2. Volume 21 Number 8S McWilliams et al • S205
RF Ablation
RF ablation uses rapidly alternating
RF current to induce frictional heat
around an electrode, producing cell
death by coagulation necrosis. Small
electrode diameter, good ablation area
size, and effective marketing have com-
bined to make RF ablation a popular
technique. RF ablation also benefits
from the “oven effect”; heat retention is
improved in lesions surrounded by cir-
rhotic tissue (35). Complete ablation
rates for small to medium HCC exceed
80% in a single treatment session, and
exceed 90% with two sessions; 5-year
survival rates in the largest studies are
40%–58% (14,18,19,36 –39). Local pro-
gression after complete ablation is un-
commonly observed (1%–12%). RF abla-
tion studies are summarized in Table 1
(18,19,36 –38).
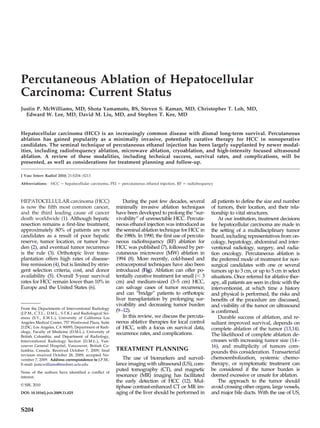
Figure. Representative percutaneous ablation devices. Clockwise from top left: Cool-Tip The most commonly used RF abla-
internally cooled RF electrode, LeVeen expandable RF electrodes, Evident 915-MHz tion devices in contemporary practice
cooled-shaft percutaneous MW antenna, and Perc-24 cryoprobe (Endocare, Irvine, Cali- are monopolar internally cooled
fornia). (Available in color online at www.jvir.org.) electrodes, such as the Cool-Tip de-
vice (Covidien, Mansfield, Massa-
chusetts), and monopolar multitined
some obliquity can usually be found that ous ethanol injection (PEI). Several non- expandable electrodes, such as the
will allow safe placement of the ablation randomized trials in the 1990s (25–27) LeVeen (Boston Scientific, Natick, Mas-
probe. CT-ultrasound fusion imaging, confirmed that PEI can safely achieve sachusetts) or RITA (Angiodynamics,
which matches a preprocedural volumet- complete necrosis of small HCCs, with Queensbury, New York) devices. Two
ric CT to real-time ultrasound images, can 5-year survival rates of 32%–38%. How- studies have been performed compar-
aid probe placement in difficult cases (17). ever, the technique suffered from the need ing the effectiveness of the two electrode
Positioning of the active tip near the large for multiple treatment sessions, uncer- types in the treatment of small HCC
and small bowel, bile ducts, stomach, gall- tainty of the ablation zone, and a high (40,41); neither study found any differ-
bladder, and diaphragm can cause collat- local progression rate of 17%–38% (28,29). ence in immediate treatment success,
eral damage and limits percutaneous ab- Several randomized controlled trials complication rate, local progression, or
lation in approximately 6–9% of cases compared PEI versus RF ablation in the overall survival between the treatment
(18,19). treatment of small HCC (30–32). These groups (40,41).
In such cases, adjunctive use of dex- Cohort studies of RF ablation have
trials demonstrated an approximately
trose solution (20), carbon dioxide shown low rates of major complications,
20% advantage for RF ablation versus PEI
(21), or balloon interposition (22) can ranging from 0.9% to 5.0%. (37,42). Peri-
in overall survival at 3–4 years, mainly as
separate and protect vital organs. toneal hemorrhage, bile duct injury, ab-
a result of a much lower incidence of local scess, and intestinal perforation were
Thermocouples can be used to moni-
tumor recurrence in the RF ablation the most notable adverse outcomes.
tor temperatures adjacent to sensitive
group. Also, approximately threefold Tumor seeding is occasionally re-
structures (23). For lesions adjacent to
main bile ducts, the placement of a fewer treatment sessions were required ported, particularly with subcapsular
nasobiliary stent with instillation of for RF ablation compared with PEI. Two tumors, but rarely occurs when careful
chilled saline can protect the ducts recent metaanalyses comparing RF abla- attention is given to technique (indi-
from thermal damage (24). These tech- tion versus PEI echoed these sentiments, rect tumor puncture, gradual increase
niques allow the vast majority of abla- declaring RF ablation superior to PEI in in power deposition, and thermocoag-
tions to be safely and effectively per- the treatment of small HCC (33,34). ulation of the needle track) (43).
formed using percutaneous technique. PEI maintains the advantage of al- RF ablation does have some disad-
lowing treatment of tumors near sensi- vantages. The majority of ablation oc-
tive organs and tissues, and avoids the curs through thermal conduction, which
HCC TREATMENT problem of the “heat-sink” effect adja- can be limited by tissue desiccation and
MODALITIES cent to vessels. The applicability of PEI charring (44). RF ablation is susceptible
Percutaneous Ethanol Injection in other situations is limited. Given the to a heat-sink effect from flowing blood,
superiority of RF ablation to PEI for the which may result in sublethal tempera-
One of the first methods devised to treatment of HCC, this review will focus tures adjacent to vessels larger than 3
ablate liver tumors involved percutane- on thermal ablation. mm in size (45– 48). As a result of elec-
3. S206 • Percutaneous Ablation of HCC August 2010 JVIR
Table 1
Percutaneous RF Ablation in de novo HCC among Cohort Studies with at Least 100 Patients and 5-year Survival Data
(18,19,36 –38)
Tumor Size Survival
(cm) Complete (%) Local Major
No. of Child Class Ablation No. of Recurrence Complications
Study, Year Pts. (A/B/C) Mean Range (%) Sessions 3y 5y (%) (%)
Lencioni et al, 2005 (18) 187 144/43/0 2.8 1.5–5.0 90 1.2† 71 48 10 2
N’Kontchou et al, 235 205/30/0 2.9 1.1–5.0 94 1.2† 60 40 12 0.9
2005 (36)
Tateishi et al, 2005 (37) 319* 221/94/4 2.6 0.8–9.7 93 1–2 78 54 2 4
Raut et al, 2005 (38) 140 59/46/35 3.0 NR 97 1 74 58 3 5
Livraghi et al, 2008 (19) 218 218/0/0 NR Յ2 98 1.1† 76 55 1 2
Note.—NR ϭ not reported.
* A total of 137 of these patients received transarterial embolization before RF ablation. Tumor size, technical success rate, local
recurrence rate, and major complication rate are composite data from de novo and recurrent HCC in this series.
† Mean.
Table 2
Details of Percutaneous Microwave Ablation in HCC among Cohort Studies with at Least 50 Patients (51–53)
Survival
Tumor Size (cm) Complete (%) Local Major
No. of Child Class Ablation Recurrence Complications
Study, Year Pts. (A/B/C) Mean Range (%) 3y 5y (%) (%)
Dong et al, 2003 (51) 234 24/207/3 4.1 1.2–8.0 89* 66 57 7% 0%
Liang et al, 2005 (52) 288 54/214/20 3.8 1.2–8.0 NR 72 51 8% NR
Lu et al, 2001 (53) 50 16/30/4 2.7 0.8–6.4 94† 73 — 6% 0%
Note.—NR ϭ not reported.
* One session.
† Two sessions.
tromagnetic interference, only one RF nae can be simultaneously activated series showed no difference in complete
electrode can be activated at one time, with MW ablation, potentially allowing ablation rate or survival between the
which can lengthen procedure time in more rapid treatment of large or multi- two techniques in HCC averaging 2.6
medium and large lesions. Finally, the focal tumors (50). Grounding pads are cm in size, despite worse underlying
grounding pads required for RF abla- not required. liver disease and more tumor multiplic-
tion can occasionally cause skin burns. Three cohort studies of percutaneous ity in the MW ablation group (55). In
These limitations have invited interest MW ablation in a mix of small to large contrast, a second unmatched series
in alternative ablation modalities de- HCC demonstrated a complete ablation in small HCC showed better survival in
scribed in the subsequent sections. rate of 89%–94%, local progression rate the RF ablation group (71% vs 49% at 3
of 6%– 8%, and 5-year survival rate of years), largely due to higher complica-
Microwave Ablation 51%–57%, despite a predominance of tion and local recurrence rates with MW
patients with Child class B disease (51– ablation (56).
Microwave (MW) ablation uses high- 53). These results compare favorably The range of complications encoun-
frequency electromagnetic energy to ag- with the results of RF ablation (Table 2) tered with MW ablation are the same as
itate water molecules, producing frictional (51–53). with RF ablation, including hemor-
heat and resultant coagulation necrosis. One randomized controlled trial (54) rhage, abscess, biliary tract injury, and
Although both modalities function by compared MW ablation versus RF abla- tumor seeding. The rate of major com-
tissue heating, MW ablation has several tion for small HCC in 72 well matched plication in most series varies from 0%
advantages versus RF ablation. MW ab- patients. The complete ablation rates to 8%, similar to RF ablation.
lation has a much broader zone of active were similar (89% for MW and 96% for The above-quoted studies of percuta-
heating, leading to higher temperatures RF). Long-term survival was not re- neous MW ablation come from Asia, us-
within the targeted zone in a shorter ported. ing a previous-generation 2450-MHz
treatment time. The active heating of The only comparative survival data microwave system. A new generation of
MW ablation is less affected by the heat- for MW versus RF ablation with percu- cooled-shaft 2450-MHz antennae prom-
sink effect, improving tumor necrosis taneous technique come from retrospec- ise ablation volumes similar to the lat-
adjacent to vessels (49). Multiple anten- tive, unmatched case series. One such est-generation RF ablation electrodes