
Recommandé
Contenu connexe
Tendances
Tendances (19)
Similaire à Poster renal biopsy
Similaire à Poster renal biopsy (20)
Plus de pryce27
Plus de pryce27 (20)
Poster renal biopsy
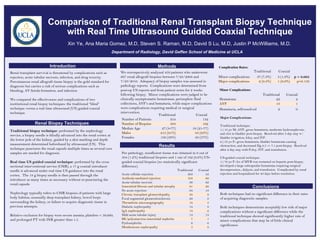
- 1. Comparison of Traditional Renal Transplant Biopsy Technique with Real Time Ultrasound Guided Coaxial Technique Xin Ye, Ana Maria Gomez, M.D, Steven S. Raman, M.D, David S Lu, M.D, Justin P McWilliams, M.D. Department of Radiology, David Geffen School of Medicine at UCLA Introduction Methods Complication Rates: Renal transplant survival is threatened by complications such as We retrospectively analyzed 459 patients who underwent Traditional Coaxial rejection, acute tubular necrosis, infection, and drug toxicity. 667 renal allograft biopsies between 7/28/2008 and Minor complications 37 (7.3%) 3 (1.9%) p = 0.005 Percutaneous renal allograft tissue biopsy is the gold standard for 7/23/2010. Adequacy of biopsy samples was assessed in Major complications 2 (0.4%) 1 (0.6%) p=0.133 diagnosis but carries a risk of serious complications such as pathology reports. Complications were determined from bleeding, AV fistula formation, and infection. post-op US reports and from patient notes for 2 weeks Minor Complications: following biopsy. Minor complications were judged to be Traditional Coaxial We compared the effectiveness and complications of two clinically asymptomatic hematomas, perinephric fluid Hematoma 22 2 institutional renal biopsy techniques: the traditional “blind” collections, AVF’s and hematuria, while major complications AVF 13 1 technique versus a real time ultrasound (US) guided coaxial were complications requiring medical or surgical Hematuria, self-resolved 2 0 technique. intervention. Traditional Coaxial Major Complications: Number of Patients 354 132 Renal Biopsy Techniques Number of Biopsies 504 162 Traditional technique: Median Age 27 (3-77) 54 (21-77) 1.) 13 yo M- AVF, gross hematuria, moderate hydronephrosis, Traditional biopsy technique: performed by the nephrology Males 215 (61%) 83 (63%) and clot in bladder post-biopsy. Resolved after 3 day stay w/ service, a biopsy needle is blindly advanced into the renal cortex at Females 139 (39%) 49 (37%) bladder irrigation, foley, and IVF. the lower pole of the kidney, guided by a skin marking and depth 2.) 53 yo F- gross hematuria, bladder hematoma causing measurement determined beforehand by ultrasound (US). This Results obstruction, and decreased Hg 8.5 -> 7.1 post-biopsy. Resolved technique punctures the renal capsule multiple times as several core after 2 day stay with Foley, IVF, and transfusion. samples are needed for diagnosis. Per pathology, insufficient tissue was obtained in 6 out of 504 (1.2%) traditional biopsies and 1 out of 162 (0.6%) US- US-guided coaxial technique: Results Real time US guided coaxial technique: performed by the cross guided coaxial biopsies (no statistically significant 1.) 76 yo F- hx of MVR was restarted on heparin post-biopsy, sectional interventional service (CSIR), a 17 g coaxial introducer difference). developed a large subcapsular hematoma requiring surgical needle is advanced under real time US guidance into the renal Traditional Coaxial decompression., dialysis, and transfusion. Complicated by renal Acute cellular rejection 303 43 rejection and hospitalized for 40 days before resolution. cortex. The 18 g biopsy needle is then passed through the introducer as many times as necessary without re-puncturing the Antibody-mediated rejection 103 60 Acute tubular necrosis 90 62 renal capsule Interstitial fibrosis and tubular atrophy 81 26 Conclusions No acute rejection 64 19 Nephrology typically refers to CSIR biopsies of patients with large Chronic transplant glomerulopathy 38 9 Both techniques had no significant difference in their rates body habitus, unusually deep transplant kidney, bowel loops Focal segmental glomerulosclerosis 29 9 of acquiring diagnostic samples. surrounding the kidney, or failure to acquire diagnostic tissue in Thrombotic microangiography 18 5 previous attempts. Diabetic nephropathy 14 8 Both techniques demonstrate acceptably low risk of major IgA nephropathy 14 2 complications without a significant difference while the Relative exclusion for biopsy were severe anemia, platelets < 50,000, Mild acute tubular injury 13 14 traditional technique showed significantly higher rate of and prolonged PT with INR greater than 1.5. BK/polyomavirus interstitial nephritis 7 1 minor complications that may be of little clinical Pyelonephritis 6 6 significance. Membranous nephropathy 5 8