

Contenu connexe
Tendances
En vedette
En vedette (20)
Similaire à 23205059
Similaire à 23205059 (20)
Dernier
Dernier (20)
23205059
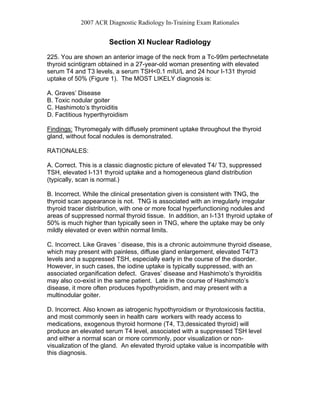
- 1. 2007 ACR Diagnostic Radiology In-Training Exam Rationales Section XI Nuclear Radiology 225. You are shown an anterior image of the neck from a Tc-99m pertechnetate thyroid scintigram obtained in a 27-year-old woman presenting with elevated serum T4 and T3 levels, a serum TSH<0.1 mIU/L and 24 hour I-131 thyroid uptake of 50% (Figure 1). The MOST LIKELY diagnosis is: A. Graves’ Disease B. Toxic nodular goiter C. Hashimoto’s thyroiditis D. Factitious hyperthyroidism Findings: Thyromegaly with diffusely prominent uptake throughout the thyroid gland, without focal nodules is demonstrated. RATIONALES: A. Correct. This is a classic diagnostic picture of elevated T4/ T3, suppressed TSH, elevated I-131 thyroid uptake and a homogeneous gland distribution (typically, scan is normal.) B. Incorrect. While the clinical presentation given is consistent with TNG, the thyroid scan appearance is not. TNG is associated with an irregularly irregular thyroid tracer distribution, with one or more focal hyperfunctioning nodules and areas of suppressed normal thyroid tissue. In addition, an I-131 thyroid uptake of 50% is much higher than typically seen in TNG, where the uptake may be only mildly elevated or even within normal limits. C. Incorrect. Like Graves ’ disease, this is a chronic autoimmune thyroid disease, which may present with painless, diffuse gland enlargement, elevated T4/T3 levels and a suppressed TSH, especially early in the course of the disorder. However, in such cases, the iodine uptake is typically suppressed, with an associated organification defect. Graves’ disease and Hashimoto’s thyroiditis may also co-exist in the same patient. Late in the course of Hashimoto’s disease, it more often produces hypothyroidism, and may present with a multinodular goiter. D. Incorrect. Also known as iatrogenic hypothyroidism or thyrotoxicosis factitia, and most commonly seen in health care workers with ready access to medications, exogenous thyroid hormone (T4, T3,dessicated thyroid) will produce an elevated serum T4 level, associated with a suppressed TSH level and either a normal scan or more commonly, poor visualization or non- visualization of the gland. An elevated thyroid uptake value is incompatible with this diagnosis.
- 2. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 226. You are shown flow, immediate and delayed static spot images (Figure 2A) and delayed whole body images (Figure 2B) from a three-phase Tc-99m MDP (methylene diphosphonate) bone scan in a previously healthy 11 year-old boy, presenting with worsening knee pain and fever. Which of the following diagnoses is MOST consistent with the imaging findings? A. Tibial stress fracture B. Reflex sympathetic dystrophy C. Metastatic neuroblastoma D. Osteomyelitis FINDINGS: There is moderate focal hyperemia to the proximal left tibia. The delayed static images demonstrate diffusely increased bone uptake in this region, with a lesser degree of increased cortical uptake noted in the proximal and mid left tibial shaft. Additional sites of asymmetrically increased uptake are noted in the region of the right shoulder and left hip joints. RATIONALES: A. Incorrect. The extent of the lesion is greater than typically seen with a stress fracture. In addition, there is also abnormal uptake at the right shoulder and left hip, indicating a multifocal process. B. Incorrect. Again, this is a multifocal process, and the distribution of the abnormality is not typical of reflex sympathetic dystrophy (RSD), which classically produces a “glove and stocking” peripheral distribution. C. Incorrect. Neuroblastoma can certainly metastasize to bone, and would typically involve the region of the physes (as in this case). However, osteomyelitis is a more likely diagnosis in an 11-year-old child. D. Correct. Although not specific, the findings in this case are consistent with multifocal osteomyelitis, which is the most likely diagnosis of the options listed. REFERENCES: Taylor A, Datz. Clinical Practice of Nuclear Medicine. Churchill Livingstone. 1991. Zeissman HA, O’Malley JP, Thrall JH: Nuclear Medicine-The Requisites. 3rd ed. Mosby. 2006.
- 3. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 227. You are shown serial images (Figure 3A and 3B) from a Tc-99m diethylene- triamine-pentaacetic acid (DTPA) radionuclide CNS shunt study. Which one of the following statements is CORRECT? A. This is a normal study. B. There is high-grade obstruction of the efferent limb of the shunt. C. There is abnormal loculation of activity in the peritoneal cavity. D. There is scintigraphic evidence of diffuse peritonitis. FINDINGS: The immediate static image demonstrates activity within the V-P shunt reservoir and early passage of activity into the efferent limb of the shunt, progressing inferiorly along the right lateral neck and upper chest. Subsequent images demonstrate visualization of activity in the distal portion of the shunt catheter, overlying the right lower quadrant of the abdomen at 10-20 minutes post-injection. Further delayed images demonstrate progressive accumulation of activity within the peritoneal cavity in the right lower quadrant from 30-60 minutes. A final image of the abdomen at 120 minutes demonstrates free intraperitoneal dispersion of the tracer. RATIONALES A. Correct. This study demonstrates normal progression of the tracer throughout the shunt catheter, with normal drainage into the peritoneal cavity, without evidence of loculation. B. Incorrect. There is normal transit of tracer through the shunt, without evidence of obstruction, which would appear either as non-entry of the dose into the efferent limb, an abrupt stoppage of the tracer within the shunt catheter or failure of free intaperitoneal dispersion of tracer. C. Incorrect. Intraperitoneal loculation might be suspected on the images obtained at 30-60 minutes, but the further 120 minute delayed image clearly demonstrates free intraperitoneal dispersion, without evidence of loculation. D. Incorrect. The finding of diffuse peritoneal activity on the 120 minute image is a normal finding. The presence or absence of peritonitis cannot be determined with this radiopharmaceutical, and would require other imaging, such as an In-111 leukocyte study or CT imaging of the abdomen and pelvis.
- 4. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 228. You are shown serial 3 minute posterior static images and renogram curves from a Tc-99m mercaptoacetyltriglycine (MAG3) renal scan (Figures 4A and 4B) performed in an adult with left hydronephrosis. Repeat images and curves obtained after intravenous administration of 40mg of furosemide (LasixR) are also shown (Figures 4C and 4D). Which one of the following statements is CORRECT? A. There is left ureteropelvic junction obstruction. B. There is no evidence of anatomic obstruction. C. The study is non-diagnostic because of renal insufficiency. D. 24 hour delayed images are necessary for a definitive diagnosis. FINDINGS: The baseline study demonstrates prompt MAG3 uptake and excretion by the right kidney, with minimal retention of activity within the right upper and mid-pole calyces, without calyceal dilatation. On the left, there is decreased initial tracer uptake, with prominent photopenic areas in the left renal medullary region, consistent with dilated calyceal structures, and with progressive accumulation of activity with dilated left renal calyces and a dilated left renal pelvis. There is high-grade drainage impairment noted at the left ureteropelvic junction, which persists on an upright post-void image. There is borderline asymmetry in renal function, with the left kidney providing approximately 45% of renal function. The post-diuretic study demonstrates relatively prompt clearance of remaining activity from the left renal collecting system, with a clearance half-time after furosemide administration of approximately 7 minutes, which is normal. There is no evidence of anatomic obstruction on either side. RATIONALES A. Incorrect. The baseline study is consistent with high-grade left ureteropelvic (UPJ) obstruction. However, on the diuretic portion of the study, there is prompt clearance of activity from the left renal calyces and renal pelvis, with a clearance half-time of 7 minutes, which is normal (normal < 10 minutes). Based on these results, there is no evidence of significant anatomic obstruction, and the findings are consistent with dilatation of the left renal collecting system without obstruction. B. Correct. See discussion in A above. C. Incorrect. If there is renal insufficiency, then the diuretic study may produce a false- positive result for obstruction, because the affected kidney(s) may be unable to respond to the loop-acting diuretic. Renal insufficiency would not produce a false negative result (ie. apparent non-obstruction in the face of significant anatomic obstruction). Furthermore, there is only mild impairment in left renal function, with normal right renal function in this case, thus this option is not a plausible explanation for the findings demonstrated.
- 5. 2007 ACR Diagnostic Radiology In-Training Exam Rationales D. Incorrect. The diagnosis of a dilated, non-obstructed left renal collecting system can be made on the basis of the available images alone, as discussed above, without the need for further delayed views, which would add nothing to the diagnosis in this case. 229. You are shown multiple static images from a Tc-99m macroaggregated albumin (MAA) pulmonary perfusion scintigram (Figure 5). What is the MOST LIKELY explanation for the image findings? A. Tc-99m sulfur colloid was injected instead of Tc-99m MAA. B. There is significant alumina breakthrough in the radiopharmaceutical. C. Blood clot was introduced into the syringe during radiopharmaceutical injection. D. The patient has multiple pulmonary arteriovenous malformations. FINDINGS: There are focal areas of increased tracer uptake noted in the left mid-lung field, near the left major fissure, and also in right middle lobe. There are no significant perfusion defects demonstrated. RATIONALES A. Incorrect. If sulfur colloid were injected instead of MAA, then the biodistribution of the tracer would follow that of the smaller sulfur colloid particles, resulting in uptake within the liver, spleen and bone marrow, without significant pulmonary uptake. Focal areas of increased activity within the lungs would not result. B. Incorrect. Alumina breakthrough can result in particle formation in a non-particulate radiopharmaceutical or formation of larger particles in a particulate radiopharmaceutical. For example, excessive alumina breakthrough can result in significant pulmonary uptake on a sulfur colloid liver-spleen scan. However, alumina breakthrough is unlikely to produce particles sizes large enough to result in the focal “hot spot” artifacts noted in this case. The findings in the present case are much more commonly produced via the mechanisms discussed below, namely, aggregation of MAA particles secondary to formation of blood clots in the syringe or from settling of the suspended particles (see C below). C. Correct. The focal areas of increased tracer uptake demonstrated in the left mid- lung field, near the major fissure, and in the right middle lobe are consistent with focal areas of aggregation of the MAA particles, most likely due either to introduction of blood into the radiopharmaceutical syringe during injection (ie., drawing blood into the syringe) or failure to properly suspend the particles or re-suspend them, if the syringe had been left sitting in the radiopharmacy for a long period of time prior to injection. D. Incorrect. The findings in this case are consistent with a radiopharmaceutical artifact, as discussed above. Furthermore, pulmonary arteriovenous malformations (AVMs), when large enough to resolve, would present as focal areas of decreased tracer uptake, secondary to shunting of blood via the AVMs
- 6. 2007 ACR Diagnostic Radiology In-Training Exam Rationales from the venous to arterial circulation, bypassing the pulmonary capillary bed, and thus not trapped within it. Therefore, the presence of multiple pulmonary AVMs is not a viable explanation for the findings in this case. 230. You are shown maximum intensity projection (MIPS) coronal, transaxial and sagittal F-18-fluorodeoxyglucose (FDG) PET images obtained in an adult patient (Figure 6). What is the MOST LIKELY diagnosis? A. Bronchogenic carcinoma B. Breast carcinoma C. Hodgkin’s Disease D. Malignant melanoma FINDINGS : There are numerous focal areas of increased tracer uptake noted in the chest, abdomen and pelvis, many of which are clearly located in the subcutaneous tissues of the abdominal wall and chest wall, best seen on the selected transaxial and sagittal images provided. RATIONALES A. Incorrect. While several of the lesions demonstrated do project over the lung fields on the MIPS image, the sagittal image demonstrates that at least several are located in the soft tissues of the posterior chest wall, rather than in the lungs. In addition, there is no single dominant lesion that appears to be within a lung. While not excluded, bronchogenic carcinoma is a less likely etiology for these findings than melanoma. B. Incorrect. As discussed in A above, the predominance of subcutaneous lesions is less characteristic of metastatic breast carcinoma than of melanoma. There is no lesion demonstrated in the breast, and there is also no evidence of axillary adenopathy or hepatic metastases, which would also commonly occur in metastatic breast carcinoma. Therefore, while not excluded, metastatic breast carcinoma is a less likely etiology for the findings than melanoma. C. Incorrect. As discussed above, the pattern of subcutaneous lesions is more characteristic of melanoma than lymphoma, particularly in the absence of significant lymph node involvement. While some non-Hodgkin’s lymphomas may primarily involve the skin, this pattern of involvement is not common in Hodgkin’s disease. D. Correct. Metastatic malignant melanoma is the most likely diagnosis. The pattern of extensive, markedly hypermetabolic lesions in the subcutaneous soft tissues is most characteristic of metastatic malignant melanoma.
- 7. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 231. Which of the following statements about Y-90-ibritumomab tiuxetan (ZevalinR) radioimmunotherapy (RIT) for indolent non-Hodgkin’s lymphoma is TRUE? A. It targets CD-15 receptors on immature B cells. B. Tc-99m labeled ZevalinR is used for imaging prior to therapy. C. Unlabeled rituximab (RituxanR) must be intravenously infused before therapy. D. Bone marrow involvement of less than or equal to 50% is a prerequisite. RATIONALES: A. INCORRECT. Y-90 ZevalinR targets CD-20 receptors on mature B-cells. B. INCORRECT. Pre-RIT imaging is performed using In-111 labeled ZevalinR. ZevalinR is not available labeled with Tc-99m. C. CORRECT. Rituximab is given prior to administration of Y-90 ZevalinR to deplete binding sites on circulating B-cells, which would otherwise bind to the radiopharmaceutical and reduce the effectiveness of the RIT. D. Bone marrow involvement must be less than 25%, not 50%. References: Biodistribution and dosimetry results from a phase III prospectively randomized controlled trial of Zevalin radioimmunotherapy for low-grade, follicular, or transformed B-cell non-Hodgkin's lymphoma. Crit Rev Oncol Hematol. 2001 Jul- Aug;39(1-2):181-94.PMID: 11418315
- 8. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 232. Which of the following statements regarding F-18-fluorodeoxyglucose PET imaging in lymphoma is TRUE? A. It has the same sensitivity for the detection of Hodgkin’s disease and non- Hodgkin’s lymphoma. B. Higher standardized uptake values are associated with mucosa-associated lymphoid tumor (MALT) lymphoma than with other cell types. C. It can be used to assess the effectiveness of chemotherapy after as few as two treatment cycles. D. While it is more sensitive than Ga-67 citrate imaging for the primary staging of lymphoma, it is less sensitive for the detection of recurrent disease. RATIONALES: A. INCORRECT. While both Hodgkin’s disease (HD) and non-Hodgkin’s lymphoma (NHL) are accurately assessed using F-18 FDG PET, HD has significantly higher sensitivity and specificity than NHL overall. This difference is due to the fact that low-grade NHLs demonstrate lower FDG uptake. B. INCORRECT. In one study of 10 patients, MALT lymphoma did not reveal any significant F-18 FDG uptake. While other studies have produced variable results, nevertheless, the FDG avidity for MALT lymphomas is overall significantly lower than for many other cell types. C. CORRECT. FDG PET can be used with high positive predictive value to assess the response to chemotherapy, even after only one or two cycles of treatment. D. INCORRECT. FDG PET has been demonstrated to be more sensitive than Ga-67 citrate scintigraphy for the diagnosis, staging and re-staging of both HD and NHL. References: Israel O, Keidar Z, Bar-Shalom R. Positron Emission Tomography in the Evaluation of Lymphoma. Semin Nucl Med 34:166-179, 2004.
- 9. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 233. Which of the following is the MOST appropriate pharmacologic stress agent for patients undergoing myocardial perfusion imaging who have severe bronchospasm? A. Dypyridamole B. Adenosine C. Dobutamine D. Aminophylline RATIONALES: A. Incorrect: Dypyridamole is a commonly used agent for pharmacologic stress in conjunction with myocardial perfusion imaging. It inhibits reabsorption of adenosine back into the myocytes, increasing blood and tissue levels of adenosine. Dipyridamole and adenosine increase coronary blood flow 3-4 times in normal vessels, but stenosed vessels are unable to respond, resulting in a relative “steal” phenomenon, unmasking areas of myocardial ischemia. However, both dypyridamole and adenosine are contraindicated in those patients with known severe bronchospasm, as they can trigger further bronchospasm. B. Incorrect: See rationale for item A above. Adenosine does increase coronary blood flow, but is also contraindicated in patients with severe bronchospasm, asthma or wheezing. C. Correct: Dobutamine has major B1 agonist properties and only mild (not clinically significant) B2 properties. It also has Alpha 1 agonist properties. It increases both the inotropic and chronotropic action of the heart. It is appropriately employed in those patients who cannot perform exercise or those with contraindications to adenosine and dypyridamole (eg., because of bronchospastic pulmonary disease) or in patients who recently received xanthine derivatives or have ingested caffeine within 24 hours of the study. D. Incorrect: Aminophylline and other xanthines block adenosine receptors. It is not a cardiac pharmaceutical stress agent. This is why intake of xanthines is contraindicated at least 24 hours before an adenosine or dypyridamole pharmacologic stress myocardial perfusion imaging study. Aminophylline is used to prevent and treat wheezing, shortness of breath, and difficulty breathing caused by asthma, chronic bronchitis, emphysema, and other lung diseases. Furthermore, it is used as an antidote in patients developing adverse reactions during dipyridamole infusion studies. References: Sandler, Diagnostic Nuclear Medicine. 4rth Ed. Lippincott Williams & Wilkins, Philadelphia, PA. 2003.Williams, Scott. Aunt Minnie.com (Reference: Nuclear Medicine). 10September 2005 Update
- 10. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 234. Analysis of an equilibrium multigated-acquisition (MUGA) radionuclide cardiac study is performed, with the background region of interest placed over the spleen. The resulting calculated left ventricular ejection fraction will be: A. Artifactually reduced. B. Artifactually elevated. C. Unchanged. D. Variably affected. RATIONALES: A. Incorrect. Selection of a non-representative high count region of interest for the background region will result in an artifactual increase in the ejection fraction calculation, not a decrease. B. Correct. In the formula for calculation of the ejection fraction, the background counts in the numerator cancel out by subtraction, with the resultant formula for the ejection fraction being: (ED counts – ES counts) / (ED counts – Bkgd counts). Thus, placement of the background region of interest in an unrepresentative area of high counts, such as the splenic blood pool, will artifactually decrease of the denominator’s value in the equation. This relative decrease in the denominator’s value will result in a spurious elevation of the calculated ejection fraction. Typically, a crescentic background region of interest with average of 2 to 3 pixel width is drawn adjacent to the lateral aspect of the left ventricle. C. Incorrect. See B above. D. Incorrect. See B above. References: Http://www.auntminne.com/index.asp?sec=ref&sub=ncm&pag=car&itemid=5507 3 Sandler, Diagnostic Nuclear Medicine. 4rth Ed. Lippincott Williams & Wilkins, Philadelphia, PA. 2003
- 11. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 235. Which of the following statements about agreement states is CORRECT? A. They are states that agree to allow the Nuclear Regulatory Commission (NRC) to regulate radioactive by product material within their boundaries. B. They are states that agree to regulate radioactive by product material within their borders on behalf of the NRC. C. They are permitted to have less stringent regulations than the NRC. D. A state can become an agreement state without prior notification of the NRC. RATIONALES: A. Incorrect. Agreement states regulate by-product material within their borders in place of the NRC. B. Correct C. Incorrect. Regulations in agreement states must be as stringent as NRC regulations, and can be more stringent. D. Incorrect. Agreement states must demonstrate to the NRC that they have the capabilities to assume the NRC's mission within their boundaries, and that the intended regulations are consistent with NRC rules and regulations and are as strict or more so. References: Code of Federal Regulations Wilson, Michael A., editor, Textbook of Nuclear Medicine. Lippincott-Raven, Philadelphia, PA, 1998.
- 12. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 236. In nuclear medicine, what is the primary benefit for the use of a narrow energy window? A. Enhances count rate B. Reduces dead time losses C. Diminishes background radiation in image D. Reduces scatter radiation in image RATIONALES: A. Incorrect. A narrow window would reduce the image count rate. B. Incorrect. While the count rate for generating the image would be reduced, the actual detected photon count rate would not be changed and the dead time losses would not be reduced. C. Incorrect. Background radiation counts would be reduced, but this is a minor component compared with the scatter radiation coming from the patient. D. Correct. Gamma rays are emitted at very specific energies. If the detected photon has a lower energy, it may be assumed that the photon was from a Compton scatter interaction and is not coming directly from the location of the radionuclide tracer. 237. What is the maximum allowable total effective dose equivalent annual occupational radiation exposure for an adult? A. 5 mrem (0.05 mSv) B. 5 rem (0.05 Sv) C. 500 rem (5 Sv) D. 5000 rem (50 Sv) RATIONALES: A, C & D.. Incorrect. Total annual limit for occupational exposure is 5 rem (5,000 mrem or 0.05 Sv or 50 mSv). B. Correct. Reference: Code of Federal Regulations 10 CFR 20 Subpart C 20.1201, (a), (1), (i).
- 13. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 238. What is the critical organ for myocardial perfusion imaging using Tl-201 chloride? A. Gallbladder wall B. Upper large intestines C. Kidneys D. Urinary bladder RATIONALES: A. Incorrect. The gallbladder wall is the critical organ for Tc-99m tetrofosmin (MyoviewR) myocardial perfusion imaging, not for Tl-201 scintigraphy. B. Incorrect. The upper large intestines/colon is the critical organ for Tc-99m sestamibi (CardioliteR) and Tc-99m teboroxine (CardiotecR). C. Correct. The kidney is the critical organ for Tl-201 scintigraphy, receiving 5.1 rem from a typical 3 mCi dose of Tl-201. D. Incorrect. The urinary bladder is the critical organ for Tc-99m methylene diphosphonate bone scintigraphy. REFERENCES: DePuey EG, Garcia EV, Berman DS 2001 Cardiac SPECT Imaging 2nd ed., Lippincott Williams & Wilkins, Philadelphia, p. 118. Mettler FA, Guiberteau MJ 2006 Essentials of Nuclear Medicine Imaging 5th ed., Saunders, Philadelphia, p. 105-107.
- 14. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 239. Which of the following factors contributes MOST to the specificity of Tc-99m sestamibi scintigraphy for the detection of parathyroid adenomas? A. Size of the parathyroid adenoma B. Greater hypercellularity of parathyroid adenomas compared to thyroid adenomas C. Greater avidity of the radiopharmaceutical for parathyroid tissue than for thyroid tissue D. Longer retention of the tracer in parathyroid tissue than in thyroid tissue RATIONALES: A. Incorrect. Size of the adenoma affects sensitivity, not specificity. Parathyroid adenomas must attain a size greater than ~500mg to be generally detectable, although this is usually the threshold at which they are clinically (not chemically) manifest. B. Incorrect. This is frequently untrue and unrelated. C. Incorrect. There is no in vitro evidence supporting this statement. D. Correct. Slow Tc-99m sestamibi wash-out is the hallmark of a parathyroid adenoma (or carcinoma) This phenomenon is specific for hypercellular parathyroid neoplasms and is not a characteristic of thyroid neoplasms. Reference: Taillefer R., Boucher Y., et al. Detection and localization of parathyroid adenomas in patients with hyperthyroidism using a single radionodule imaging procedure with technetion 99m – sestamibi (double-phase study). J. Nuclear Med. 1992; 33: 1801 – 1807.
- 15. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 240. Which of the following statements about the clinical evaluation of bone mineral density using dual-energy x-ray absorptiometry (DEXA) and dual-photon absorptiometry (DPA) is TRUE? A. An advantage of DEXA over DPA is significantly reduced radiation exposure to patients. B. An advantage of DPA over DEXA is the ability to correct for soft tissue attenuation. C. The World Health Organization (WHO) criteria for the assessment of osteopenia and osteoporosis were developed using the DEXA technique. D. The radius (forearm) cannot be evaluated using either technique. RATIONALES A. Incorrect. There is no significant difference in radiation exposure between DEXA and DPA techniques, and given the higher photon flux, DEXA may result in a slightly higher exposure than DPA. B. Incorrect. Soft tissue attenuation correction is needed for accurate density measurement of bony structures such as the spine or hip. This is accomplished with dual-energy techniques by assessing the differential attenuation of photons by bone vs. soft tissue at different energies. Both DPA and DEXA are dual- energy techniques that allow for such attenuation correction. C. Correct. The WHO criteria were developed based on the DEXA technique. D. Incorrect. The distal radius and/or ulna can be evaluated either by DPA or DEXA techniques. Previously, the radius was also evaluated using I-125 absorptiometry. REFERENCES:Zeissman HA, O’Malley JP, Thrall JH: Nuclear Medicine-The Requisites. 3rd ed. Mosby. 2006.
- 16. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 241. Regarding bone scintigraphy in the evaluation of malignancy, which of the following is TRUE? A. A solitary “hot” lesion in the sternum of a patient with breast cancer has approximately a 75% likelihood of being malignant. B. Bone metastases are present in approximately 20% of patients with prostate cancer and a prostate specific antigen (PSA) of <10 ng/mL. C. The “flare” phenomenon can be excluded as the cause for interval worsening of a bone scan in patients experiencing worsening of bone pain. D. The role of bone scintigraphy in the evaluation of primary bone malignancy is the pre-operative assessment of the extent of the primary tumor. RATIONALES: A. Correct. Based on a study by Kwai et al published in 1988. Lesions in the sternum in breast carcinoma may be secondary either to hematogenous spread or direct extension of tumor. B. Incorrect. In this setting, the incidence of bone metastases is less than 1%. C. Incorrect. The paradoxical worsening of the bone scan with the “flare” phenomenon may also be accompanied by a worsening of bone pain as well as increasing sclerosis on radiographs. The radiographic finding of sclerotic healing of lesions and the time course following chemotherapy are better clues as to the presence of a flare phenomenon. For this reason, follow-up bone scintigraphy in patients with skeletal metastases is most often performed no sooner than 3 months and typically at 6-12 months or later. D. Incorrect. Bone scintigraphy does not reliably determine the extent of primary bone malignancies, and may overestimate the extent of involvement. Assessment of the extent of the primary lesion is better accomplished with MRI and plain radiographs. Bone scintigraphy is useful as a whole body survey to assess for additional sites of involvement (metastatic or multicentric disease). REFERENCES: Murray IPC, Ell PJ. Nuclear Medicine in clinical diagnosis and Treatment. 2nd ed. Churchill Livingstone. 1998. Zeissman HA, O’Malley JP, Thrall JH: Nuclear Medicine-The Requisites. 3rd ed. Mosby. 2006.
- 17. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 242. An 8-year-old patient with suspected lower extremity osteomyelitis presents with normal plain radiographs. Which one of the following is the MOST appropriate next imaging study? A. Tc-99m methylene diphosphonate (MDP) three-phase bone scintigraphy B. Ga-67 citrate scintigraphy C. In-111-labeled WBC scintigraphy D. Tc-99m sulfur colloid bone marrow scintigraphy RATIONALES: A. Correct. A three-phase bone scan is almost always a good choice for the initial evaluation of possible osteomyelitis, especially if the plain radiographs are normal (and there is no other underlying bone pathology which would be likely to cause increased bone uptake of the tracer and limit the usefulness of the exam). It is both highly sensitive and has a very high negative predictive value for osteomyelitis. The radiopharmaceutical is readily available, the exam is easily performed, and the radiation dose is lower than for Ga-67 or In-111 labeled WBC imaging. The normal increased radiopharmaceutical activity at the growth plates is a potential limitation in pediatric patients, but this would also be a limitation with Ga-67 citrate imaging. B. Incorrect. A three-phase bone scan is the most appropriate next study. In some settings, Ga-67 citrate may be used in addition to bone scan to improve diagnostic accuracy, with the gallium scan performed after the bone scan. C. Incorrect. In-111 WBCs are generally avoided in pediatric patients if there is a good alternative, because of the high radiation-absorbed dose to the spleen. A three-phase bone scan is a better choice. D. Incorrect. A bone marrow scan can be used in conjunction with radiolabelled WBC imaging to improve diagnostic accuracy in the evaluation of osteomyelitis, but it has no role as an initial imaging agent in this setting. REFERENCES: Zeissman HA, O’Malley JP, Thrall JH: Nuclear Medicine-The Requisites. 3rd ed. Mosby. 2006. Treves, ST: Pediatric Nuclear Medicine. 2nd ed. Springer-Verlag. 1995.
- 18. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 243. Which one of the following is MOST LIKELY to produce a whole-lung ventilation-perfusion (V/Q) mismatch on a ventilation-perfusion lung scan? A. Swyer-James Syndrome B. Fibrosing mediastinitis C. Foreign body in a mainstem bronchus D. Mucous plugging RATIONALES A. Incorrect. Swyer-James Syndrome is characterized by bronchiolitis obliterans, a primary ventilatory disorder, which produces a whole-lung matching abnormality on the V/Q scan. B. Correct. This condition is associated with vascular compression or compromise, without airway involvement, which can produce a whole-lung V/Q mismatch, mimicking the presence of massive pulmonary embolism involving the ipsilateral main pulmonary artery. C. Incorrect. A foreign body produces a primary central airway obstruction, resulting in a large ventilation defect, possibly involving the entire lung, if located in a mainstem bronchus. There may be secondary diffuse hypoperfusion resulting from reflex vasoconstriction, producing matching findings, but a V/Q mismatch (ie., abnormal perfusion with normal ventilation) would not occur. D. Incorrect. The pathophysiology of mucous plugging is the same as for a foreign body (see C above), and may involve either selected segments, an entire lung or portions of both lungs. Again, this is a primary ventilatory disorder, and V/Q mismatch would not be observed. References: Mettler FA and Guiberteau MJ: Essentials of Nuclear Medicine Imaging, 5th ed., Saunders Elsevier, Philadelphia, pp. 187-194.
- 19. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 244. What type of radiation is detected in a positron emission tomography (PET) scan? A. Beta radiation B. Two photons detected in coincidence C. Two positrons detected in coincidence D. A positron and an electron detected in coincidence RATIONALES: A. Incorrect. B. Correct. In PET scanning a positron emitted by radioactive nucleus, travels up to a few millimeters before losing all of its energy, attracts and combines with an electron, and the particles annihilate producing two 0.511 MeV photons that travel in opposite directions, which if both are detected at the same time (“in coincidence”) indicates that the decay event occurred along a line between the detectors C. Incorrect. D. Incorrect. References: The Essential Physics of Medical Imaging, 2nd edition. J.T. Bushberg, J.A. Seiabert, E.M. Leidholdt, and J.M. Boone, Lippincott Williams & Wilkins (2002), Chap 22, p720. Physics of Radiology, 2nd edition. Anthony Brinton Wolbarst, Medical Physics Publishing, Madison WI (2005), Chap 43, p446.
- 20. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 245. Instant thin-layer chromatography is used to assess what parameter of radiopharmaceutical quality assurance? A. Radionclidic purity B. Radiochemical purity C. Chemical purity D. Presence of pyrogens RATIONALES A. Incorrect. Radionclidic purity is typically evaluated by assessing for the presence of high energy contaminants by means of counting radiopharmaceutical samples in a dose calibrator, with and without lead shielding, or by using a multichannel analyzer to identify the comtaminants. B. Correct. Using different solvents, instant thin-layer chromatography can be used to assess for and quantitate the presence of free Tc-99m pertechnetate and free hydrolyzed reduced Tc-99m. In each case, the desired product radiopharmaceutical and the contaminant demonstrate disparate Rf values, when the strips are cut up and counted for radioactivity in a well counter. C. Incorrect. Chemical purity is tested using chemical test strips that change color in the presence of non-radioactive chemical contaminants, such as alumina from the Mo- 99/Tc-99m generator column or stannous ion (tin, used as a reducing agent) from the radiopharmaceutical kits. D. Incorrect. Pyrogen testing is performed using the limulus lysate test. It is not routinely performed in daily clinical Nuclear Medicine practice, but is required of radiopharmaceutical manufacturers and during the conduct of research with investigational radiopharmaceutical agents. References: Mettler FA and Guiberteau MJ: Essentials of Nuclear Medicine Imaging, 5th ed., Saunders Elsevier, Philadelphia, pp. 43-46.
- 21. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 246. Regarding hepatobiliary scintigraphy in suspected biliary atresia in the neonatal period, imaging should be carried out for at least: A. 2 hours. B. 4 hours. C. 24 hours. D. 48 hours. RATIONALES A. Incorrect. At 2 hours, biliary atresia and neonatal hepatitis may appear identical, without visualization of the biliary tree or bowel. B. Incorrect. As noted in A above, biliary atresia and neonatal hepatitis may be indistinguishable at 4 hours as well. C. Correct. In most cases, the diagnosis will be apparent by 24 hours, especially if phenobarbital was given prior to the study to enhance hepatic biliary excretion. Beyond 24 hours, radioactive decay of the Tc-99m biliary tracer will limit the resolution of images obtained. D. Incorrect. As discussed above, in most cases, the diagnosis can be made in 24 hours, and the relatively short 6 hour half-life of Tc-99m limits the utility of imaging beyond 24 hours as well. References: Mettler FA and Guiberteau MJ: Essentials of Nuclear Medicine Imaging, 5th ed., Saunders Elsevier, Philadelphia, p. 230.
- 22. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 247. Gastric emptying of which of the following is associated with an exponential pattern of gastric clearance? A. Solids only B. Liquids only C. Both solids and liquids D. Neither solids nor liquids RATIONALES A. Incorrect. Solid-phase gastric emptying studies typically demonstrate an initial lag phase followed by linear gastric emptying in normal subjects. B. Correct. Liquids follow a monoexponential pattern of gastric emptying normal. Liquid gastric emptying studies are less sensitive than solid-phase studies for the assessment of gastroparesis. C. Incorrect. As discussed above, the normal patterns of gastric emptying are an initial lag phase followed by linear emptying of solids and a monoexponential emptying of liquids. D. Incorrect. As discussed above, the normal patterns of gastric emptying are an initial lag phase followed by linear emptying of solids and a monoexponential emptying of liquids. References: Mettler FA and Guiberteau MJ: Essentials of Nuclear Medicine Imaging, 5th ed., Saunders Elsevier, Philadelphia, pp. 234-236.PEDIATRICS