2. Head & Neck (ENT) PATHOLOGY OTOLARYNGOLOGY www.freelivedoctor.com
3. Objective; Understand the common disorders of the upper airway and upper digestive tract (i.e., head and neck) in the usual context of: DEGENERATIVE, INFLAMMATORY, and NEOPLASTIC … deviations of normal anatomy and histology www.freelivedoctor.com
5. EVERYTHING that touches AIR (columnar) or FOOD (squamous) in the HEAD/NECK region ORAL CAVITY “ UPPER” RESPIRATORY TRACT EARS NOSE SALIVARY GLANDS www.freelivedoctor.com
56. The Tympanic Cavity www.freelivedoctor.com Chorda Tympani N. (CN VII) Tendon of Tensor Tympani M. (V 3 ) Incus Tendon of Stapedius M. (CN VII) Stapes Cut edge of tympanum Malleus
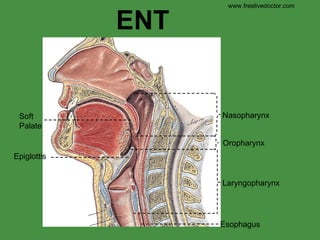
The “realm” of “ENT”, or otolaryngology, includes diseases of the nose, nasal cavity, nasopharynx, oral cavity, oropharynx, larynx, laryngopharynx, “upper” airway, defined as airspaces leading ultimately into the lung, and all the structures in these spaces, such as the for pairs of nasal sinuses, auditory tubes, ears, nasolacrimal duct, tonsils, and salivary glands. ENT docs do thyroid surgery too.
Once again, amid the numerous brilliant adjectives one can place before the word “diseases”, from a solid anatomical point of view, the classifications of DEGENERATIVE, INFLAMMATORY, and NEOPLASTIC cover almost all basis, and is a good way to think of disease classifications of any organ or system.
This will be an amazingly fun and GRAPHIC chapter
Because a tougher stratified squamous mucosa is needed when these spaces come into contact with particulate matter, or material other than air or water, this type of mucosa, no matter where it is in the ENT domain, behaves similarly to degenerative, inflammatory, and neoplastic influences. Similarly, upper “airway” mucosa, classically subject only to air contact, is pseudostratified ciliated columnar in histology, and behaves similarly to these three influences as well. Upper airway mucosa, however, often transforms into stratified squamous by a process called “squamous metaplasia” as a non specific response to a wide variety of injurious stimuli.
Which of these spaces come into contact with only air? If you guessed that that space would be lined by a columnar epithelium (pseudostratified, often ciliated, columnar epithelium). You guessed right!
Common pathologic conditions of the oral cavity
What is “upper” airway defined as? If this area was infected, would it be called an “upper” respiratory infection? Would you expect that if parts of an upper airway were lined by the same types of epithelium then they might be subject to the same types of inflammations and neoplasms? Answer: YES
Common pathologic conditions of the “neck” itself.
Common pathologic conditions of the “non-accessory” salivary glands, i.e., submandibular (mixed), parotid (99% serous), sunlingual (99% mucinous).
Find the “cavity”, i.e., caries, i.e., enamel erosion.
The main predecessor to “peridontal”, i.e., structures surrounding teeth, is gingivitis, largely caused by actinoobacilli, porphyromonas, and prevotella species, although more than 300 types of bacteria are known to commonly hang out in the mouth.
Inflammatory endpoint or true neoplasm? Who cares? Often the terms “inflammatory” or “reactive” refers to this type of “fibroma”.
Granuloma or neoplasm or granulation tissue? Who cares? A pyogenic granuloma pops out like a “tumor” and is 100% indistinguishable from normal granulation tissue, and looks nice and pink and healthy like granulation tissue, i.e., organizing inflammation, too. The least thing it can be called is a granuloma, because it rarely has clusters of macrophages or giant cells. Would you expect a pyogenic granuloma to “blanch” and a fibroma NOT to “blanch”? Answer: YES
Obscure etiology, 40% of us have had them, painful, and you can bet there are inflammatory cells at the base. You know what they are. You’ve had them. Things related to them include: stress , fatigue , illness , injury from accidental biting , hormonal changes, menstruation , sudden weight loss , food allergies , and deficiencies in vitamin B12 , iron , and folic acid (wikipedia). Whenever a condition is associated with LOTS of things, like this, we call this an “obscure” etiology ;)
Glossitis: Bacterial or viral infections (including oral herpes simplex ). Mechanical irritation or injury from burns, rough edges of teeth or dental appliances, or other trauma Exposure to irritants such as tobacco , alcohol , hot foods, or spices . Allergic reaction to toothpaste, mouthwash, breath fresheners, dyes in candy, plastic in dentures or retainers, or certain blood-pressure medications (ACE inhibitors). Disorders such as iron deficiency anemia , pernicious anemia and other B-vitamin deficiencies, oral lichen planus , erythema multiforme , aphthous ulcer , pemphigus vulgaris, syphilis , and others. Occasionally, glossitis can be inherited. (Wikipedia) If a “geographic” tongue mans only a part of the tongue is inflamed, i.e., “red”, then the tongue on the right has the geography of Maine or Illinois? Or India?
Herpetology is the study of creepy critters, reptiles and amphibians. Herpetic vesicles “creep” over mucosal surfaces. Like CMV and V-Z viruses, the various herpes viruses (mainly type 1 and 2) are, amazingly, in the “herpes” family of viruses. Early lesions crop up as vesicles, after a few days, these vesicles can be irritated, ulcerated, inflamed, and secondarily pustulated. Classically type 1 was predominantly oral mucosa, and the slightly nastier type 2 was more genital, but nowadays, crossover is so common, who cares any more? The virus recurs often for many years, triggered off by god-knows-what, and the newer antiviral agents have shown amazing efficacy in preventing recurrences. Just about everybody had been exposed to herpes of some type.
Herpes, dried vesicle with inflammation
Herpes, dried vesicle with ulceration and secondary inflammation. Acute or chronic?
The neat thing about a Tzanck smear is that you can do it easily in your office, just gently scrape a vesicle, smear it, stain it with just about anything, and look for much larger than usual squamous nuclei with inclusions. Most vesicles cause by herpes family viruses can have a POSITIVE Tzanck (pronounced “zank”) smear, or test. Would you rule out herpes if the test was negative? Would you tend to be more likely to rule it in, if the smear was positive?
Monilia, thrush-mouth, candida: they all mean the same thing. Look for a whitish oral film without much underlying inflammation (i.e., redness). Common in babies, diabetics, immunocompromised people. Candida (almost always ablicans) always affects moist, usually non-keratinized, stratified squamous mucosa, i.e., mouth, vagina, moist genital skin areas. Everybody has it lying around waiting for an immunocompromised condition to occur.
White filmy patches NOT firmly attached to the underlying moist non-keratinized stratified squamous mucosa. Minimal redness. Candida is on all of us. It LOVES to proliferate on moist NON-keratinized stratifies squamous mucosae, especially in immune deficiency situations.
Like the Tzanck test, finding the NON-septate hyphae (i.e., “pseudo”-hyphae) along with yeasts and budding yeasts in your simple office lab, is diagnostic. Almost any simple stain will show this. The “PAS” stain is best, because it imparts a bright red color to yeasts and pseuduhyphae, relative to all the other squamous and inflammatory and blood junk around it.
LEUKOPLAKIA. This is defined as a dry flat “plaque” of, usually, the oral mucosa, due to ANY reason, many (most?) of which are NON-malignant, NON-dysplastic, and 100% reversible, but some of which are premalignant. Please understand “leukoplakia” is a clinical description, and NOT a specific clinical or pathological entity, and can range anywhere between hyperkeratosis/inflammation to carcinoma.
“ Hairy” leukoplakia however, is usually a sign of HIV.
“ Hairy” leukoplakia however, is usually a sign of HIV.
EXTREMELY IMPORTANT concept in the insidious development of squamous cell carcinoma of ANY location, no matter what the genetics, molecular biology, or etiology is! UNDERSTAND THIS FOR THE REST OF YOUR LIFE!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
Does this look like more than a simple “plaque”? Like, perhaps, ulceration and induration under the ulcer bed. This is a classic appearance of INFILTRATING or INFILTRATIVE SQUAMOUS CELL CARCINOMA of the mouth. Can there be any other type? Where would you take the biopsy?
Well, moderate, poor. These are the 3 types of differentiation of squamous cell cancer, no matter what the current trendy buzz words or grading letters/numbers are!!! In “well” you can see “pearls”. This is a pearl above. In “moderate”, you can usually see “intercellular bridges”, but not pearls. In “poor” you usually have no real idea that it even looks squamous at all, and you have to rely on squamous or immunochemical markers, such as cytokeratin markers, or a whole host of others.
As a rule of thumb, all cysts submitted by oral surgeons are benign. Many types often recur however. It is only a question of whether the cyst is “developmental”, i.e., an abnormal development, ultimately from embryology, or “inflammatory” in etiology. IMHO, learning the names of all the many different types, is idiotic. Both developmental and inflammatory cysts develop from remnants of odontogenic epithelium, i.e., the epithelium which gives rise to teeth.
Classical radiologic and histologic image of a dentigerous cyst.
These conditions cover 99% of what might appear as a tumor or bump in the nose, nasal, cavity, or nasal pharynx, and simple ”polyps”, also called “Inflammatory polyps” are the vast majority
Not only are inflammatory “polyps” associated with inflammation of their mucosa of origin, but they show inflammatory changes in them!
Multiple appearances of nasal polyps
These are two very serious, i.e., potentially and often fatal aggressive granulomatous proliferations of the upper airway. They are often hard to distinguish from each other clinically and even histologically. “Lethal” midline granuloma is thought to be a malignant tumor of NK (Natural Killer) cells.
Papilloma and “inverting” or “inverted” papilloma of upper airways.
Where is the “angio” part? Where is the “fibroma” part?
All plasmacytomas are proliferations of plasma cells, which often look classically like normal plasma cells. Name the 4 features of “normal” plasma cells. Do you remember that many of these, perhaps ALL, with time, will become multiple myelomas and express a monoclonal gammopathy?
Esthesioneuroblastomas of the olfactory nerve (really bulb or tract) are exceedingly rare. This will probably be the only one you will ever see. Like any other neuroblastoma, it may have “rosettes”.
Nasopharyngeal carcinomas almost always look like they are half carcinoma and half lymphoma. Draw a line which separates an “epithelial” looking part of the tumor from a “lymphoid” appearing part
World’s most normal vocal cords.
What are the 4 cardinal signs of acute –itis?
Polyp, or “singer’s” nodule. If I gave you a list of all the famous pop singers that had these nodules, you would be amazed. (Try Wiki)
Papilloma, but there may be some cancer microscopically.
Carcinomas are usually ulcerated, irregular, indurated, invasive, and destructive, with secondary necrosis. For all practical purposes regard them all as squamous.
What are those huge cells under the stratified squamous mucosa? Cancer cells, i.e.’, malignant invasive squamous cells. Are they invasive? Of course, otherwise the would not be UNDER the mucosa, would they?
Otitis externa
World’s most normal tympanic membrane.
Acute middle ear infection
Chronic “serous” otitis media
Cerumen impaction, probably the most common ear abnormality and/or cause of decreased hearing.
Otosclerosis, abnormal bone deposition between the footplate of the stapes and oval window, one of the commonest forms of conduction hearing loss, begins in middle age, get progressive, usually bilateral, often familial.
Tumors of the carotid body are composed of “balls of cells”, or “zell-ballen” in German. There is an infinitely confusing relationship to the terms paragangliomas, glomus tumors, chemodectomas, with respect to carotid body tumors. For purposes of sanity we will say, carotid body tumors ore tumors of the carotid body receptor cells which are cells near the carotid sinus that are sensitive to pO2, pCO2, pH, and even temperature, and are called carotid body tumors, and appear as little round balls microscopically. Pathologists have spent their whole life being confused about the proper nomenclature of these tumors with respect to the other mentioned terms, so I am not going to propagate the confusion more.
Squamous metaplasia of an interlobular duct is a very common finding in chronic sialadenitis or any duct injury.
Mucocele of an accessory salivary gland duct, just a big cyst filled with mucin and lined by mucinous columnar epithelium, often inflamed and/or squamous metaplastic
The classic place for ANY visible parotid swelling or tumor to present, between the tip of the ear and the tip (angle) of the mandible.
Viral parotitis, i.e., mumps
Remember the two commonest benign tumors and the two commonest malignant tumors of the salivary glands.
Mixed tumors are generally benign, have BOTH connective tissue (i.e., usually cartilagenous) components as well as glandular components, hence the name pleomorphic or mixed, they generally look and feel like little round soft cartilage balls.
Why is PAPILLARY CYSTADENOMA LYMPHOMATOSUM a better name than Warthin tumor for this tumor?
Why is muco-epidermoid carcinoma a perfect name for this salivary gland malignancy?
Why is adenoid cystic carcinoma a perfect name for this salivary gland malignancy? The tumor cells characteristically along the nerve spaces, and another classical feature about this malignancy, thank God, is that it is slow slow slow growing, patients are frequently alive 20-30 years after diagnoses even with no treatment, and die from other causes.