presenting as blue has a critically small or closed duct and is a neonatal emergency requiring consultant input. These babies can deteriorate very quickly Differential diagnosis Without echocardiography, clinical distinction between persistent pulmonary hypertension (PPHN) and a duct-dependent pulmonary circulation can be extremely challenging Lungs • Persistent pulmonary hypertension of newborn • Congenital diaphragmatic hernia • Congenital lung lesions (e.g. pulmonary lymphangiectasia) Heart • Obstruction of blood flow from heart to lungs • Obstruction of blood flow from lungs to heart • Mixing oxygenated and deoxygenated blood • Total disconnection of pulmonary and systemic circulations SYMPTOMS AND SIGNS IN CARDIAC DISEASE • Central cyanosis • Usually limited signs of respiratory distress • Murmur, in the minority • Hepatomegaly • Poor perfusion INVESTIGATIONS • Chest X-ray • oligaemia/plethora/congenital anomaly • ‘classic’ appearance (e.g. ‛boot shaped’ heart) is unusual • Blood gas including lactate • Echocardiogram • 4-limb BP (>20 mmHg difference between an upper and lower limb is abnormal) • Pre- and postductal saturations (saturation of <95% in both limbs or >3% difference is significant) • Nitrogen washout test (carries risk of duct closure: discuss with consultant first) to differentiate between respiratory (parenchymal) and cardiac cause of cyanosis including PPHN • baseline saturation (and blood gas if arterial line in-situ) • place baby in 100% ambient oxygen for 10 min • if there is respiratory pathology, saturations should rise to >95% IMMEDIATE MANAGEMENT Resuscitation Call consultant A cardiac baby presenting collapsed and/or cyanosed is a challenging neonatal emergency
- 3. Cyanotic 2011-13 Airway • Intubate and ventilate all babies presenting profoundly cyanosed or collapsed • If apnoea occurs secondary to a prostaglandin infusion, intubate baby but do not alter infusion Maintain ductal patency • Open duct with dinoprostone (prostaglandin E2, prostin E2) • Start at 5 nanogram/kg/min, may be increased to 40 nanogram/kg/min on advice of cardiologist • if dinoprostone not available, use prostaglandin E1 (Alprostadil); see local formulary • Make fresh solution every 24 hr • Be vigilant: 10% will develop apnoeas on this low dose regimen Ventilation Indications • Significant apnoeas • Congestive cardiac failure • Respiratory failure Technique • Avoid hyperventilation, which can increase pulmonary blood flow • initial settings: PEEP 4–5 cm H2O and FiO2 0.21, adjusted accordingly • Aim for: • PaCO2 5–7 KPa • PaO2 4–6 KPa • pH 7.35–7.40 • SpO2 75–90%, although many will run higher in room air Inotropes • If signs of peripheral underperfusion persist, arrange local echocardiography (if available) to assess contractility • if confirmed, start dobutamine 5–10 microgram/kg/min by continuous IV infusion • if no improvement to peripheral circulation, consider nitroprusside 0.5–8 microgram/kg/min by continuous IV infusion after discussion with cardiac team Monitor • Monitor blood pressure invasively using a peripheral arterial cannula, not UAC • Titrate infusion to keep to SpO2 >75–90% • need to balance pulmonary and systemic circulations: too high an SpO2 compromises LV output and worsens hypotension • Assess cardiac output, likely to be low when: • tachycardia persists • BP remains low • acidosis persists • lactate elevated or rising • poor peripheral perfusion • When cardiac output low: • ensure prostaglandin infusion adequate • ensure adequate intravascular volume • correct anaemia • inotropes (dobutamine) may be required for tissue oxygen delivery and hypotension (as usually started for elevated lactate and reduced perfusion long before hypotension arises) SUBSEQUENT MANAGEMENT TRANSFER It is imperative that baby is kept warm and normoglycaemic
- 4. Cyanotic 2011-13 • Discuss further management and transfer with regional cardiac centre • Babies who respond to a prostaglandin infusion do not need to be transferred out-of- hours • Appropriately skilled medical and nursing staff are necessary for transfer Intubation Do not intubate routinely for transfer An intubated baby requires a cardiac centre ITU bed • Intubate if: • continuing metabolic acidosis and poor perfusion • long-distance transfer necessary • significant inotropic support in sick baby needed • apnoea • recommended by cardiac team DISCHARGE FROM CARDIAC CENTRE Patient may go home or return to a paediatric ward or neonatal unit Management plan • Regardless of outcome, obtain a management plan from cardiac centre, defining: • medication, including dosage • acceptable vital signs (e.g. saturations) • follow-up arrangements HYPOPLASTIC LEFT HEART SYNDROME (HLHS) (AND OTHER DUCT-DEPENDENT LESIONS DIAGNOSED ANTENATALLY) BACKGROUND • Malformation affecting left ventricle, aorta and valves • Degree of hypoplasia varies considerably and, in many cases, lesion is dynamic with progression during pregnancy • Recently palliative/corrective surgery (Norwood procedure and its modifications) has become increasingly successful in prolonging survival with a view to later heart transplantation ANTENATAL MANAGEMENT • Record management plan in mother’s notes and in antenatal counselling letter (with additional copy of both on neonatal unit) • After delivery and stabilisation at local maternity unit, arrange non-urgent transfer to regional cardiac surgery centre for full cardiology assessment • If closed or small (restrictive) atrial septum puts fetus at risk of severe pulmonary congestion and hypoxaemia shortly after birth, urgent septostomy immediately after delivery at maternity unit may be recommended, despite a generally poor outcome Postnatal diagnosis • Some babies will present when duct closes, anytime during neonatal period and early infancy, particularly where a left heart lesion has developed later in gestation It is important to consider diagnosis of HLHS in any baby presenting with ‛shock’
- 5. Cyanotic 2011-13 MANAGEMENT Aim to maintain patency of (or open a closed) ductus arteriosus, and optimise systemic perfusion • In HLHS, single right ventricle supplies blood to systemic and pulmonary circulations . Excess flow in one circulation will lead to a significant decrease in blood supplied to other circulation • Greatest risk is excessive blood flow through pulmonary circulation with systemic underperfusion, presenting with: • tachypnoea; • poor peripheral perfusion; and • metabolic acidosis • Poor peripheral perfusion can lead to cerebral injury and necrotising enterocolitis (NEC) Resuscitation • Neonatal team must be present at delivery to ensure baby establishes effective respirations and becomes pink • Although no increased requirement for resuscitation, it is extremely important to avoid hypoxia and hyperoxia • If stable, allow short cuddle with parents before transfer to neonatal unit, but keep warm to avoid hypothermia • Admit to unit for routine monitoring and investigations including blood gases and avoid acidosis FURTHER MANAGEMENT See Cyanotic congenital heart disease section of this guideline
- 6. ECG abnormalities 2011-13 ECG ABNORMALITIES SINUS TACHYCARDIA Recognition and assessment • Sinus rhythm (P wave precedes every QRS complex) with a heart rate above normal limit for age and gestation Causes • Fever • Infection • Low haemoglobin • Pain • Hypovolaemia • Hyperthyroidism • Myocarditis • Drugs (e.g. caffeine and salbutamol) Management • Treat the cause SINUS BRADYCARDIA Recognition and assessment • Sinus rhythm (P wave precedes every QRS complex) with a heart rate below normal limit for age and gestation Differential diagnosis • Hypoxia (most likely cause) • Vagal stimulation (ET tube touching carina) • Post-intubation • Hypovolaemia • Hypothermia • Metabolic derangement Immediate management • Manage airway and breathing • Adjust ET position, if too low • If post-intubation, use atropine (see Neonatal Formulary) • Correct hypovolaemia • Correct metabolic derangement • If persistent, obtain 12-lead ECG PREMATURE ATRIAL BEAT Recognition and assessment • Most common form of arrhythmia • In a regular sinus rhythm at a normal rate, a P wave occurring before next expected P wave is a premature atrial beat • Most premature atrial beats are benign Investigations • 12-lead ECG PREMATURE VENTRICULAR BEAT Recognition and assessment • Premature abnormal QRS complex not preceded by a premature P wave
- 7. ECG abnormalities 2011-13 Investigations • 12-lead ECG • Measure QTc interval on ECG during period of sinus rhythm • Echocardiogram to rule out structural abnormality of heart Immediate treatment • Seek advice from paediatric cardiologist SUPRAVENTRICULAR TACHYCARDIA Recognition and assessment • Rapid regular tachyarrhythmia • Heart rate >230/min • ECG: • P waves commonly absent. When present, almost always have a different morphology • narrow QRS complex • in fast sinus tachycardia, P waves can be very difficult to see • look for delta waves consistent with Wolff-Parkinson-White syndrome as this affects the choice of anti-arrhythmic agent used by cardiologists at Birmingham Children’s Hospital (BCH) Symptoms and signs • Persistent SVT can cause haemodynamic compromise Investigations • 12-lead ECG to document SVT: if not definite SVT, treat for cause of sinus tachycardia (e.g. fluid for hypovolaemia) Immediate management • Assess airway, breathing and circulation • Check for signs of cardiac failure • Vagal manoeuvre such as applying ice pack to face • Adenosine IV bolus • use central venous access or IV access in a bigger vein (antecubital fossa) • connect 3-way connector to end of cannula/catheter • establish patency of IV access • connect syringe with adenosine to one port and sodium chloride 0.9% flush to another port • run ECG strip • give adenosine as a quick bolus and push the bolus of sodium chloride 0.9% at the end quickly • document change in cardiac rhythm on ECG Adenosine dosage • Start with 150 microgram/kg IV bolus • if no response, increase by 50 microgram/kg • Repeat every 1–2 min • maximum dose 300 microgram/kg • If no response, discuss with BCH cardiologists regarding DC shock Subsequent management • Echocardiogram to assess ventricular function and presence of congenital heart disease • Correct electrolyte and metabolic imbalance, if present • Discuss with paediatric cardiology centre for further management or earlier if necessary VENTRICULAR TACHYCARDIA Recognition and assessment • Heart rate >200/min
- 8. ECG abnormalities 2011-13 • Wide QRS complexes Immediate management • Manage airway and breathing • Correct hypoxia • Correct electrolyte disturbance • Discuss with paediatric cardiology centre • Consider synchronised cardioversion (in very fast heart rates, defibrillators cannot synchronise with the patient and unsynchronised will be required) if intubated, with analgesia • Amiodarone 5 mg/kg over 30 min IV (repeat if necessary) • If no response, lidocaine 0.5–1 mg/kg IV. May be repeated after 5 min TACHYARRHYTHMIA • True heart rate? • Is baby crying/in pain? • Check airway and breathing • Check saturation • Consider arterial/capillary gas • Check perfusion • Check blood pressure • Manage airway and breathing • Correct hypoxia • Correct electrolyte disturbance 12 lead ECG12-lead ECG • Narrow QRS complex • Absent/abnormal P wave • vagal manoeuvres • adenosine • discuss with paediatric cardiologist • consider synchronised cardioversion • Broad QRS complex • Abnormal P wave • discuss with paediatric cardiologist • synchronised cardioversion
- 9. Heart failure 2011-13 HEART FAILURE DEFINITION • Congestive cardiac failure occurs when heart unable to pump sufficient blood to meet metabolic demands of body tissues • cause may be cardiac or non-cardiac Causes Non-cardiac • Sepsis • Asphyxia • Anaemia • Polycythaemia • Fluid overload • AV malformation • Bronchopulmonary dysplasia (BPD) Cardiac • Left ventricular outflow tract (LVOT) obstruction • Left-to-right shunt (see Increased left to right shunt below) • Arrhythmia Left ventricular outflow tract obstruction (LVOT) • Hypoplastic left heart syndrome • Critical aortic stenosis • Coarctation • Interrupted aortic arch SYMPTOMS AND SIGNS OF CARDIAC FAILURE • Tachycardia • Tachypnoea • Hepatomegaly • Excessive weight gain • Hypotension • Murmur • Abnormal femoral pulses • in obstructive left heart lesions, femoral pulses may not be absent if duct still patent • weak femoral pulses are significant INVESTIGATIONS • Blood gas including lactate • Chest X-ray • cardiomegaly and pulmonary oedema • Echocardiogram • Four-limb BP (a difference of >20 mmHg between an upper and lower limb is significant) • Pre- and postductal saturations • postductal saturations can be considerably lower than preductal in aortic arch defects (a difference of >3% is significant) IMMEDIATE TREATMENT Clinical differentiation between an obstructed systemic circulation and severe sepsis is extremely difficult as a murmur and weak pulses can be common to both. In infant in extremis, presence of abnormal pulses alone is sufficient indication to start a prostaglandin infusion until a cardiac lesion has been excluded by echocardiography If left sided obstructive lesion suspected, treat with inotropes and use diuretics cautiously
- 10. Heart failure 2011-13 Resuscitation Airway • Intubate and ventilate babies presenting collapsed or with obvious cyanosis in association with cardiac failure • Routine intubation not indicated • If apnoea occurs secondary to a prostaglandin infusion, intubate baby but do not alter infusion Breathing • See Ventilation guideline • Ventilate with PEEP 5–6 cm • Adjust ventilation to maintain: • PaCO2 5–6 kPa • pH ≤7.4 Circulation • Vascular access with 2 IV cannulae or umbilical venous catheter (UVC) – See Umbilical venous catheterisation guideline Presence of cyanosis and a murmur suggest baby likely to respond to prostaglandin infusion • Prostaglandin infusion to maintain ductal patency • open duct with dinoprostone (prostaglandin E2, prostin E2), see Neonatal Formulary. Start at 5 nanogram/kg/min, may be increased to 40 nanogram/kg/min, but only on advice of cardiologist • alprostadil (prostaglandin E1 can also be used. Start at 5 nanogram/kg/min, may be increased but only on advice of cardiologist • Monitor blood pressure invasively using a peripheral arterial cannula, not umbilical arterial catheter (UAC) • need to balance pulmonary and systemic circulations: too high an SpO2 compromises LV output and worsens hypotension – seek advice from cardiologist Cardiac output • Assess cardiac output, it is likely to be low when: • tachycardia persists • BP remains low • acidosis persists • high lactate • peripheral perfusion poor • ensure prostaglandin infusion adequate • When cardiac output low: • ensure adequate intravascular volume • correct anaemia • dobutamine will be required for poor perfusion SUBSEQUENT MANAGEMENT – TRANSFER Baby must be kept warm and normoglycaemic • Discuss further management and transfer with regional cardiac centre • Babies who respond to a prostaglandin infusion do not need transferring out-of-hours • Appropriately skilled medical and nursing staff are necessary for transfer Intubation An intubated baby requires a cardiac centre ITU bed: do not intubate routinely for transfer
- 11. Heart failure 2011-13 • Intubate if: • continuing metabolic acidosis and poor perfusion • long-distance transfer necessary • inotropic support needed • apnoea occurring • recommended by cardiac team DISCHARGE FROM CARDIAC CENTRE Patient may go home or return to a paediatric ward or neonatal unit, possibly on a prostaglandin infusion whilst awaiting surgery or for continuing care after a palliative procedure (e.g. septostomy) Management plan • Regardless of outcome, obtain a management plan from cardiac centre, defining: • acceptable vital signs (e.g. saturations) • medication, including dosage • follow-up arrangements INCREASED LEFT TO RIGHT SHUNT RECOGNITION AND ASSESSMENT Definition • Any lesion causing increased pulmonary blood flow • Usually presents when pulmonary resistance falls after 48 hr • Size and type of lesion will influence time of presentation Differential diagnosis • AVSD • Partial AVSD • VSD • Truncus arteriosus Investigations • Chest X-ray looking for fluid overload • Echocardiogram MANAGEMENT • If in cardiac failure, give immediate dose of diuretic • May require maintenance diuretics (discuss with cardiologist) • usually furosemide 1 mg/kg and amiloride 100 microgram/kg orally • Discuss with cardiac centre for definitive management and follow-up
- 12. Hypotension 2011-13 HYPOTENSION Hypovolaemia is an uncommon cause of hypotension in the preterm newborn. Excessive volume expansion can increase mortality DEFINITION Thresholds for intervention • Aim to maintain mean arterial BP >gestational age in weeks • If mean BP unavailable or pulse pressure wide (e.g. PDA), aim to maintain systolic BP >gestational age in weeks in first 24 hr, and >30 mmHg thereafter • Aim for even higher mean arterial blood pressure in case of persistent pulmonary hypertension of newborn – see PPHN guideline RECOGNITION AND ASSESSMENT Assessment of BP • Measure mean arterial pressure (MAP): • by direct intra-arterial BP [umbilical arterial catheter (see Umbilical artery catheterisation guideline) or peripheral arterial line if trace satisfactory] • automated oscillometry (Dinamap) has limited accuracy in hypotensive preterm neonates; usually over-reads BP in the lower ranges • Assess as many of the following indices of tissue perfusion as possible (thresholds for abnormality in brackets): • toe-core temperature difference (>2o C) • urine output (<1 mL/kg/hr) • blood lactate (>2.5 mmol/L) Causes of hypotension or poor perfusion • Cardiac dysfunction or hypovolaemia owing to: • extreme immaturity • hypoxia • pneumothorax • hypothermia • morphine analgesia • bleeding • polyuria secondary to glucosuria • Sepsis IMMEDIATE TREATMENT Aim of treatment is to improve organ perfusion, not to correct a ‘BP reading’ Seek senior advice throughout Transilluminate chest to exclude pneumothorax Fluid • Not >10 mL/kg unless there is evidence of fluid/blood loss and hypovolaemia • If clinical condition poor, BP very low, or mother has been treated with IV antihypertensive agent, give inotrope (see below) after fluid bolus Which fluid? • Use sodium chloride 0.9% 10 mL/kg over 30 min EXCEPT when there is: • coagulopathy with bruising: give fresh frozen plasma 10 mL/kg over 30 min (see Coagulopathy guideline ) • Acute blood loss: give packed cells 10 mL/kg over 30 min Reassess clinically within 30 min of each bolus
- 13. Hypotension 2011-13 • If hypotension persists after fluid bolus, seek senior advice • start inotropes Inotropes • If evidence of poor perfusion, give dobutamine as initial agent commencing at 10 microgram/kg/min. If no response after 20 min, increase to 15 microgram/kg/min Always use dobutamine as first inotrope for pulmonary hypertension • Dobutamine will have now improved organ perfusion, but if mean BP remains low, commence dopamine at 5 microgram/kg/min, increasing by 5 microgram/kg/min increments in 30 min intervals to a maximum of 20 microgram/kg/min • where possible, perform echocardiogram to assess response to dopamine at doses >10 microgram/kg/min • If hypotensive but peripheral perfusion good or bounding, as in sepsis, consider dopamine as initial inotrope after fluid bolus, as this will cause vasoconstriction that will help alleviate poor vascular tone seen with sepsis How • Dopamine must be given centrally because: • can cause tissue injury if given into liver or extravasation injury if given peripherally • Dobutamine is best given centrally, although can be given peripherally Continuing hypotension • If hypotension persists despite these measures: • give hydrocortisone 1 mg/kg IV followed by 1 mg/kg IV 8–12 hrly for 2–3 days as necessary • seek senior advice throughout Refractive hypotension Seek senior advice before starting adrenaline infusion. Depending on individual circumstances, discuss alternative agents (e.g. noradrenaline, vasopressin) If acidotic with severe hypotension, but not hypovolaemic • Give adrenaline 100–300 nanogram/kg/min (see Neonatal Formulary for instructions on making up solution) • Monitor limb perfusion and urine output If cooling, refer to Cooling guideline and avoid vasoconstrictive agents which further reduce peripheral perfusion DO NOT USE ADRENALINE in cooled infants MONITORING • If pneumothorax suspected, transilluminate • Chest X-ray: • if intubated • urgent, if respiratory status worsening • look for air leak or overinflation • Blood gases • Check effective delivery of drugs: • record volume in syringe hourly • check for leaks • ensure correct position of umbilical venous catheter (UVC) delivering inotropes SUBSEQUENT MANAGEMENT • If being given morphine, reduce dose if possible
- 14. Hypotension 2011-13 • If ventilated, try to reduce mean airway pressure without compromising chest inflation and oxygenation • If poor response to above measures: • echocardiogram to assess for myocardial dysfunction/congenital heart disease Weaning inotropes • Wean dopamine or dobutamine in 5 microgram/kg/min decrements as tolerated and directed by senior advice
- 15. PDA 2011-13 PATENT DUCTUS ARTERIOSUS RECOGNITION AND ASSESSMENT Definition • Patent ductus arteriosus (PDA) is the continuation of blood flow through the duct following birth • Persistent PDA is failure of functional closure of duct by 48 hr or of anatomical closure by 3 weeks Factors associated with delayed closure • Early gestation • Lack of antenatal corticosteroid prophylaxis where indicated • Surfactant-deficient lung disease • Hypoxaemia • Volume overload Adverse effects of PDA • Can become manifest in first 48 hr • Significant right-to-left shunt and hypoxia until pulmonary pressure falls • Reduced systemic blood flow leading to acidosis and hypotension • Increased pulmonary blood flow leading to increased work of breathing • Pulmonary haemorrhage • Intraventricular haemorrhage and cerebral ischaemia (steal) Symptoms and signs • Can be absent in a clinically significant duct for first 7 days of life • Significant left-to-right shunt suggested by: • active praecordium • full pulses • wide pulse pressure • murmur • hypotension • hepatomegaly • oedema • Significant right-to-left shunt suggested by: • hypoxia Differential diagnosis • Other cardiac pathology • physiological left pulmonary branch stenosis • ventricular septal defect • atrial septal defect/patent foramen ovale • Sepsis • Right-sided cardiac pathology secondary to lung disease INVESTIGATIONS • Palpation of femoral pulses • Pre and post ductal SpO2 monitoring • Chest X-ray: • cardiomegaly • pulmonary plethora • Echocardiography • not essential but advisable because duct-dependent cardiac lesion can be difficult to detect clinically • important, if considering treatment with prostaglandin inhibitor, to assess cardiac anatomy and ductal status
- 16. PDA 2011-13 IMMEDIATE TREATMENT • Restrict fluid intake to <150 mL/kg/day Prostaglandin inhibitor to initiate ductal closure • Indometacin or ibuprofen • follow your unit’s practice Contraindications to indometacin or ibuprofen • Renal impairment • Urine output <1 mL/kg/hr • Platelet count <50 × 109 /L • Suspected necrotising enterocolitis Dose • If not contraindicated, give loading dose of indometacin 100 microgram/kg IV over 20–30 min or ibuprofen 10 mg/kg IV administered in accordance with Neonatal Formulary SUBSEQUENT MANAGEMENT • Check renal function and platelets before each dose • Repeat echocardiogram after completing the course • Feeds can be initiated and continued at a routine rate Monitoring pharmacological treatment • Check: • urine output >1 mL/kg/day • feed tolerance • FBC platelets >50 × 109 /L • renal profile: an increase in urea and creatinine can be expected after administration of indometacin/ibuprofen but urine output is of more clinical value. Discuss with senior colleague Persistence or recurrence of murmur • Does not necessarily indicate return of PDA • Echocardiogram sometimes demonstrates a physiological left branch pulmonary stenosis: common after ductal closure and not clinically significant Surgical referral • Consider surgical ligation if: • pharmacological closure contraindicated or ineffective • obvious cardiac compromise • it is not possible to extubate baby or there has been post-extubation failure • there have been pulmonary haemorrhages or other symptoms suggestive of ductal steal DISCHARGE POLICY FOR PERSISTENT PDA • If duct does not close but baby can be extubated: • monitor duct clinically • Refer to cardiologist for further management if there is: • evidence of cardiac failure • failure to thrive • persistent oxygen requirement • If PDA still present echocardiographically or clinically by age 6 wks, refer to paediatric cardiology service
- 17. Pericardial 2011-13 PERICARDIOCENTESIS INDICATION Consider drainage of a pericardial effusion only if there is cardiovascular compromise PERICARDIAL EFFUSION Causes • Neonatal hydrops • Extravasation of TPN from migrated long lines • Complication of central venous catheters Clinical signs • Tachycardia • Poor perfusion • Soft heart sounds • Increasing cardiomegaly • Decreasing oxygen saturation • Arrhythmias • Sudden collapse in baby with long line or umbilical venous catheter (UVC) in situ Investigations • Chest X-ray: widened mediastinum and enlarged cardiac shadow • Echocardiogram (if available) EQUIPMENT • Sterile gown and gloves • Sterile drapes • Dressing pack with swabs and plastic dish • 22/24 gauge cannula • 5–10 mL syringe with 3-way tap attached • Cleaning solution as per unit policy - suggest aqueous chlorhexidine 0.5%/isopropyl alcohol 70% (Hydrex), diluted 50:50 with Normasol for infants <26 weeks’ gestation PROCEDURE Consent and preparation • If time allows, inform parents and obtain consent (verbal or written) • If skilled operator available, perform under ultrasound guidance • In an emergency situation, the most experienced person present performs procedure without delay and without ultrasound guidance • Ensure baby has adequate analgesia Drainage • Maintain strict aseptic technique throughout • Clean skin around xiphisternum and allow to dry • Attach needle to syringe and insert just below xiphisternum at 30° to skin and aiming towards left shoulder • Continuously aspirate syringe with gentle pressure as needle inserted. As needle enters pericardial space there will be a gush of blood or air • Send aspirated fluid for microbiological and biochemical analysis • Withdraw needle AFTERCARE • Cover entry site with clear dressing (e.g. Tegaderm/Opsite)
- 18. Extreme prematurity 2011-13 EXTREME PREMATURITY INTRODUCTION • Outcomes for premature babies at borderline of viability generally improve with each additional week of gestational age • estimation of gestational age confirmed by ultrasound when carried out in first trimester of pregnancy is generally reliable • Discussion with parents, before birth if possible, should precede any action MANAGEMENT • An experienced paediatrician to be present at delivery of extremely premature babies (<28 completed weeks’ gestation) and make confirmatory assessment of gestational age and condition of baby ≥24 weeks gestation • Unless baby has a severe abnormality incompatible with any significant period of survival, initiate intensive care and admit to neonatal intensive care unit <24 weeks gestation • Discuss with parents national and local statistical evidence for survival in babies with range of disabilities found in this age group • explain that statistics indicate most babies born <24 weeks’ gestation will die Between 24 weeks, 0 days and 24 weeks, 6 days’ gestation • Unless parents and clinicians agree that, in view of baby’s condition (or likely condition) it is not in his/her best interests to start intensive care, provide full, invasive, intensive care and support from birth and admit to neonatal intensive care unit Between 23 weeks, 0 days and 23 weeks, 6 days’ gestation • Give precedence to parents’ wishes regarding resuscitation and invasive intensive care treatment. However, when condition indicates baby will not survive for long, clinicians are not legally obliged to proceed with treatment that is wholly contrary to their clinical judgement, if they consider treatment would be futile • as a first step, determine whether baby is suffering, whether any suffering can be alleviated, and likely burden placed on baby by intensive care treatment • where parents would prefer clinical team to make decision about initiation of intensive care, clinicians must determine what constitutes appropriate care • where it has not been possible to discuss a baby’s treatment with mother and, where appropriate, her partner, before the birth, clinical team should consider offering full invasive intensive care until baby’s condition and treatment can be discussed with parents Between 22 weeks, 0 days and 22 weeks, 6 days gestation • Standard practice should be not to resuscitate a baby and this would normally not be considered or proposed • If parents request resuscitation, and reiterate this request, discuss risks and long-term outcomes with an experienced neonatologist before attempting resuscitation and offering intensive care • Treating clinicians must all agree that this is an exceptional case where resuscitation is in a baby’s best interests Below 22 weeks gestation • Resuscitation should never occur in routine clinical practice • any attempt to resuscitate babies born at this gestational age should take place only within the context of an approved research study When intensive care not given, clinical team must provide palliative care until baby dies
- 19. EXTREME PREMATURITY Supporting information Most babies born <24 weeks gestation are expected to die, but outcome improves with each additional week of gestational age? A retrospective, 5 year case-control review of 237 infants with gestational ages < 27 weeks (Genzel-Boroviczeny, 2010) found that, despite successful resuscitation, infants between 23 and 26 weeks had a very poor prognosis for survival when presenting with bradycardia, cyanosis and no respiratory efforts (1-min Apgar=1) at birth. Initiating active treatment for an infant at 23 weeks with bradycardia and apnoea was almost always unsuccessful (with a 1- min Apgar score of 1, a male infant at 23 weeks and 500g had a mortality rate of 92%), whereas by 26 weeks gestation, the chances of survival were higher than the probability of death. .nhs.uk Genzel-Boroviczeny O, Hempelman J, Zoppelli L, et al. Predictive value of the 1-min Apgar score for survival at 23-26 weeks gestational age. Acta Paediatr 2010;99:1790-4 Evidence Level: III Last amended January 2011 Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk
- 20. Golden hour 2011-13 GOLDEN HOUR Preterm infants <28 weeks’ gestation INTRODUCTION The care preterm babies receive within the first few hours and days of life has a significant impact on their long-term outcomes. The CESDI 27–28 study highlighted the importance of good early care for preterm babies with particular reference to effective resuscitation (see Resuscitation guideline) AIM To stabilise and perform all procedures required by the baby within the first hour of life BEFORE DELIVERY Nurses Doctors/ANNPs • Identify nurse responsible for admission and redistribute existing babies • Ensure incubator set up and pre-warmed with humidity set at maximum • Check monitor and appropriate connections • Set oxygen saturation limits at 92–95% • Ensure ventilator and NeopuffTM plugged in and checked • Ensure appropriate size face masks available • Prepare suction and catheters • Ensure transport incubator pre-warmed and cylinders full • Ensure endotracheal tube (ETT) sizes 2.5 and 3.0 are available • Set up trolley for umbilical arterial catheter (UAC) and umbilical venous catheter (UVC) beside incubator • Prepare infusion fluids for UAC and UVC • Take resuscitation bag and saturation monitor to delivery • Registrar or experienced ANNP is responsible for early care of babies <28 weeks’ gestation • counsel parents appropriate to gestation • <26 weeks, discuss delivery with consultant, who will attend whenever possible • Prescribe infusions for UAC and UVC • Check resuscitaire in delivery suite • ensure overhead heater switched on and set to maximum • set peak inspiratory pressure (PIP) at 20 cmH2O and FiO2 at 0.21 • check saturation monitor and probe available • Prepare plastic bag
- 21. Golden hour 2011-13 AFTER DELIVERY Nurses Doctors/ANNPs • Keep baby warm with plastic bag and hat • Assist with resuscitation • Accurate time-keeping including resuscitation and procedures • Attach oxygen saturation probe to right hand • Assist with ETT fixation • Set up transport incubator and transfer baby to it • Ensure baby labels in place before transport • Ensure midwives have taken cord gases • Transfer baby to neonatal unit (NNU) • Competent practitioner, ANNP or middle grade doctor to attend • If normal delivery and baby breathing, delay clamping of cord for 1–2 min providing baby can be kept warm • If operative or instrumental delivery, cut cord immediately and take baby to resuscitaire • Place baby in plastic bag • Cover baby’s head with appropriate size warmed hat • Assess colour tone, heart rate and breathing • If baby is breathing regularly, commence CPAP at 5 cmH2O • If baby is not breathing regularly, give 5 inflation breaths at 20–25 cmH20 using T piece and face mask • monitor response by checking colour, breathing and heart rate • if baby does not start to breath, ventilate at 20/5 • if heart rate not above 100 bpm or falls, observe chest movement and if poor, increase pressures to 25/5 • observe chest movement throughout and, if obvious and heart rate good, reduce pressures • when heart rate >100 bpm or chest movement seen, check saturation monitor and adjust FiO2 aiming to bring saturations close to NLS guidance • If continued IPPV necessary, intubate • If unit policy is to give surfactant on labour ward ensure that ETT is not inserted too far and is securely fixed before administering surfactant • Check baby once placed in transport incubator and review • air entry • colour • heart rate • saturation • Complete joint resuscitation record and obtain signature from maternity team • Show baby to parents • Senior member of staff to talk briefly to parents • Transfer baby to NNU
- 22. Golden hour 2011-13 FIRST HOUR ON NNU Nurses Doctors/ANNPs • Aim for at least 1:1 nursing care for first hour • Transfer to incubator in plastic bag • Weigh baby in plastic bag • Leave baby in plastic bag until incubator reaches adequate humidity • Attach baby to ventilator or CPAP driver and reassess ABC • If ventilated, pre-warm surfactant and prepare Mac TachCare • Monitor heart rate and saturation • Record blood pressure • Do not use ECG leads on babies <26 weeks’ gestation • Measure axillary temperature on arrival • Insert nasogastric (NG) tube • Assist doctor/ANNP with lines • Give Vitamin K • Give first dose of antibiotics • Take a photograph for parents • Reassess ABC • Split tasks between doctors/ANNP Doctor/ANNP A • Prescribe weight dependent drugs and infusions and Vitamin K • Write blood test forms and prepare blood bottles • Start admission notes (Badger) Doctor/ANNP B • Check ETT position clinically and administer surfactant if not previously given on labour ward • Check ventilation – Review tidal volume and chest movement • if tidal volume >5 mL/kg or vigorous chest movement, reduce PIP without waiting for first gas • check saturations and adjust FiO2 to keep saturation 92–95% • Insert UAC and UVC through hole in plastic bag • commence infusions as soon as line secured • Take blood for: • FBC • clotting • group and DCT • blood culture • blood glucose • pre-transfusion bloodspots • arterial gas • Defer peripheral IV cannula insertion unless unable to get umbilical lines • Once lines inserted, request X-rays • Document • ETT position • NG length • UAC and UVC positions at time X-ray taken • Write X-ray report in notes • Update parents and document in notes Once baby set up – minimise handling Hands off – Eyes on
- 23. Hypothermia 2011-13 HYPOTHERMIA DEFINITION • Skin temperature <36.0O C on admission from delivery suite ASSESSMENT Babies at risk • Preterm <30 weeks’ gestation • Low birth weight <1500 g • Sick baby • Small for dates Consequences (<36.0O C) • Hypoglycaemia • Metabolic acidosis • Hypoxia with increased oxygen demands Consequences (<35.5O C) • Increased metabolic rate • Clotting disorders • Shock • Apnoea • Intraventricular haemorrhage • Persistent fetal circulation • Decreased surfactant production and function Causes of heat loss • Radiation: heat lost to cooler objects in the room • in cold environment, whether in incubator or not, excessive heat may be lost • in excessively hot environment or in direct sunlight, baby could overheat in incubator • Conduction: heat lost to cooler surfaces on which baby is placed • Convection: heat lost due to drafts • Evaporation: heat lost through water evaporating from skin PREVENTION Delivery suite • Keep room 23–28O C and free from draughts, especially when babies are due to be delivered Babies <30 weeks • Dry head and put on hat • Do not dry remainder of baby • Place in polythene bag immediately and keep inside bag until placed in pre-heated pre- humidified incubator. Do not cover the polythene bag during transfer Other babies • Use pre-warmed towel, dry immediately after delivery • Discard towel and wrap in another pre-warmed towel and blanket • Ensure room warm enough to enable skin-to-skin contact and early breastfeeding • Cover exposed skin with warm blanket Neonatal unit • Keep at 24–25O C to avoid cooling from radiant heat loss, and ‛misting’ (condensation) in incubators • Keep incubators and cots away from windows to prevent radiation heat loss • Nurse babies requiring intensive care in pre-warmed incubator
- 24. Hypothermia 2011-13 • Babies <29 weeks must have humidification >60% for first 2 weeks Incubator temperature during first 3 days Birth weight (g) Incubator temperature (O C) 1000 35 1500 34 2000 33.5 2500 33.2 3000 33 4000 32.5 • Babies <1000 g require even higher temperatures, occasionally >37O C • If baby’s temperature remains within normal limits for 24 hrs, reduce incubator temperature by 1O C according to baby’s needs • When baby’s weight reaches about 1600 g, or according to local practice, transfer to open cot Rainout may occur if the difference between temperature in incubator and room temperature is >5O C: ensure room temperature kept at locally agreed level Babies not at risk of hypothermia • If not requiring observation of respiratory status or excessive invasive procedures, babies may be: • dressed • kept wrapped • placed in a cot • Mild hypothermia can be managed with the addition of: • hats • cot lids • heated mattresses • If baby’s temperature <36.0O C consider: • use of incubator, if available • increasing humidity, if appropriate for gestational age • bubble wrap REWARMING OF HYPOTHERMIC BABIES • Rewarm in incubator • >1200 g, rewarm at 1O C per hour • <1200 g, rewarm more slowly Take care not to overheat babies. Aim for 36.5–37.2O C
- 25. HYPOTHERMIA Supporting Information Placing the baby in a polythene bag prevents heat loss pending transfer to an incubator? A Cochrane systematic review (McCall, 2010) found that “Plastic wraps or bags were effective in reducing heat losses in infants < 28 weeks' gestation (4 studies, n = 223; WMD 0.68 °C; 95% CI 0.45, 0.91), but not in infants between 28 to 31 week's gestation.” McCall EM, Alderdice F, Halliday HL, et al. Interventions to prevent hypothermia at birth in preterm and/or low birthweight infants. Cochrane Database of Systematic Reviews 2010, Issue 3. Art. No.: CD004210 Evidence Level: I Heated mattresses are useful in the treatment of mild hypothermia? A retrospective review (Ibrahim, 2010) studied the occurrence of hypothermia in 105 babies born before, and 124 born after the introduction of heated gel mattresses. Four (3.3%) babies were hypothermic (temperature <36 degrees C) at admission when the mattresses were used, compared to 21 (22.6%) babies during the period it was not (p < 0.001). Hyperthermia (temperature >37 degrees C) rose from 30.1% prior to use of gel mattresses to 49.6% when they were used (p = 0.004). Ibrahim CP, Yoxall CW. Use of self-heating gel mattresses eliminates admission hypothermia in infants born below 28 weeks gestation. Eur J Pediatr 2010;169:795-9 Evidence Level: IV Last amended October 2010 Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk
- 26. Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk PAIN AND STRESS Supporting information This guideline and supporting information has been prepared with reference to: Anon. Prevention and management of pain in the neonate: an update. American Academy of Pediatrics Committee on Fetus and Newborn and Section on Surgery; Canadian Paediatric Society Fetus and Newborn Committee. Pediatrics 2006;118:2231-41 What is the evidence for the efficacy of non-pharmacological interventions? A systematic literature review of 13 randomised trials and 2 meta-analyses (Cignacco, 2007) looked at the effects of non-nutritive sucking, music, swaddling, positioning, olfactory and multisensorial stimulation, kangaroo care and maternal touch. These had an observable positive effect on pulse rate, respiration and oxygen saturation, reduction of motor activity and excitation states following painful procedures. Validated pain assessment instruments were not employed in these studies, however, and further research was called for. A Cochrane systematic review of 11 trials (Shah, 2006) found that distress measured by heart rate, crying time and three scoring systems (Premature Infant Pain Profile, Douleur Aigue Nouveau-ne and Neonatal Facial Coding Score) was significantly reduced by breastfeeding or breast milk supplementation during painful procedures. A double-blind prospective trial in 110 infants (Thyr, 2007) found that infants given 2 mL of 30% glucose after immunisation at 3, 5 and 12 months cried less than those given water (mean crying time reduced by 22, 62 and 52% respectively). “Additional research is needed to fully understand the mechanism of action, optimal dose, and safety of repeated doses of oral sucrose in neonates” (Anon, 2006). A meta-analysis of 20 RCTs involving 1380 infants and children between 1 month and 11 years of age (Chambers, 2009) found that breathing exercises, child-directed distraction, nurse-led distraction, and combined cognitive-behavioural interventions were effective in reducing the pain and distress associated with routine childhood immunisations. A Cochrane systematic review of 44 studies involving 3,496 infants (Stevens, 2010) found that sucrose significantly reduced the duration of total crying time (seconds) [WMD -39.26 (95% CI - 44.29, -34.24), 88 neonates]. Anon. Prevention and management of pain in the neonate: an update. American Academy of Pediatrics Committee on Fetus and Newborn and Section on Surgery; Canadian Paediatric Society Fetus and Newborn Committee. Pediatrics 2006;118:2231-41 Chambers CT, Taddio A, Uman LS, et al. Psychological interventions for reducing pain and distress during routine childhood immunizations: a systematic review. Clin Ther 2009;31(Suppl 2):S77-S103) Cignacco E, Hamers JP, Stoffel L, et al. The efficacy of non-pharmacological interventions in the management of procedural pain in preterm and term neonates. A systematic literature review. Eur J Pain 2007;11:139-52 Shah PS, Aliwalas LL, Shah V. Breastfeeding or breast milk for procedural pain in neonates. Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No.: CD004950 Stevens B, Yamada J, Ohlsson A. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database of Systematic Reviews 2010, Issue 1. Art. No.: CD001069 Thyr M, Sundholm A, Teeland L, et al. Oral glucose as an analgesic to reduce infant distress following immunization at the age of 3, 5 and 12 months. Acta Paediatr 2007; 96:233-6 Evidence Level: I Last amended May 2010
- 27. Pain and Stress 2011-13 PAIN AND STRESS RECOGNITION AND ASSESSMENT Symptoms and signs • Distinguish signs of pain and stress from signs of life-threatening conditions, such as hypoxia, seizures or CO2 retention, which require other forms of management • Lack of behavioural responses (e.g. crying and movement) does not necessarily indicate lack of pain Sudden pain and distress is usually caused by serious condition e.g. bowel perforation Behavioural • Crying, whimpering • Facial expressions: • brow bulge • eye squeeze • deepening of nasolabial folds • Active movement and attempts to withdraw from painful stimulus: • thrashing • tremulousness • limb withdrawal, flexion • cycling movements • arching • Flexor reflexes; leg withdrawal • Exaggerated reactivity • Decreased sleep periods Physiological • Changes in heart rate and variability • Respiratory rate and quality, including apnoea and tachypnoea • Fluctuations in blood pressure, up or down • Decreased transcutaneous oxygen and carbon dioxide levels • Oxygen desaturation • Pallor • Flushing Indications for pain management • Before painful procedures: • insertion of long lines • intubation and IPPV • lumbar puncture • insertion of chest drain • venous sampling/access • In response to behavioural changes • To aid ventilation in: • term infants with pulmonary hypertension • stabilisation of congenital diaphragmatic hernia • preterm babies only if local unit policy • To assist with management of cooling in infants treated for encephalopathy NON-PHARMACOLOGICAL PAIN MANAGEMENT • Non-nutritive sucking • Swaddling • Calming • Tactile stimulation
- 28. Pain and Stress 2011-13 • Rocking • Expressed breast milk • Skin-to-skin care PRINCIPLES OF ANALGESIA • Prophylactic or symptomatic • Use stepwise approach with agents of increasing potency ANALGESIA FOR NON-VENTILATED INFANTS Sucrose Activates opioid systems that provide natural analgesia and is recognised as an appropriate analgesia for newborn babies during some painful procedures Contraindicated in unstable babies, sedated intubated babies, NEC, GI obstruction and paralysed babies Indications • Heel pricks for blood sampling • Cannulation and venous sampling • Ventricular tap • Lumbar puncture • Insertion of long lines • Eye examination • IM injection • Tape removal • Nasogastric tube insertion Use • Use sucrose in conjunction with other non-pharmacological methods such as: • dummy • hands-on comforting • swaddling • performing procedure in a quiet environment • Use sucrose solution (e.g. Sweet-Ease 24%) • preterm baby: 0.1–0.5 mL repeated as necessary • term baby: 2 mL in repeated doses as necessary at 5 min intervals to a maximum of 3 doses per procedure • maximum doses per 24 hr – see Table 1 Table 1: Maximum doses of sucrose per 24 hr Gestational age (weeks) Maximum oral dose of sucrose (24%) 24–26 0.2 mL (max 1 mL in 24 hr) 27–31 0.5 mL (max 2.5 mL in 24 hr) 32–36 1 mL (max 5 mL in 24 hr) >36 weeks 2 mL (max 10 mL in 24 hr) Give a maximum of 5 doses only in one 24 hr period • Give first dose 2 min before procedure by one of the following methods: • dip cotton bud into solution and wipe around baby’s mouth • dip dummy into solution and give to baby (each dip is 0.2 mL) • via syringe Topical pain relief • Lidocaine (plain, not with adrenaline) 1% 0.3 mL/kg maximum per dose effective as a topical anaesthesia
- 29. Pain and Stress 2011-13 Indications • Insertion of a chest drain • Insertion of a peritoneal drain Paracetamol • Orally or rectally: absorbed more quickly if given via oral route Table 2 Route Gestation Loading dose Maintenance Maximum daily dose Oral >32 weeks 24 mg/kg 12 mg/kg 4-hrly 60 mg/kg <32 weeks 24 mg/kg 12 mg/kg 8-hrly 30 mg/kg Rectal >32 weeks 30 mg/kg 20 mg/kg 8-hrly 60 mg/kg <32 weeks 20 mg/kg 15 mg/kg 12-hrly 30 mg/kg Morphine sulphate oral liquid (Oramorph) • Particularly useful for chronic pain relief and for terminal care • Large doses such as 100 microgram/kg 6-hrly can cause hypotension and respiratory depression ANALGESIA FOR VENTILATED INFANTS • It is essential that ventilated babies have adequate pain control • may be achieved using diamorphine or morphine in addition to agents used for non- ventilated Infants • Manage any asynchrony using alternative ventilation modes (see Ventilation guideline) • Loading doses for maintenance of analgesia for ventilation are lower than formulary recommends for painful procedures Diamorphine • Loading dose for ventilated babies in serious pain, 180 microgram/kg IV over 30 min • Maintenance 15 microgram/kg/hr IV infusion • Larger doses than this are no more effective but are associated with more adverse effects • Effects can be reversed by naloxone 100 microgram/kg IV Morphine • Loading dose for sedation whilst ventilated 120 microgram/kg IV over 5 min; for severe pain 240 microgram/kg • Maintenance 10–20 microgram/kg/hr IV • Can cause hypotension, bradycardia and respiratory depression • Half-life between 1 and 6 hr: increases with decreasing gestational age • Effects can be reversed by naloxone 100 microgram/kg IV as a bolus SEDATION Sedation has no analgesic effect. Always use in conjunction with appropriate analgesia Chloral hydrate • Can be useful in irritable fatigued child/cerebral irritation • Has long half life and can accumulate, leading to hypotension and respiratory depression • single dose treatment: 45 mg/kg orally (75 mg/kg for term infants for single procedure, e.g. CT) • sustained sedation: 30 mg/kg 6-hrly orally • if used regularly, review after 1–2 days Avoid EMLA cream: evidence of efficacy in neonate is inconsistent
- 30. PRETERM CARE (“GOLDEN HOUR”) Supporting information Evidence pertinent to this guideline may be found in the supporting information for the following Neonatal Guidelines: • Resuscitation • Hypothermia • Ventilation • Cannulation • Infection Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk
- 31. Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk RESUSCITATION Supporting information This guideline and supporting information has been prepared with reference to the following: Anon. Ethical guidelines on resuscitation of newborns: FIGO Committee for the Ethical Aspects of Human Reproduction and Women’s Health. Int J Gynecol Obstet 2006;94:169-71 Kattwinkel J, Perlman JM, Aziz K, et al. Neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Pediatrics 2010;126:e1400-13 Resuscitation Council (UK). Newborn life support. 2010 http://www.resus.org.uk/pages/nls.pdf Naloxone should not be administered to infants whose mothers abuse narcotics? A single case study (Gibbs, 1989) recorded generalised convulsions unresponsive to diazepam in a naloxone-treated baby born to a heroin user maintained throughout her pregnancy on methadone. The authors concluded that, as convulsions due to neonatal abstinence syndrome do not appear until at least 48 hours after birth, the symptoms in this case were due to naloxone administration. Gibbs J, Newson T, Williams J, et al. Naloxone hazard in infant of opioid abuser. Lancet. 1989;2:159–60 Evidence Level: V Should resuscitation be carried out with 21% or 100% oxygen? Guidelines from the Resuscitation Council (see above) give no direction on this question. A systematic review and meta-analysis of 10 studies in a total of 2,133 infants (Saugstad, 2008) found that those given 21% oxygen (n=1,082) had reduced mortality compared to those (n=1,051) given 100% oxygen (RR 0.69; 95% CI 0.54 – 0.88). A systematic review of 2,011 infants from 7 controlled trials (Rabi, 2007) found a statistically significant reduction in mortality in the room air group at 1 week (OR 0.70, 95% CI 0.50 - 0.98) and at 1 month (OR 0.63, 95% CI 0.42 - 0.94). A randomised study in 44 preterm infants (Ezaki, 2009) found reduced oxidative stress in the group given 21% oxygen, compared to the group given 100% oxygen. Ezaki S, Suzuki K, Kurishima C, et al. Resuscitation of preterm infants with reduced oxygen results in less oxidative stress than resuscitation with 100% oxygen. J Clin Biochem Nutr 2009;44:111-8 Rabi Y, Rabi D, Yee W. Room air resuscitation of the depressed newborn: a systematic review and metaanalysis. Resuscitation 2007;72:353–63 Saugstad OD, Ramji S, Soll RF, et al. Resuscitation of newborn infants with 21% or 100% oxygen: an updated systematic review and meta-analysis. Neonatology 2008;94:176-82 Evidence Level: I Last amended September 2011
- 32. Resuscitation 2011-13 RESUSCITATION • Check equipment daily, and before resuscitation • Follow Resuscitation Council UK Guidelines www.resus.org.uk DRY AND COVER • Cord clamping – see Cord clamping below • >28 weeks’ gestation, dry baby, remove wet towels and cover baby with dry towels • <28 weeks’ gestation, do not dry body but place in plastic bag, dry head only and put on hat Cord clamping • It is current NLS recommendation that cord is not clamped immediately • In uncompromised infants a delay in cord clamping of at least one minute is recommended • After discussion in Staffordshire, Shropshire & Black Country resuscitation group it has been decided any time a neonatologist is called for fetal reasons, do not delay cord clamping ASSESS • Assess colour, tone, breathing and heart rate If baby very floppy and heart rate slow, assist breathing immediately • Reassess every 30 sec throughout resuscitation process • If help required, request immediately If baby not breathing adequately by 90 sec, assist breathing CHECK AIRWAY For baby to breathe effectively, airway must be open • To open airway, place baby supine with head in ‛neutral position’ • If very floppy, consider chin support or jaw thrust while maintaining the neutral position IMMEDIATE TREATMENT Airway • Keep head in neutral position • Use T-piece and soft round face mask, extending from nasal bridge to chin • Give 5 inflation breaths, sustaining inflation pressure (Table 1) for 2–3 sec for each breath • Give PEEP of 5 cm H2O • Begin inflation breaths in air Table 1: Inflation pressure (avoid using pressure higher than recommended) Term infant 30 cm of water Preterm infant 20–25 cm of water No chest movement Ask yourself: • Is head in neutral position? • Is a jaw thrust required? • Do you need a second person to help with airway to perform a jaw thrust?
- 33. Resuscitation 2011-13 • Is there an obstruction and do you need to look with a laryngoscope and suck with a large- bore device? • Consider placing oro-pharyngeal (Guedel) airway under direct vision using laryngoscope • Is inflation time long enough? • if no chest movement occurs after alternative airway procedures above have been tried (volume given is a function of time and pressure), a larger volume can be delivered if necessary by inflating for a longer time (3–4 sec) • Attach saturation monitor to right hand – see Saturation monitoring for guidance on saturation targets Endotracheal intubation Indications • Severe hypoxia (e.g. terminal apnoea or fresh stillbirth) • Stabilisation of airway • Extreme prematurity • Congenital diaphragmatic hernia Breathing • Most babies have a good heart rate after birth and establish breathing by 90 sec • if not breathing adequately give 5 inflation breaths, preferably using air at pressures in Table 1 • heart rate should rapidly increase as oxygenated blood reaches heart Do not move onto ventilation breaths unless you have a heart rate response OR you have seen chest movement Review assessment after inflation breaths • Is there a rise in heart rate? • Is there chest movement with the breaths you are giving? • If no spontaneous breathing, but chest movement has been obtained, perform 30 sec of ventilation breaths, given at a rate of 30 breaths per min (1 sec inspiration) Table 2: Outcome after 30 sec of ventilation breaths Heart rate Breathing Action Increases Not started breathing • Provide 30–40 breaths/min • Where available, use PEEP at 5 cm water with T-piece system <60 Obvious chest movement • Start chest compressions – See below • If baby is floppy with slow heart rate and there is chest movement, start cardiac compressions with ventilation breaths immediately after inflation breaths • Increase inspired oxygen concentration every 30 sec by 30% e.g. 30–60–90% depending on response – see Saturation chart Safe insertion of tracheal tube requires skill and experience If you cannot insert a tracheal tube within 30 sec, revert to mask ventilation
- 34. Resuscitation 2011-13 Chest compression • Use if heart rate approximately <60 beats/min (do not try and count accurately as this will waste time) Figure 1 Figure 2 Pictures taken from NLS manual and Resuscitation Council (UK) and reproduced with their permission Ideal hold (figure1/figure 2) • Circle chest with both hands so that thumbs of both hands can press on the sternum just below an imaginary line joining the nipples with fingers over baby’s spine Alternative hold (less effective) • Compress lower sternum with fingers whilst supporting baby’s back. The alternative hand position for cardiac compressions can be used when access to the umbilicus for UVC catheterisation is required, as hands around the chest may be awkward Start chest compression only after successful inflation of lungs
- 35. Resuscitation 2011-13 Action • Compress chest quickly and firmly to reduce the antero-posterior diameter of the chest by about one-third, followed by full re-expansion to allow ventricles to refill • remember to relax grip during IPPV, and feel for chest movement during ventilation breaths, as it is easy to lose neutral position when cardiac compressions are started Co-ordinate compression and ventilation to avoid competition. Aim for 3:1 ratio of compressions to ventilations, and 90 compressions and 30 breaths (120 ‛events’) per min Blood • If there is evidence of fetal haemorrhage, consider giving O negative emergency blood Resuscitation drugs • Always ask about drugs taken recently by, or given to mother • Consider drugs only if there is an undetectable or slow heartbeat despite effective lung inflation and effective chest compression • Umbilical venous catheter (UVC) preferred venous access Adrenaline 1:10,000 • 10 microgram/kg (0.1 mL/kg) IV • If this dose is not effective, consider giving 30 microgram/kg (0.3 mL/kg) after sodium bicarbonate has been given • Adrenaline should only be given via the ET tube if venous access is taking time to achieve; it should not delay intravenous access and treatment; the dose is 0.5–1.0 mL/kg of 1 in 10,000. Sodium bicarbonate 4.2% • 1–2 mmol/kg (2–4 mL/kg) IV (never give via ET tube) Glucose 10% • 2.5 mL/kg IV slowly over 5 min Sodium chloride 0.9% • 10 mL/kg IV Naloxone • Consider only after ventilation by mask or endotracheal tube has been established with chest movement seen and heart beat >100 beats/min • If mother has been given pethidine within 2–4 hr of delivery, give IM naloxone: • 100 microgram (0.25 mL) for small prem babies • 200 microgram (0.5 mL) for all other babies Do not give naloxone to babies born to mothers who abuse narcotics WHEN TO STOP • If no sign of life present after 10 min of continuous good quality resuscitation, outlook is poor with few survivors, majority will have cerebral palsy and learning difficulties • If no sustained spontaneous breathing 30 min after a heart rate has been established, majority also have poor prognosis Continue resuscitation until a senior neonatologist advises stopping
- 36. Resuscitation 2011-13 MONITORING Saturation monitoring • Oxygen monitoring is activated when paediatrician/2nd pair of hands arrives. In the meantime, the person initiating resuscitation carries out all the usual steps in resuscitation • Do not stop resuscitation for a saturation probe to be attached • Attach saturation monitor to the right hand once five inflation breaths have been given • Saturations should spontaneously improve as Table 3 Table 3 Time (min) Acceptable pre-ductal saturations (%) 2 60 3 70 4 80 5 85 10 90 Air to oxygen • If inflation breaths have been successful and chest movement seen but heart rate and/or colour/saturations (if available) not improved: • in term babies – increase oxygen to 30% • in preterm babies – increase oxygen to 30% • If no response, increase by increments of 30% every 30 sec i.e.: Term air 30–60–90/100% Preterm air 30– 60–90/100% • Reduce oxygen if saturation levels as per Boost recommendations when oxygen saturation levels at 91–95% for preterm <30 weeks or >95% for term at 10 min of life (otherwise Resus Council target sats should be followed to stop babies being too pink too early on and being at risk of O2 toxicity) Preterm deliveries • >26 weeks’ gestation do not require routine intubation if respiratory effort good • these babies can receive PEEP 5cm H20 via mask ventilation with oxygen supplementation as appropriate on the resuscitaire and PEEP support on transfer to NICU • If respiratory effort is poor, at any point, or baby’s condition deteriorates, intubate and ventilate as per BAPM guidance DOCUMENTATION • Make accurate written record of facts (not opinions) as soon as possible after the event • Record • when you were called, by whom and why • condition of baby on arrival • what you did and when you did it • timing and detail of any response by baby • date and time of writing your entry • a legible signature COMMUNICATION • Inform parents what has happened (the facts)
- 37. Resuscitation 2011-13 Newborn life support algorithm Dry baby Remove wet towels and cover Start clock or note time Assess tone, breathing and heart rate If gasping or not breathing Open airway Give 5 inflation breaths Consider SpO2 monitoring Re-assess If no increase in heart rate, look for chest movement If chest not moving Re-check head position Consider 2-person airway control and other airway manoeuvres Repeat inflation breaths Consider SpO2 monitoring Look for a response No increase in heart rate – Look for chest movement When chest moving If heart rate not detectable or slow (<60/min), start chest compressions 3 compressions to each breath Re-assess heart rate Every 30 sec If heart rate not detectable or slow (<60/min), consider venous access and drugs Birth 60 sec 30 sec AT ALL STAGES ASK: DO YOU NEED HELP? Acceptable Pre-ductal SpO2 2 min 60% 3 min 70% 4 min 80% 5 min 85% 10 min 90%
- 38. Hyperglycaemia including insulin 2011-13 HYPERGLYCAEMIA DEFINITION • Blood glucose >12 mmol/L, and/or presence of >2+ glycosuria on dipstick testing Do not take sample from an infusion line that has glucose running through it CLINICAL FEATURES • Dehydration • Acidosis • ketoacidosis does not occur in babies • Poor weight gain Babies at high risk • Ill, unstable • Preterm (especially <28 weeks) • Small for gestational age (<3rd centile) • Receiving total parenteral nutrition (TPN) • Receiving corticosteroids, caffeine MONITORING Twice-daily monitoring • Check blood glucose at least twice a day in: • unstable or acutely ill babies (RDS, septicaemia, NEC) Daily monitoring • Check blood glucose at least once a day in babies: • <32 weeks’ gestation for first week • receiving TPN • with severe unexpected dehydration or metabolic acidosis • with poor weight gain while receiving >120 kcal/kg/day Babies treated with corticosteroids • Check urine for glycosuria daily • Check blood glucose if >2+ glucose in urine TREATMENT • Discontinue or decrease medications that worsen hyperglycaemia Suspected infection • Hyperglycaemia in baby with previously stable blood glucose may be early indicator of infection • After taking appropriate cultures, treat empirically Fluids • Correct dehydration by increasing daily fluid intake: use sodium chloride 0.9% • If baby receiving >6 mg glucose/kg/min, decrease concentration of glucose infused or replace some of the glucose intake with sodium chloride 0.9% using following formula: • glucose infusion rate (mg/kg/min) = % glucose × fluid volume (mL/kg/day) divided by 144 • these measures often bring blood glucose down substantially • hypoglycaemia can occur following overzealous glucose restriction Insulin • Consider if: • baby remains hyperglycaemic (blood glucose >12 mmol/L), and/or • presence of >2+ glycosuria on dipstick testing and • when control not obtained with above methods or • a higher carbohydrate intake than infant will tolerate is necessary for nutritional reasons
- 39. Hyperglycaemia including insulin 2011-13 • Seek senior advice about commencing insulin therapy • See Administration of Actrapid insulin below • Follow Neonatal Formulary for insulin infusion rates • Check blood glucose concentrations regularly during insulin infusion. Treating clinician to decide on frequency, based on stability of glycaemia • If unable to wean off insulin after 2 weeks, transient neonatal diabetes is likely; consult a paediatric endocrinologist ADMINISTRATION OF ACTRAPID INSULIN (SOLUBLE INSULIN) • To avoid delay in administration of Actrapid insulin infusion caused by lumen capacity of IV extension sets and cannula T-connections, administer via a peripheral cannula used only for this purpose • Before starting infusion, prime T-connector of cannula with a 0.5 mL bolus of infusion fluid • Provided an octopus or IV extension set is not used, the infusion can also be administered directly connected to the lumen of an umbilical venous catheter (UVC). In this instance, the recommended priming volume is 0.26 mL • If it is not possible to deliver the Actrapid infusion in either of these ways, and the use of an extension set or octopus is unavoidable, be aware of lumen capacity of the extension set used and the delay it may cause. Inform medical team when assessing effectiveness of treatment • Calculate delays by using the information below and the infusion rate Example Actrapid insulin to be infused at 0.1 mL/hr through a peripheral cannula (including a ‘T’ adapter) + octopus extension set Total lumen capacity: 0.5 mL + 0.34 mL = 0.84 mL Time delay: 0.84 mL/0.1 mL/hr = 8.4 hr* Lumen capacity of IV sets** IV product Product manufacturer Product code Priming volume (lumen capacity) Extension set with ‘T’ adapter SL Venisytems F89805014 0.5 mL Ready set Vygon 836.201 0.85 mL Double lumen umbilical catheter Vygon 1274.14 0.26 mL Triple lumen extension tube with Bionector (octopus) Vygon 841.364 0.34 mL (per lumen) *It may be possible to reduce delay by priming some or all of the IV assembly with infusion fluid, if safe from interactions with drugs infused simultaneously through same extension set and with permission of the medical team i.e. SpR or consultant only **Information above was obtained from the manufacturers of the IV sets currently in use. If a new product is introduced or a new manufacturer used for an existing product, priming volume may require updating
- 40. Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk HYPERGLYCAEMIA Supporting information Hyperglycaemia increases mortality risk in premature infants? A prospective chart study of 93 extremely low birth-weight infants (Hays, 2006) found that more than 50% of the infants had persistent blood glucose concentrations of >150 mg/dL during the first week of life. Twenty-two of these infants (44%) had an early adverse outcome, defined as death or intra-ventricular haemorrhage of grade 3 or 4 before the 10th day of life. Another prospective study in 252 premature infants weighing </=1500 g (Heimann, 2007) found a significant increase in mortality (p<0.0001) with increasing median blood glucose level and repeated (>/=4) incidents of blood glucose levels >/=150 mg/dL associated with low gestational age (<27 weeks). Retrospective analysis of a prospective cohort study of 201 ELBW infants (Kao, 2006) found the odds ratio for either dying or developing a late infection was 5.07 (95% CI 1.06 – 24.3) in those babies with persistent severe hyperglycaemia (>/=180 mg/dL). A review of the literature (Ogilvy-Stuart, 2010) concluded that hyperglycaemia “is associated with increased morbidity and mortality in preterm infants, but what should be considered optimal glucose control, and how best to achieve it, has yet to be defined in these infants”. Hays SP, O’Brian Smith E, Sunehag AL. Hyperglycemia is a risk factor for early death and morbidity in extremely low birth-weight infants. Pediatrics 2006;118:1811-18 Heimann K, Peschgens T, Kwiecien R, et al. Are recurrent hyperglycemic episodes and median blood glucose level a prognostic factor for increased morbidity and mortality in premature infants </=1500 g? J Perinat Med 2007;35:245-8 Kao LS, Morris BH, Lally KP, et al. Hyperglycemia and morbidity and mortality in extremely low birth weight infants. J Perinatol 2006;26:730-6 Ogilvy-Stuart AL, Beardsall K. Management of hyperglycaemia in the preterm infant. Arch Dis Child Fetal Neonat Ed 2010;95:F126-31 Evidence Level: IV Treating hyperglycaemia has a beneficial effect on mortality and morbidity? A Cochrane Systematic Review of 2 trials in 47 infants (Bottino, 2009) found the evidence was insufficient to answer this question and called for more and larger trials to be conducted. Bottino M, Cowett RM, Sinclair JC. Interventions for treatment of neonatal hyperglycemia in very low birth weight infants. Cochrane Database of Systematic Reviews 2009, Issue 1. Art. No.: CD007453 Evidence Level: I Last amended June 2010
- 41. Hyperkalaemia 2011-13 HYPERKALAEMIA RECOGNITION AND ASSESSMENT • Plasma potassium >6 mmol/L (normal 3.0–5.5 lithium heparin specimen) • Neonates often tolerate concentrations up to 7.5–8.0 mmol/L without ECG changes SYMPTOMS AND SIGNS • Cardiac arrest • ECG abnormalities (see below): • tall peaked T waves • widened QRS complex • sine waves (widened QRS complex merging with T wave) • prolonged PR interval, bradycardia, absent P wave Tall, peaked T wave, widening of QRS Sine wave QRS complex (before cardiac arrest) CAUSES • Renal failure: secondary to hypoxic ischaemic encephalopathy (HIE), sepsis and hypotension, or structural abnormalities • Cellular injury with potassium release e.g. large intraventricular haemorrhage • Very low-birth-weight babies without renal failure (non-oliguric hyperkalaemia) in first 12– 48 hr • Excess K + in IV solutions • Endocrine (congenital adrenal hyperplasia) INVESTIGATIONS • If sample haemolysed, repeat and send free-flowing venous sample or arterial sample • If potassium >6.0 mmol/L, connect to cardiac monitor IMMEDIATE TREATMENT Serum potassium >6.0 mmol/L (stable with normal ECG) • Stop all K + IV solutions or oral supplements • Reconfirm hyperkalaemia • Institute continuous ECG monitoring
- 42. Hyperkalaemia 2011-13 Serum potassium >7.0 mmol/L without ECG changes • As above • Give salbutamol 4 microgram/kg IV in glucose 10% over 5–10 min: effect evident within 30 min but sustained benefit may require a repeat infusion after at least 2 hr • if IV access difficult, give nebulized salbutamol 2.5 mg as a single dose (difficult to administer if ventilated and not formally evaluated in neonates) and repeat if necessary • Give intravenous insulin 0.5 units/kg in glucose 10% (made up to 2.5 mL and given over 30 min): very effective and has an additive effect with salbutamol • Repeat U&E • Repeat insulin infusion as necessary until K + <7 mmol/L • Monitor blood glucose every 15 min for first 2 hr during and after infusion • aim for blood glucose 4–7 mmol/L Serum potassium >7.5 mmol/L with ECG changes • As above, but first institute emergency measures below: • give 10% calcium gluconate 2 mL/kg IV over 5–10 min • flush line with sodium chloride 0.9% or preferably use a different line • give IV sodium bicarbonate (1 mmol/kg over 2 min) this is effective even in patients who are not acidotic (2 mL of 4.2 % sodium bicarbonate = 1 mmol) Further treatments: discuss with consultant • A cation-exchange resin, such as calcium resonium (500 mg/kg rectally, with removal by colonic irrigation 8–12 hrly, repeat every 12 hr. Dose can be doubled at least once to 1 g/kg in severe hyperkalaemia). Useful for sustained reduction in serum potassium but takes many hours to act and is best avoided in sick preterms who are at risk of necrotising enterocolitis (NEC) • If severe hyperkalaemia persists despite above measures in term babies with otherwise good prognosis, contact renal team for consideration of dialysis • Exchange transfusion using fresh blood or washed red blood cells provides another strategy for sustained and reliable reduction in serum K + concentration – see Exchange transfusion guideline SUBSEQUENT MANAGEMENT • Recheck serum K + 4–6 hrly; when arrhythmias present with renal failure, monitor hourly • Monitor urine output and maintain good fluid balance • If urine output <1 mL/kg/hr, unless baby volume depleted, give IV furosemide 1 mg/kg until volume corrected • Treat any underlying cause (e.g. renal failure)
- 43. Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk HYPERKALAEMIA Supporting information What is the evidence for the use of salbutamol, and is it superior to insulin as a treatment for hyperkalaemia? Has nebulised salbutamol been evaluated? Intravenous administration of insulin (together with glucose) effectively manages hyperkalaemia in neonates (Ditzenberger, 1999), but the response is unpredictable, and carries the risk of hypoglycaemia, hyperosmolarity, and volume overload (Helfrich, 2001). No good, randomised trials for its use in neonates have been identified. Intravenous salbutamol is rapidly effective and side effects, including elevated heart rate, mild vasomotor flushing and mild tremor are all short-lasting (Helfrich, 2001; Kemper, 1996; Murdoch, 1991). One prospective, randomised, placebo-controlled double-blind trial of nebulised salbutamol, in 19 neonates <2000g, has been identified (Singh, 2002). Serum potassium levels fell rapidly (from 7.06 +/- 0.23 mmol/L to 6.34 +/- 0.24 mmol/L, P=.003) in the first 4 hours in the treatment group (n=8) in response to 400 mcg given by nebuliser. No significant change was seen in the placebo group (n=11) (6.88 +/- 0.18 mmol/L to 6.85 +/- 0.24 mmol/L). Ditzenberger GR, Collins SD, Binder N. Continuous insulin intravenous infusion therapy for VLBW infants. J Perinat Neonat Nurs 1999;13:70-82 Helfrich E, de Vries TW, van Roon EN. Salbutamol for hyperkalaemia in children. Acta Paediatr 2001;90:1213-6 Kemper MJ, Harps E, Hellwege HH, et al. Effective treatment of acute hyperkalaemia in childhood by short- term infusion of salbutamol. Eur J Pediatr 1996;155:495-7 Murdoch IA, Dos Angos R, Haycock GB. Treatment of hyperkalaemia with intravenous salbutamol. Arch Dis Child 1991;66:527-8 Singh BS, Sadiq HF, Noguchi A, et al. Efficacy of albuterol inhalation in treatment of hyperkalemia in premature neonates. J Pediatr 2002;141:16-20 Evidence Level: II (for inhaled salbutamol) Is rectal calcium resonium a safe treatment in neonates? Intestinal perforation has been reported in infants treated with exchange resin enemas (Grammatikopoulos, 2003; Bennett, 1996), although these may have been spontaneous rather than as a result of the treatment. Nausea and vomiting are common side effects of oral administration, but changing to the rectal route is “less effective” (Helfrich, 2001). Only one randomised trial of resins in the treatment of hyperkalaemia in neonates has been identified (Hu, 1999). 40 VLBW infants were randomised to receive either glucose/insulin infusion (n=20) or kayexalate resin enema (n=20). Duration of hyperkalaemia was significantly shorter (26.4 +/- 14.9 vs 38.6 +/-13.3 hours) in the insulin group. An appropriately-sized randomised trial is necessary to evaluate the risks and benefits of this treatment in premature infants (Grammatikopoulos, 2003). Bennett LN, Myers TF, Lambert GH. Cecal perforation associated with sodium polystyrene sulfonate-sorbitol enemas in a 650 gram infant with hyperkalemia. Am J Perinatol 1996;13:167-70 Grammatikopoulos T, Greenough A, Pallidis C, et al. Benefits and risks of calcium resonium therapy in hyperkalaemic preterm infants. Acta Paediatr 2003;92:118-27 Helfrich E, de Vries TW, van Roon EN. Salbutamol for hyperkalaemia in children. Acta Paediatr 2001;90:1213-6 Hu PS, Su BH, Peng CT, et al. Glucose and insulin infusion versus kayexalate for the early treatment of non-oliguric hyperkalaemia in very-low-birth-weight infants. Acta Paediatr Taiwan 1999;40:314-8 Evidence Level: II (For no evidence of benefit of resins over glucose/insulin) Evidence Level: V (For case report evidence of harm from resins)
- 44. Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk Do some VLBW infants without renal failure suffer from hyperkalaemia? Both renal and non-renal causes of neonatal hyperkalaemia have been suggested (Singh, 2002), and the cause of the condition is generally held to be multi-factorial (Ditzenberger, 1999). One study of 48 infants (Fukuda, 1989) implicated metabolic acidosis and catabolic state, but another, in 33 infants (Stefano, 1993), found no difference in muscle protein catabolism between 12 infants with hyperkalaemia and 21 without. In a study of 18 VLBW infants (Gruskay, 1988) no differences in renal glomerular function were noted in 8 who developed hyperkalaemia and 10 who did not. Inability to regulate potassium balance, as a result of immature distal tubule function, may result in hyperkalaemia in the absence of renal failure (Mildenberger, 2002; Lorenz, 1997; Matsuo, 1995; Sato, 1995). Ditzenberger GR, Collins SD, Binder N. Continuous insulin intravenous infusion therapy for VLBW infants. J Perinat Neonat Nurs 1999;13:70-82 Fukuda Y, Kojima T, Ono, A, et al. Factors causing hyperkalemia in premature infants. Am J Perinatol 1989;6:76-9 Gruskay J, Costarino AT, Polin RA, et al. Nonoliguric hyperkalemia in the premature infant weighing less than 1000 grams. J Pediatr 1988;113:381-6 Lorenz JM, Kleinmann LI, Markarian K. Potassium metabolism in extremely low birth weight infants in the first week of life. J Pediatr 1997;131:81-6 Matsuo Y, Hasegawa K, Doi Y, et al. Erythrocyte sodium-potassium transport in hyperkalaemic and normokalaemic infants. Eur J Pediatr 1995;154:571-6 Mildenberger E, Versmold HT. Pathogenesis and therapy of non-oliguric hyperkalaemia of the premature infant. Eur J Pediatr 2002;161:415-22 Sato K, Kondo T, Iwao H, et al. Internal potassium shift in premature infants: cause of nonoliguric hyperkalemia. J Pediatr 1995;126:109-13 Singh BS, Sadiq HF, Noguchi A, et al. Efficacy of albuterol inhalation in treatment of hyperkalemia in premature neonates. J Pediatr 2002;141:16-20 Stefano JL, Norman ME. Nitrogen balance in extremely low birth weight infants with nonoliguric hyperkalemia. J Pediatr 1993;123:632-5 Evidence Level: IV What level of hyperkalaemia should prompt treatment? The criteria on which to treat hyperkalaemia have ranged from 6.8 to 7.5 mmol/L, but 6.5 mmol/L may be a better level at which to begin treatment, as rhythm disturbances are to be expected above 7.0 mmol/L (Grammatikopoulos, 2003). If treatment is not initiated until symptoms appear (or the serum level exceeds 7.0 mmol/L), the potential for success is reduced (Ditzenberger, 1999). Mortality rates may be as high as 80% once arrhythmias have appeared (Singh, 2002). Ditzenberger GR, Collins SD, Binder N. Continuous insulin intravenous infusion therapy for VLBW infants. J Perinat Neonat Nurs 1999;13:70-82 Grammatikopoulos T, Greenough A, Pallidis C, et al. Benefits and risks of calcium resonium therapy in hyperkalaemic preterm infants. Acta Paediatr 2003;92:118-27 Singh BS, Sadiq HF, Noguchi A, et al. Efficacy of albuterol inhalation in treatment of hyperkalemia in premature neonates. J Pediatr 2002;141:16-20 Evidence Level: V Last amended September 2007
- 45. Hypernatraemia 2011-13 HYPERNATRAEMIC DEHYDRATION DEFINITION In breast fed babies • Serum sodium >145 mmol/L • mild: 146–149 mmol/L • moderate: 150–169 mmol/L • severe: >170 mmol/L AIM To prevent/treat hypernatraemic dehydration while encouraging breastfeeding Other causes of hypernatraemia • Diarrhoea • Excessive perspiration • Renal dysplasia • Obstructive uropathy • Osmotic diuresis • Diabetes insipidus • Idiopathic causes • Infection (meningitis, encephalitis) • Improperly mixed formula • Sodium bicarbonate or sodium chloride administration PREVENTION Babies at high risk • Born to primiparous women • Maternal prolonged second stage of labour >1 hr • Caesarean section with delayed initiation of feeding • Maternal breast abnormalities (flat, inverted nipples)/surgery • Use of labour medications • Maternal illness, haemorrhage • Preterm <37 weeks • Maternal obesity • Maternal diabetes Action • Identify babies at risk • Immediate skin-to-skin contact at birth and breastfeed within 1 hr of life • Offer breastfeeding assistance within 6 hr of life • Ensure babies feed at least 6 times within 24 hr • If baby reluctant to feed, express breast milk (see Breast milk expression guideline) and offer by cup or syringe • Calculate required volume of feeds using local guidelines • Avoid bottle feeding and dummies • Avoid early discharge in at-risk babies • Assess baby to ensure feeding adequate • assess feeding, number of wet nappies and stools using following table
- 46. Hypernatraemia 2011-13 Day Wet nappies Stool 1–2 >2/day >1/day 3–4 >3/day >2 /day, changing in colour and consistency 5–6 >5/day >2/day, yellow in colour • Weigh between 72 and 96 hr • Refer all who have lost more than 10% weight • weight loss % = weight loss (g)/birth weight (g) × 100 Symptoms and signs • Lethargy • Irritability: fussy or unsettled during breastfeeding • Prolonged feeding >45 min • Delayed change from meconium to transitional stools • Demanding <6 feeds in 24 hr • Reduced urinary frequency • Weight loss • Jaundice • Tremor • Increased tone • Fever • Doughy skin • Seizures (usually during rehydration) • Fullness of anterior fontanelle • Physical examination can be unremarkable • usual signs (sunken fontanelle, reduced skin turgor) of dehydration can be absent Complications • Venous and arterial thrombosis • Subdural and capillary haemorrhage • Cerebral oedema • Seizures (especially following rehydration) • Apnoea and bradycardia • Cognitive and motor deficits • Hypertension • Cerebral infarction • Death Investigations • U&E • Calcium • Total bilirubin • Blood glucose • CRP • Blood culture
- 47. Hypernatraemia 2011-13 MANAGEMENT Signs or symptoms of dehydration or clinical suspicion of hypernatraemia Send blood for U&E Mild hypernatraemia • Manage in postnatal ward • Put baby to the breast and encourage mother to express breast milk (EMB), see Breast milk expression guideline • Top up baby with EBM/formula milk 100 mL/kg/day by cup or syringe • Check U&E and calcium after 12 hr • Monitor blood glucose as per Hypoglycaemia guideline • Aim to establish breastfeeding and reduce top-up once sufficient EMB • If Na+ returns to normal before sufficient EBM, liberalise feeds calculated according to local guidance • Oral feeds not tolerated • Baby unwell • Repeat U&E shows worsening hypernatraemia, moderate or severe hypernatraemia • Associated hypocalcaemia • Baby improving • continue routine postnatal care • Routine postnatal examination • Follow-up with GP and community midwife Admit to neonatal unit
- 48. Hypernatraemia 2011-13 Yes Baby admitted to neonatal unit Examine and exclude other cause of hypernatraemia Moderate or severe hypernatraemia Mild hypernatraemia Unwell baby • Put baby to breast • Top up with EBM/formula at 100 mL/kg/day via cup or syringe • If cup and syringe feeds not tolerated, pass NG tube and administer feeds (breast milk and/or formula milk) • If total enteral feeds not tolerated, give IV fluids to make up deficit Well baby Signs of shock? Resuscitate with 10 mL/kg sodium chloride 0.9% Tolerate enteral feed • Start IV fluids 100 mL/kg/day • If blood glucose >2.5 mmol, use sodium chloride 0.9% • If blood glucose <2.5 mmol, use sodium chloride 0.45% and glucose 5% or 10% • Subtract resuscitation fluid from calculated maintenance fluid Wean off formula feeds or IV fluids on to breast or EBM as tolerated by baby • U&E and blood glucose 4-hrly • Aim for rate of fall in Na + of 0.5 mmol/L/hr. If Na + falling any faster, reduce rate of rehydration • If severe hypernatraemia, contact consultant • If low blood glucose, see Hypoglycaemia guideline • If renal failure or Na + >170 mmol/L, discuss with paediatric nephrologist • Monitor 4-hrly: • temperature • heart rate • blood pressure • Keep strict fluid balance chart • Monitor weight daily • Aim to correct dehydration over 48–72 hr or slower in severe cases • Do not correct hyperglycaemia with insulin, this can reduce plasma osmolality rapidly and precipitate cerebral oedema • Once sufficient EBM, aim to establish breastfeeding and reduce top-up • Neurodevelopmental follow-up for all babies with moderate and severe hypernatraemia • Encourage mother to continue expressing breast milk in addition to breastfeeding No No
- 49. Not found an answer to your question? Contact bedsideclinicalguidelines@uhns.nhs.uk HYPERNATRAEMIC DEHYDRATION Supporting information Infants losing more than 10% of birth weight should be referred? A prospective cohort study in 2,788 term newborns (Konetzny, 2009) found that weight loss of >/= 10% of birth weight was an early indicator for hypernatraemic dehydration of sufficient severity to cause possible convulsions, permanent brain damage, or death. Sixty-seven (2.4%) newborns had a weight loss >/ = 10% of birth weight; 24 (36%) of these had moderate and 18 (27%) severe hypernatraemia. Infants born by caesarean section had a 3.4 times higher risk for hypernatraemia than those born vaginally. All newborns regained weight 24 h after additional fluids. Konetzny G, Bucher HU, Arlettaz R. Prevention of hypernatraemic dehydration in breastfed newborn infants by daily weighing. Eur J Pediatr 2009;168:815-8 Evidence Level: III Weighing babies early (72-96 hrs after birth) helps to prevent hypernatraemic dehydration? A study of outcomes pre- and post- the introduction of a policy of weighing newborns at 72-96 hrs after birth (Iyer, 2008) found 60 cases of hypernatraemic dehydration: 23 before and 37 after introduction of the policy. After the policy, there was earlier recognition (median 3 vs 6 days), lower percentage weight loss (11% vs 15%), smaller increase in sodium (147 vs 150 mmol/l), and higher breastfeeding rate at discharge (73% vs 22%) and 8 weeks (57% vs 22%). All the differences were significant (p<0.01). There was one death in the pre-policy group, and none in the post-policy group. Iyer NP, Srinivasan R, Evans K, et al. Impact of an early weighing policy on neonatal hypernatraemic dehydration and breast feeding. Arch Dis Child 2008;93:297-9 Evidence Level: IV Last amended January 2011
- 50. Hypoglycaemia 2011-13 HYPOGLYCAEMIA DEFINITION Asymptomatic hypoglycaemia • Low blood glucose concentrations are common in preterm and small-for-gestational-age infants • No simple correlation between blood glucose concentration and neuroglycopenia • Blood glucose >2.0 mmol/L is safe Symptomatic hypoglycaemia • Blood glucose <2.6 mmol/L and any of the following symptoms, provided these resolve once hypoglycaemia has been corrected: • convulsions • abnormal neurological behaviour, including hypotonia and poor response to stimulation • apnoea Symptoms cannot be attributed to hypoglycaemia if they persist after adequate treatment. Jitteriness alone does not constitute symptomatic hypoglycaemia PREVENTION • Keep all infants warm • Feed all high-risk infants within 2 hr of birth if possible • In all starved high-risk infants, institute IV infusion of glucose 10% (see below) At-risk infants Perform blood glucose estimation in: • Small for dates • Preterm • Any ill infant • Infant of diabetic mother • Beckwith-Wiedemann syndrome • Haemolytic disease of the newborn • Severe fluid restriction Monitor all at-risk infants using near-patient monitoring • First 24 hr, 3–4 hrly • Second 24 hr, 4–6 hrly • Then as necessary • Babies requiring TPN, at least daily • Babies fed enterally, immediately before feeds Always verify a low near-patient test result (<2.6 mmol/L) in a symptomatic baby by sending a sample for laboratory blood glucose estimation MANAGEMENT Never use concentrated (>20%) glucose solutions in babies Asymptomatic hypoglycaemia in at-risk infant • Correct hypothermia (see Hypothermia guideline) Feeding • Increase frequency and/or volume of feeds • milk is more beneficial than glucose 10% as it is more energy dense (70 kcal/100 mL –vs- 40 kcal/100 mL) and contains fats that promote ketoneogenesis and glucose uptake • Calculate exact amount of milk baby needs and ensure calculated amount given
- 51. Hypoglycaemia 2011-13 • seek advice from breastfeeding advisor, if available • if baby not taking full amount, top-up with nasogastric feeding • If breast milk not adequate, top-up feeding via cup with term formula first, then, if next blood glucose still <2.6, preterm formula IV glucose • Give IV glucose if: • unable to increase/tolerate feed frequency or volume or • intensive feeding does not produce normoglycaemia • Give glucose 6 mg/kg/min (glucose 10% at 90 mL/kg/day) by IV infusion • Continue enteral feeding during IV infusion • Once normoglycaemia achieved, wean from infusion as tolerated Monitor • Repeat glucose measurement after 1 hr. If low, check laboratory blood glucose • If infant develops symptoms or becomes profoundly hypoglycaemic (<1.1 mmol/L), follow Symptomatic hypoglycaemia protocol (below) immediately Symptomatic hypoglycaemia • Aim for blood glucose >2.6 mmol/L IV glucose • Give glucose 10% 2.5 mL/kg by IV bolus over 5 min into peripheral vein and follow with an infusion of at least 90 mL/kg/day (~6 mg/kg/min), that may be increased if necessary • Continue enteral feeds Monitor and adjust • Record whether symptoms respond to treatment within 30 min: very important for definitive diagnosis of symptomatic hypoglycaemia • Re-check blood glucose after 30 min. If still low, give another 2.5 mL/kg bolus and increase infusion rate to 120 mL/kg/day (8.3 mg/kg/min) except on day 1 when increase glucose concentration of infusion • Record response and repeat glucose measurement in 1 hr. If still low, check blood glucose by laboratory estimation and, if hypoglycaemia confirmed, increase delivered glucose content by increasing either volume (to 150 mL/kg/day), or concentration (12.5–20%). Glucose 20% is commercially available but please follow local policy (Table 1) Give glucose 12.5–20% centrally as extremely hypertonic. If UVC used, ensure tip not near liver Failure to respond • If >12 mg/kg/min of glucose required to achieve normoglycaemia, hyperinsulinaemic state is very likely. Obtain blood sample at time of hypoglycaemia for simultaneous measurement of: • blood glucose • plasma insulin and serum C-peptide • free fatty acids • ketones • cortisol • growth hormone • acylcarnitines • collect next passed urine for organic acid analysis • Administer glucagon 200 microgram/kg (maximum 1 mg) IM, SC, or IV. Check blood glucose within 30 min of glucagon administration, and houly thereafter until stable • If persistent hyperinsulinism suspected, seek advice from paediatric endocrinologist/metabolic paediatrician, and consider early transfer to a unit specialising in the management of such infants
- 52. Hypoglycaemia 2011-13 Routine addition of glucose polymers (e.g. Maxijul) not recommended. If decision made to use Maxijul, discuss with paediatric dietitian. Beware risk of necrotising enterocolitis Table 1: Prescription to make up 50 mL of varying concentrations of glucose solution Infusion concentration (%) Volume of 10% glucose (mL) Volume of 50% glucose (mL) 12 47.5 2.5 15 44.0 6.0 17 41.0 9.0 20 37.5 12.5 Step down • Once blood glucose normal, wean infant on to milk feeds either continuously or by hourly boluses, followed by normalising to 3-hrly feeds when blood glucose stable MONITORING • Hypoglycaemic patients: • if symptomatic, every 30 min • if asymptomatic, every hour • continue until normoglycaemic • Once normoglycaemic, 3–4 hrly until 24 hr has elapsed since last hypoglycaemic episode SEVERE PERSISTENT OR RECURRENT HYPOGLYCAEMIA Causes of recurrent, persistent neonatal hypoglycaemia • Hyperinsulinism • Endocrine deficiency, especially panhypopituitarism • Disorder of fatty acid metabolism • Disorder of carbohydrate metabolism • Disorder of amino acid metabolism • Rate of glucose infusion required is good guide to likely cause Substrate or endocrine deficiency <5 mL/kg/hr of glucose 10% required (<8 mg/kg/min) Hyperinsulinism >6 mL/kg/hr of glucose 10% required (>10 mg/kg/min) When to investigate further • Persistent recurrent hypoglycaemia, especially in ‛low-risk’ baby • Unexpectedly profound hypoglycaemia in a well baby • Hypoglycaemia in association with metabolic acidosis • Hypoglycaemia in association with other abnormalities: • midline defects • micropenis • exomphalos • erratic temperature control • Family history of SIDS, Reye’s syndrome, or developmental delay Investigations • Paired insulin and glucose estimations while hypoglycaemic (hyperinsulinism confirmed if insulin >10 picomol/L when glucose <2 mmol/L or glucose/:insulin ratio <0.3) • Urinary ketones and organic acids • Serum C-peptide • Plasma cortisol and growth hormone • Plasma amino acids • Plasma acylcarnitine • Free and total carnitines
- 53. Hypoglycaemia 2011-13 • Free fatty acids and betahydroxybuturate • Galactosaemia screen
- 54. Hypoglycaemia 2011-13 Management of glycaemic status in at-risk infants YES YES YES NO NO Symptomatic Cord blood glucose not available Check cord blood glucose • Admit to neonatal unit • Start IV glucose (10%) 90 mL/kg/day – See Symptomatic hypoglycaemia <2.6 mmol/L • Do not admit to neonatal unit unless otherwise indicated • Initiate feeding as soon as possible • Breastfeeding recommended but support mother’s choice • Check blood glucose before 2 nd feed – See Asymptomatic hypoglycaemia >2.0 mmol/L Symptomatic Asymptomatic • Continue feeding • Check blood glucose before 4 th feed >2.6 mmol/L • Continue feeding • No more blood glucose monitoring necessary unless symptomatic • Increase volume and frequency of feeds • Check blood glucose before 4th feed • Increase volume and/or concentration of IV glucose • Consider glucagon after senior advice • Investigate >2.60 mmol/L • Check blood glucose 1 hr later • Continue IV fluids • Commence and increase enteral feeds as tolerated • Monitor pre-feed blood glucose and decrease IV fluids gradually NO Asymptomatic