Kolkata Call Girls Services 9907093804 @24x7 High Class Babes Here Call Now
Docetaxel Versus Docetaxel/Cisplatin in NSCLC
1. o riginal contribution
Docetaxel Versus Docetaxel/Cisplatin in Patients with
Advanced Non–Small-Cell Lung Cancer: Preliminary
Analysis of a Multicenter, Randomized Phase III Study
V. Georgoulias, A.G. Pallis, C. Kourousis, A. Alexopoulos, A. Ardavanis, A. Agelidou,
M. Agelidou, M. Toumbis, S. Tzannes, G. Pavlakou, P. Ziotopoulos, E. Tzelepatiotis,
N. Samaras
Abstract
The purpose of this study was to compare the efficacy and safety profile of docetaxel versus the combination
of docetaxel/cisplatin as frontline treatment of patients with advanced or metastatic non–small-cell lung can-
cer (NSCLC) in a multicenter, randomized, prospective phase III trial. Patients with unresectable stage IIIB or
metastatic stage IV NSCLC who had previously undergone no chemotherapy were allocated to receive either
docetaxel (100 mg/m2 in a 1-hour intravenous infusion; group A) or the combination of docetaxel (100 mg/m2
day 1) and cisplatin (80 mg/m2 day 2) after adequate hydration (group B). Appropriate premedication was
given before docetaxel infusion. All patients in group B received granulocyte colony-stimulating factor (150
µg/m2 subcutaneously) support from days 3 to 9 after treatment. Response and toxicity were assessed by
World Health Organization criteria. From March 1999 to November 2001, 302 patients were randomly assigned
to receive docetaxel (group A, n = 146) or docetaxel/cisplatin (group B, n = 156). The overall response rate
was significantly higher in the combination arm (18% vs. 36%; P < 0.001). However, the 2 groups did not dif-
fer in median duration of response, time to progression (TTP), median overall survival (OS), or 1-year survival
rate. Drug combination was associated with higher toxicity than single-agent therapy. Both regimens had com-
parable activity in terms of TTP and OS in chemotherapy-naive patients with advanced NSCLC; however, single-
agent therapy had a more favorable toxicity profile.
Clinical Lung Cancer, Vol. 4, No. 5, 288-293, 2003 Key words: Chemotherapy, Growth factors, Platinum
agents, Taxanes
Introduction and induces microtubule bundle formation in cells.4 Several
Non–small-cell lung cancer (NSCLC) remains the leading phase II trials have evaluated the activity of docetaxel in previ-
cause of cancer-related death in men and women in Western ously untreated patients with NSCLC. Docetaxel as single-
countries and accounts for 80% of lung cancer cases.1 The prog- agent therapy (100 mg/m2 and 75 mg/m2 every 3 weeks) has
nosis of patients with NSCLC is poor; only one third have re- produced response rates of 26%-54%.5-10 In addition, docetaxel
sectable disease at diagnosis and more than half die from subse- is active in patients who are refractory or resistant to cisplatin,
quent relapse and metastases. Furthermore, patients with metasta- producing responses ranging from 18% to 25%, implying a lack
tic disease have a median survival of approximately 5-6 months.2 of cross-resistance between docetaxel and cisplatin, probably be-
Docetaxel is a semisynthetic taxane derived from 10-deacetyl cause of their different mechanisms of action.11
baccatin III3 and, like paclitaxel, promotes the in vitro assembly For > 10 years, cisplatin-based chemotherapy represented the
of stable microtubules in the absence of guanosine triphosphate cornerstone treatment for advanced NSCLC. A large meta-
analysis of 8 randomized trials (N = 778) of cisplatin-based
chemotherapy compared with best supportive care demonstrat-
Lung Cancer Group, Hellenic Oncology Research Group (LCG-HORG), ed an advantage of chemotherapy, with a 27% reduction in the
and Department of Medical Oncology, University Hospital of Heraklion,
Crete, Greece risk of death and a 10% increase in 1-year survival rate.12 Fur-
Submitted: Dec 27, 2002; Revised: Mar 6, 2003; Accepted: Mar 14, 2003
thermore, an analysis of survival determinants in > 2500 pa-
Address for correspondence: V. Georgoulias, MD, Department of Medical
tients proved that the use of cisplatin was an independent pre-
Oncology, University Hospital of Heraklion, P.O. Box 1352, 71110, dictor of survival.13 However, cisplatin has a low therapeutic
Heraklion, Crete, Greece ratio and is related to severe toxicity (nausea and vomiting, renal
Fax: 30-810-392802; e-mail: georgoul@med.uoc.gr
toxicity, neuropathy, and ototoxicity).14 Therefore, the combi-
288 Clinical Lung Cancer March 2003
2. nation of cisplatin with a new-generation agent such as doce- chemistry, chest radiography, computed tomography (CT) of
taxel was a logical step to develop more active regimens against the chest, abdomen, and brain, and whole-body radionuclide
NSCLC. Phase II studies of the docetaxel/cisplatin combination bone scan. Baseline evaluation had to be performed within 2
reported response rates of 33.4%-45.5% and median survival weeks before therapy initiation. All measurable lesions were
durations of 8.4-13 months.15-17 identified at baseline and were monitored throughout. During
A recently published metaanalysis compared the effect of sin- treatment, a complete blood cell count was performed weekly;
gle-agent versus combination chemotherapy on response rate, in case of grade 3 or 4 neutropenia, febrile neutropenia, or
toxicity, and survival in 25 trials including 5156 patients with grade 4 thrombocytopenia, the complete blood cell count was
advanced NSCLC. Overall, combination chemotherapy pro- done daily until resolution to a grade ≤ 1. A complete medical
duced a nearly 2-fold increase in response rate. However, sur- history analysis and a detailed physical examination with blood
vival at 12 months was modestly superior with combination biochemistry, EKG, and chest radiography were performed be-
chemotherapy. Additionally, combination chemotherapy also fore each treatment administration to assess disease status and
increased toxicity significantly, including a 3.6-fold increase in treatment toxicity. Lesions were evaluated after each cycle by
the risk of treatment-related death.18 clinical examination or chest radiography when appropriate; all
Based on these data, the Lung Cancer Group of the Hellenic patients were assessed for response every 3 courses of chemo-
Oncology Research Group conducted a prospective, multicen- therapy. Objective tumor responses were evaluated according to
ter, randomized phase III trial comparing docetaxel versus the WHO response criteria.19 Assessment of the lesions was per-
docetaxel/cisplatin combination in patients with previously un- formed by the same method on each occasion. All CT scans
treated, unresectable, locally advanced (stage IIIB) and/or were reviewed by an independent radiologist. Objective re-
metastatic (stage IV) NSCLC. sponses were confirmed by repeating the CT scans 1 month
later. After completion of study treatment, patients were fol-
Patients and Methods lowed every 2 months during the first year. Second-line thera-
Patients py included best supportive care, palliative radiation therapy, or
The inclusion criteria for this study was histologically or cy- reinduction to study treatment. Treatment with a platinum-
tologically confirmed, unresectable, locally advanced (stage containing regimen was not permitted in the docetaxel
IIIB) and/or metastatic (stage IV) NSCLC. Additionally, eligi- monotherapy group.
ble patients were 18-75 years of age with bidimensionally meas-
urable disease, life expectancy > 3 months, and a World Health Randomization and Treatment
Organization (WHO) performance status (PS) ≤ 2. All patients Patients were centrally randomized by computer software to a
had to be chemotherapy-naive. Previous radiation therapy, ei- 1:1 ratio to receive either single-agent docetaxel (group A) or
ther in the adjuvant setting or for the treatment of bone metas- docetaxel/cisplatin (group B). The randomization to each arm
tases, was allowed provided that the measurable lesions were was done by stratification according to PS and stage of disease.
outside the radiation fields. Patients with known, symptomatic In the single-agent arm, docetaxel was given at the dose of
central nervous system metastases were ineligible. Serum biliru- 100 mg/m2 as a 1-hour intravenous infusion. The doses of the
bin levels had to be ≤ 1.5 times the upper normal limit (UNL); administered drugs in the combination arm were based on our
aspartate aminotransferase and alanine aminotransferase levels previous experience.15 We have previously shown that docetaxel
had to be ≤ 2.5 times UNL in the absence of demonstrable liver at the dose of 100 mg/m2 and cisplatin at the dose of 80 mg/m2,
metastases or ≤ 5 times UNL in the presence of liver metastases. followed by adequate hydration, administered every 3 weeks,
Adequate renal function was also required (serum creatinine with granulocyte colony-stimulating factor (G-CSF) support is
level ≤ 1.5 times UNL). Neutrophil count had to be ≥ 1.5 × feasible and active in previously untreated patients with ad-
109/L and platelet count ≥ 100 × 109/L. Active infection, his- vanced NSCLC.15 Therefore, docetaxel was administered on
tory of significant cardiac disease (ie, unstable angina, conges- day 1 at a dose of 100 mg/m2 over a 1-hour intravenous infu-
tive heart failure, myocardial infarction within the previous 6 sion and cisplatin was administered on day 2 at a dose of 80
months, and/or ventricular arrhythmias), and malnutrition (loss mg/m2 after adequate hydration. All patients in group B re-
of ≥ 20% of original body weight) were criteria for exclusion. ceived G-CSF (150 µg/m2 subcutaneously) from days 3 to 9
All patients gave written informed consent to participate in the after treatment.
study and the trial was approved by the ethics and scientific The same antiemetic treatment was given to patients in both
committees of the participating centers. The study was con- study groups according to the common practice of the partici-
ducted according to the Helsinki Declaration and good clinical pating centers. All patients received standard pre- and post-
practice guidelines. medication with 8 mg dexamethasone at 7 hours and 1 hour be-
fore docetaxel administration and 16 mg dexamethasone in 2
Patient Evaluation divided doses daily for 3 additional days to reduce the risk of al-
Baseline assessment was necessary for all patients and consist- lergic reactions and docetaxel-associated fluid retention syn-
ed of complete medical history, physical examination and vital drome. Both regimens were repeated every 3 weeks. Treatment
signs, evaluation of PS, 12-lead electrocardiography (EKG), was continued until disease progression, the appearance of un-
complete blood cell count with differential and blood bio- acceptable toxicity, or patient withdrawal of consent.
Clinical Lung Cancer March 2003 289
3. Docetaxel Versus Docetaxel/Cisplatin in Advanced NSCLC
Toxicity Table 1 Patient Characteristics in Group A (Docetaxel) and
All adverse events were recorded along with a description of Group B (Docetaxel/Cisplatin)
the event and were graded according to WHO common toxici-
Group A Group B
ty criteria.19 In any case of grade 4 neutropenia, febrile neu- (n = 146) (n = 156)
tropenia, or grade 3 or 4 thrombocytopenia, treatment was de-
Age (Years)
layed until the resolution of toxicity to grade ≤ 1, and dosages
of both drugs were reduced by 15%. In cases of grade 3/4 neu- Median 63 61
rotoxicity and fatigue, treatment was delayed 1-2 weeks and
Range 41-75 33-76
dosages of both drugs were reduced by 25%. Dose reductions
were maintained for all subsequent cycles of treatment. Sex
Male 131 (90%) 147 (94%)
Statistical Analysis
The primary endpoint was overall survival (OS); secondary Female 15 (10%) 9 (6%)
endpoints included overall response rate (ORR) with the 2 reg- WHO Performance Status
imens, safety profile, and time to progression (TTP). The study
0 62 (42%) 64 (41%)
was designed to have 90% power to detect a difference in me-
dian survival of 7 months for the single-agent docetaxel arm ver- 1 69 (47%) 80 (51%)
sus 12 months for the docetaxel/cisplatin/G-CSF arm at the sta-
2 15 (10%) 12 (8%)
tistically significant level of 5%. One hundred fifty evaluable pa-
tients should be enrolled in each arm to achieve the statistical Histological Type
requirements of the fixed sample size design.20 Adenocarcinoma 52 (36%) 55 (35%)
Descriptive statistics for both groups are reported as mean,
median, and range. Statistical comparisons between groups were Nonadenocarcinoma 94 (64%) 101 (65%)
assessed by Pearson χ2 test for proportions (or Fisher Exact test Stage
where appropriate).20 Differences between groups in terms of
IIIB 52 (36%) 57 (37%)
survival data were assessed by the log-rank and Wilcoxon tests
(Kaplan-Meier analysis).21 IV 94 (64%) 99 (63%)
The duration of response was calculated from the day of the Number of Organs Involved
first documentation of response to disease progression; OS was
measured from entry to the study until death, and the 1-year Median 2 2
survival was estimated with use of the Kaplan-Meier method.21 Range 1-4 1-5
The TTP was measured from enrollment into the study until
Previous Treatment
the day of the first evidence of disease progression.
Surgery 16 (11%) 9 (6%)
Results Radiation therapy 4 (3%) 6 (4%)
Patient Characteristics
At the time of present interim analysis (March 2002), 302 pa- Abbreviation: WHO = World Health Organization
tients were enrolled in the study; 146 were enrolled on the doce-
taxel arm and 156 on docetaxel/cisplatin/G-CSF arm. One hun-
dred patients in the docetaxel group and 115 in the days for single-agent and combination groups, respectively).
docetaxel/cisplatin group were evaluable for efficacy and all pa- Treatment administration was delayed in 56 cycles (11%) in the
tients in both groups were evaluable for toxicity. Eighty-seven pa- docetaxel group and 110 cycles (17%) in the docetaxel/cispla-
tients were not evaluable for response for the following reasons: tin/G-CSF group (P = 0.005). Three cycles (5.4%) in the doce-
too early for evaluation (n = 51), disease response assessment not taxel group and 10 cycles (9.3%) in the docetaxel/cisplatin/G-
yet available (n = 27), or received only 1 cycle of chemotherapy CSF group were delayed because of hematologic toxicity (P =
(n = 9). Patient characteristics were well balanced between 0.038); moreover, 1 cycle (2%) in the docetaxel group and 11
groups with respect to several prognostic factors. Patient charac- (10%) in the docetaxel/cisplatin/G-CSF group (P = 0.019) were
teristics are presented in Table 1. delayed because of nonhematologic toxicity. All other cycles
were delayed for reasons not related to treatment or toxicity (ie,
Treatment patient request for personal reasons, pending imaging studies
A total of 513 and 647 chemotherapy cycles were adminis- for response assessment). Dose reductions were not common,
tered in group A and group B, respectively. The median number occurring in 1.2% of cycles in the single-agent arm and 4% in
of cycles received per patient was 3.0 for the docetaxel group the combination therapy arm. Dose reductions in the docetaxel
(range, 1-12 cycles) and 4.0 for the docetaxel/cisplatin/G-CSF group mainly resulted from hematologic toxicity; in the doce-
group (range, 1-9 cycles). The median interval between cycles taxel/cisplatin/G-CSF group, dose reductions resulted from
was 21 days for both groups (ranges of 21-32 days and 21-34 both hematologic and nonhematologic toxicity.
290 Clinical Lung Cancer March 2003
4. V. Georgoulias et al
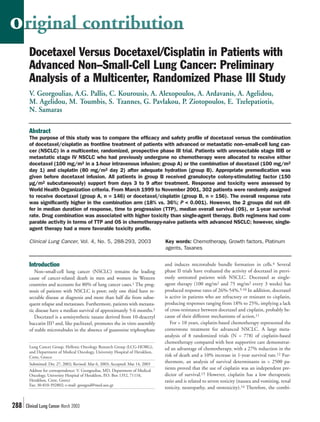
Table 2 Efficacy Results of Docetaxel and Docetaxel/Cisplatin Figure 1 Proportions of Patients with Grade 3/4 Anemia,
Neutropenia, or Thrombocytopenia by Treatment Group
Docetaxel/ P
Result Docetaxel
Cisplatin Value 25
Docetaxel
Overall Response Rate 18% 36% < 0.001
20 Docetaxel/Cisplatin
Complete response – 2% –
Patients (%)
15
Partial response 16% 33% –
Stable disease 22% 22% – 10
Progressive disease 60% 42% – 5
*
Median Duration of 0
8 (1-12) 6.5 (0.5-25) NS
Response, Months (Range) Anemia Neutropenia Thrombocytopenia
TTP, Months (Range) 7 (2-17) 8.5 (1-31) 0.308
*P = 0.01
Median Follow-up,
4 (0.5-27.5) 6 (0.5-31) NS
Months (Range)
Median Survival, thrombocytopenia. However, no patient in the combination group
10 (0.5-27.5) 13 (0.5-31) 0.471
Months (Range) had bleeding episodes or required platelet transfusions.
1-Year Survival 40% 45% NS The incidence of grade 3 nausea and vomiting was significantly
higher in the combination therapy group than in the single-agent
Abbreviations: NS = not significant, TTP = time to progression group (7% vs. 0%; P = 0.02). Furthermore, the incidence of grade
3/4 diarrhea was significantly higher in the combination group
(7% vs. 2% with docetaxel alone; P = 0.04). The frequency of
Response to Treatment grade 2-4 nephrotoxicity was significantly lower in the docetaxel
There were no complete responses in patients in the docetaxel arm (0% vs. 4.5% with combination therapy; P = 0.006). Neuro-
group; 24 patients (16%) achieved a partial response in this group. toxicity of grades 2-4 was similar between groups (docetaxel vs.
Similarly, 3 (2.0%) and 49 patients (31%) experienced complete docetaxel/cisplatin/G-CSF: 4.1% vs. 5.1%; P = NS). Mild hyper-
and partial responses, respectively, in the docetaxel/cisplatin/G- sensitivity reactions were seen in 9 patients (6.0%) in the docetaxel
CSF group. The ORRs were 18% (95% confidence interval [CI]: group and 4 patients (2.5%) in the docetaxel/cisplatin/G-CSF
11.60%-24.76%) for the docetaxel group and 36% (95% CI: group (P = NS). Incidence of nonhematologic toxicity is present-
27.64%-43.10%) for the docetaxel/cisplatin/G-CSF group (in- ed in Table 3.
tent-to-treat analysis; P < 0.001). However, no statistically signifi- There were no treatment-related deaths in the docetaxel group,
cant difference was observed between the docetaxel monotherapy whereas 5 (3.2%) treatment-related deaths (from febrile neutrope-
and combination groups regarding the median duration of re- nia, n = 2; grade 3 diarrhea and grade 3 vomiting, n = 1; grade 3
sponse, median TTP, and median OS (Table 2). After a median anemia and non-neutropenic infection, n = 1; and acute renal fail-
follow-up period of 4 and 6 months for single-agent and combi- ure, n = 1) were observed in the docetaxel/cisplatin/G-CSF group
nation groups, respectively, the median OS was 10 months for the (P = 0.02).
docetaxel arm and 13 months for the docetaxel/cisplatin/G-CSF
arm (P = 0.471). Thirty-two percent of the patients in the single- Discussion
agent arm and 22% in the combination arm received second-line The results of the present study demonstrate that docetaxel
chemotherapy (P = not significant [NS]). single-agent therapy has a more favorable toxicity profile than
the docetaxel/cisplatin/G-CSF combination regimen in the
Toxicity studied population. Granulocyte colony-stimulating factor sup-
The incidence of severe hematologic toxicity (grade 3 and 4) is port was given in the docetaxel/cisplatin arm so the incidence of
presented in Figure 1. Grade 3 or 4 neutropenia was observed in grade 3/4 neutropenia was similar between arms. However,
30 patients (20.6%) and 39 patients (25.0%) on the docetaxel and thrombocytopenia and nonhematologic toxicities (Table 3)
docetaxel/cisplatin/G-CSF arms, respectively. Eleven patients were more common in the combination group. Finally, there
(7.5%) in the single-agent arm and 15 patients (9.5%) in the com- were no treatment-related deaths in the docetaxel group, where-
bination therapy arm developed febrile neutropenia. Grade 3 or 4 as 5 (3.2%) treatment-related deaths were observed in the doce-
anemia occurred relatively infrequently. Three patients (2%) in the taxel/cisplatin/G-CSF group (P = 0.02).
single-agent arm and 3 patients (1.9%) in the combination group The comparison of docetaxel monotherapy with the doce-
developed grade 3 or 4 anemia. Thrombocytopenia was more taxel/cisplatin/G-CSF combination revealed that the combina-
common in the combination group. Grade 3 or 4 thrombocy- tion regimen is significantly more active than docetaxel
topenia was observed in 5 patients (3.2%) in the combination monotherapy in terms of response rate (18% vs. 36%; P < 0.001).
group; no patient in the docetaxel group developed grade 3 or 4 Although there was a trend toward better duration of response,
Clinical Lung Cancer March 2003 291
5. Docetaxel Versus Docetaxel/Cisplatin in Advanced NSCLC
Table 3 Grade 3/4 Nonhematologic Toxicity by Treatment Group
dration, leading to a prolonged hospital stay. The other platinum
compound, carboplatin, is easier to administer but produces
Docetaxel/
Docetaxel P more severe myelosuppression, especially thrombocytopenia. All
Cisplatin
Group Value these factors bring up the issue of whether a platinum compound
Group
should be a mandatory component of chemotherapy in NSCLC.
Nausea/Vomiting 0 11 (7.0%) 0.02
There are very few published randomized trials comparing
Diarrhea 3 (2.0%) 11 (7.0%) 0.04 platinum-based combinations with the corresponding non-plat-
inum monotherapies. In one of these studies that compared
Mucositis 1 (0.7%) 2 (1.3%) NS
gemcitabine versus gemcitabine/cisplatin, there was no differ-
Nephrotoxicity* 0 7 (4.5%) 0.006 ence in OS.22 The comparison of single-agent paclitaxel versus
Neurotoxicity* 6 (4.1%) 8 (5.1%) NS paclitaxel/carboplatin demonstrated a higher response rate and
a higher OS in favor of the combination arm.23 Similarly, a re-
Fatigue 6 (4.1%) 11 (7.0%) NS cent report on 332 patients treated with gemcitabine alone or
Fluid Retention Syndrome 1 (0.7%) 1 (0.6%) NS the gemcitabine/carboplatin combination also demonstrated a
higher response rate (30% vs. 12%) and median survival (6
* Grades 2-4. months vs. 4 months) in favor of the combination arm.24 Drug
Abbreviation: NS = not significant.
combination was associated with higher toxicity rates than sin-
gle-agent therapy in all trials.
Based on these preliminary results, we can propose that sin-
TTP, OS, and 1-year survival in the combination arm, this dif-
gle-agent docetaxel may offer an alternative in the first-line
ference failed to reach statistical significance. This may be at-
treatment of patients with advanced NSCLC, especially those
tributed to the increased toxicity in the combination arm. The
who cannot tolerate platinum-based regimens.
ORR of 16%, the median survival of 10 months, and the 1-year
survival rate of 40% observed in the single-agent arm are simi-
Participating Institutions
lar to results reported in previous studies of docetaxel monother-
Participating Centers in the Lung Cancer Group of the Hel-
apy, with the exception of ORR, which is slightly lower than
lenic Oncology Research Group are as follows:
those seen in earlier phase II studies.5-10 Similarly, for the doce-
Department of Medical Oncology, University Hospital of
taxel/cisplatin/G-CSF combination, the ORR is slightly lower
Crete (V. Georgoulias, A.G. Pallis, C. Kourousis, N. An-
than that reported in our previous phase II study, whereas me-
droulakis); 1st Department of Pulmonary Diseases (F. Apos-
dian survival and 1-year survival are quite similar.15 The lower
tolopoulou, X. Tsiafiaki, M. Agelidou) and 2nd Department of
degree of activity observed in this study may reflect the early in-
Pulmonary Diseases (P. Ziotopoulos, F. Palamidas), Sisman-
terim data analysis or may be a more accurate indication of the
ogleion Hospital, Athens; Department of Medical Oncology,
true response rate.
General Hospital of Larisa (A. Athanasiadis); 1st Department of
Some important differences were observed between the 2
Pulmonary Diseases (E. Papadakis, A. Agelidou), 3rd Depart-
groups regarding toxicity. The combination of docetaxel/cispla- ment of Pulmonary Diseases (O. Anagnostopoulos, F. Pavlakas,
tin was more myelotoxic than docetaxel monotherapy, with a A. Rapti), 6th Department of Pulmonary Diseases (M.
significantly higher incidence of thrombocytopenia. Further- Toumbis), 7th Department of Pulmonary Diseases (S. Tzannes,
more, the incidences of grade 3 nausea and vomiting and grade E. Grigoratou), Department of Internal Medicine, Medical On-
3/4 diarrhea were significantly higher in the docetaxel/cisplatin cology Unit (K. Syrigos), and University Department of Pul-
arm than in the monotherapy arm, and these adverse events monary Diseases (M. Veslemes), Sotiria Hospital, Athens; 1st
were the reason for 1 treatment-related death. As expected, Department of Internal Medicine, Agios Savvas Cancer Hospi-
nephrotoxicity was observed mainly in the combination group. tal, Athens (A. Alexopoulos, A. Ardavanis); Department of In-
Finally, significantly more treatment-related deaths occurred in ternal Medicine, Laiko Hospital, Athens (A. Polyzos); Depart-
the combination arm than in the single-agent arm. ment of Internal Medicine, Medical Oncology Unit, Patision
Locally advanced and metastatic NSCLC remains a fatal dis- Hospital, Athens (E. Tselepatiotis); 1st Department of Pul-
ease. Hence, the principal goals of treatment should be pallia- monary Diseases (N. Samaras) and 2nd Department of Pul-
tion, acceptable quality of life, and prolonged survival. There- monary Diseases (N. Galanis), Papanikolaou Hospital, Thessa-
fore, the toxicity profile of a particular chemotherapeutic regi- loniki; and 2nd Department of Pulmonary Diseases,
men should be an important issue. The toxicity of cisplatin re- Theageneio Hospital, Thessaloniki (J. Stergiou, P. Papakotoulas,
mains a serious clinical problem. Nausea and emesis are often P. Makrantonakis, I. Boukovinas).
severe and delayed; furthermore, neurotoxicity, renal toxicity,
and ototoxicity may be significant and dose-related. An impor- References
01. Ginsberg RJ, Vokes EE, Raben A. Non small cell lung cancer. In: DeVita VT Jr, Hell-
tant proportion of patients with NSCLC are elderly and have man S, Rosenberg SA, eds. Principles and Practice in Oncology. 5th ed. Philadelphia, PA:
concomitant cardiac or cardiorespiratory diseases in which the Lippincott-Raven; 1997:858-911.
02. Feigal EG, Christian M, Cheson B, et al. New chemotherapeutic agents in non-small-
administration of cisplatin is relatively contraindicated. Addi- cell lung cancer. Semin Oncol 1993; 20:185-201.
tionally, the administration of cisplatin requires the need for hy- 03. Mangatal L, Adeline MT, Guenard D. Application of the vicinal oxyaminaton reaction
292 Clinical Lung Cancer March 2003
6. V. Georgoulias et al
with asymmetric induction to the hemisynthesis of taxol and analogues. Tetrahedron 14. Schiller JH. Current standards of care in small-cell and non-small-cell lung cancer. On-
1989; 45:4177-4190. cology 2001; 61(suppl 1):3-13.
04. Gueritte-Voegelein F, Guenard D, Lavelle F, et al. Relationships between the structure 15. Georgoulias V, Androulakis N, Dimopoulos AM, et al. First-line treatment of advanced
of taxol analogues and their antimitotic activity. J Med Chem 1991; 34:992-998. non-small-cell lung cancer with docetaxel and cisplatin: a multicenter phase II study.
05. Cerny T, Kaplan S, Pavlidis N, et al. Docetaxel (Taxotere) is active in non-small-cell Ann Oncol 1998; 9:331-334.
lung cancer: a phase II trial of the EORTC Early Clinical Trials Group (ECTG). Br J 16. Le Chevalier T, Monnier A, Douillard JY, et al. Docetaxel (Taxotere) plus cisplatin: an
Cancer 1994; 70:384-347. active and well-tolerated combination in patients with advanced non-small cell lung
06. Fossella FV, Lee JS, Murphy WK, et al. Phase II study of docetaxel for recurrent or cancer. Eur J Cancer 1998; 34:2032-2036.
metastatic non-small-cell lung cancer. J Clin Oncol 1994; 12:1238-1244. 17. Zalcberg J, Millward M, Bishop J, et al. Phase II study of docetaxel and cisplatin in ad-
07. Francis PA, Rigas JR, Kris MG, et al. Phase II trial of docetaxel in patients with stage vanced non-small-cell lung cancer. J Clin Oncol 1998; 16:1948-1953.
III and IV non-small-cell lung cancer. J Clin Oncol 1994; 12:1232-1327. 18. Lilenbaum RC, Langenberg P, Dickersin K. Single agent versus combination chemo-
08. Lira-Puerto V, Zepeda G, Mohar A, et al. Phase II trial of Taxotere (docetaxel) in ad- therapy in patients with advanced nonsmall cell lung carcinoma: a meta-analysis of re-
vanced non-small cell lung cancer. Proc Am Soc Clin Oncol 1995; 14:382 (Abstract sponse, toxicity, and survival. Cancer 1998; 82:116-126.
#1186). 19. Miller AB, Hoogstraten B, Staquet M, et al. Reporting results of cancer treatment. Can-
09. Miller VA, Rigas JR, Francis PA, et al. Phase II trial of a 75-mg/m2 dose of docetaxel cer 1981; 47:207-214.
with prednisone premedication for patients with advanced non-small cell lung cancer. 20. Altman GD. Practical Statistics for Medical Research. London, UK: Chapman and Hall;
Cancer 1995; 75:968-972. 1991.
10. Roszkowski K, Pluzanska A, Krzakowski M, et al. A multicenter, randomized, phase III 21. Collet D. Modeling Survival Data in Medical Research. 3rd ed. Oxford, UK: Blackwell
study of docetaxel plus best supportive care versus best supportive care in chemother- Scientific; 1994.
apy-naive patients with metastatic or non-resectable localized non-small cell lung can- 22. Berardi R, Porfiri E, Massidda B, et al. Gemcitabine (GEM) and cisplatin (PL) versus
cer (NSCLC). Lung Cancer 2000; 27:145-157. gemcitabine alone in stage IV non-small cell lung cancer (NSCLC): preliminary results
11. Fossella FV, Lee JS, Berille J, et al. Summary of phase II data of docetaxel (Taxotere), of a randomized multicenter phase III study. Proc Am Soc Clin Oncol 2001; 20:347a
an active agent in the first- and second-line treatment of advanced non-small cell lung (Abstract #1385).
cancer. Semin Oncol 1995; 22(suppl 4):22-29. 23. Lilenbaum RC, Herndon J, List M, et al. Single-agent (SA) versus combination chemo-
12. Non-Small-Cell Lung Cancer Collaborative Group. Chemotherapy in non-small-cell therapy (CC) in advanced non-small cell lung cancer (NSCLC): a CALGB randomized
lung cancer: a meta-analysis using updated data on individual patients from 52 ran- trial of efficacy, quality of life (QOL), and cost-effectiveness. Proc Am Soc Clin Oncol
domized clinical trials. BMJ 1995; 311:899-909. 2002; 21:1a (Abstract #2).
13. Albain KS, Crowley JJ, LeBlanc M, et al. Survival determinants in extensive-stage non- 24. Sederholm C. Gemcitabine (G) compared with gemcitabine plus carboplatin (GC) in ad-
small-cell lung cancer: the Southwest Oncology Group experience. J Clin Oncol 1991; vanced non-small cell lung cancer (NSCLC): a phase III study by the Swedish Lung Can-
9:1618-1626. cer Study Group (SLUSG). Proc Am Soc Clin Oncol 2002; 21:291a (Abstract #1162).
Clinical Lung Cancer March 2003 293