Nursing care plans, concept map bronhial asthma
•
54 j'aime•177,528 vues

This nursing care plan addresses a 14-year-old female patient named Crystal Clear presenting with difficulty breathing and diagnosed with bronchial asthma. The plan identifies 6 problems related to ineffective airway clearance, ineffective breathing pattern, impaired gas exchange, impaired cardiopulmonary tissue perfusion, fatigue, and self-care deficit. For each problem, the plan outlines short-term and long-term objectives, interventions, rationales, and evaluations. Interventions include respiratory treatments, medication administration, oxygen supplementation, and patient/family education. The overall goal is for the patient to maintain a clear airway and normal breathing pattern while preventing potential complications.

Recommandé
Contenu connexe
Tendances
Tendances (20)
Plus de Reynel Dan
Plus de Reynel Dan (20)
Dernier
Dernier (20)
Nursing care plans, concept map bronhial asthma
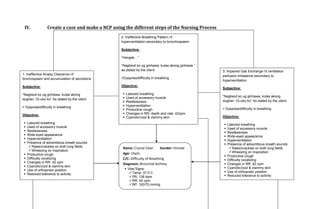
- 1. IV. Create a case and make a NCP using the different steps of the Nursing Process 2. Ineffective Breathing Pattern r/t hyperventilation secondary to bronchospasm Subjective: “Hangak…” “Naglisod ko ug ginhawa, kutas akong ginhawa.” as stated by the client. 3. Impaired Gas Exchange r/t ventilation 1. Ineffective Airway Clearance r/t perfusion imbalance secondary to brochospasm and accumulation of secretions >Dyspnea/difficulty in breathing hyperventilation Subjective: Objective: Subjective: “Naglisod ko ug ginhawa, kutas akong Labored breathing Used of accessory muscle “Naglisod ko ug ginhawa, kutas akong dughan. Gi-ubo ko” As stated by the client. dughan. Gi-ubo ko” As stated by the client. Restlessness > Dyspnea/difficulty in breathing Hyperventilation Productive cough > Dyspnea/difficulty in breathing Objective: Changes in RR, depth and rate: 42cpm Cyanotic/cool & clammy skin Objective: Labored breathing Labored breathing Used of accessory muscle Used of accessory muscle Restlessness Restlessness Wide-eyed appearance Wide-eyed appearance Hyperventilation Hyperventilation Presence of adventitious breath sounds: Presence of adventitious breath sounds: Rales/crackles on both lung fields Name: Crystal Clear Gender: Female Rales/crackles on both lung fields Wheezing on inspiration Wheezing on inspiration Productive cough Age: 14y/o Productive cough Difficulty vocalizing C/C: Difficulty of Breathing Difficulty vocalizing Changes in RR: 42 cpm Diagnosis: Bronchial Asthma Changes in RR: 42 cpm Cyanotic/cool & clammy skin Cyanotic/cool & clammy skin Use of orthopneic position Vital Signs: Temp: 37.0 C Use of orthopneic position Reduced tolerance to activity Reduced tolerance to activity PR: 136 bpm RR: 42 cpm BP: 100/70 mmHg
- 2. Name: Crystal Clear Gender: Female 6. Self-Care Deficit (hygiene and self- toileting) r/t general weakness secondary to Age: 14y/o 4. Impaired Cardiopulmonary Tissue hypoxic state C/C: Difficulty of Breathing Perfusion r/t alteration in gas exchange Diagnosis: Bronchial Asthma secondary to bronchospasm Subjective: Vital Signs: Temp: 37.0 C Subjective: “Hangak…” as stated by the client. PR: 136 bpm RR: 42 cpm “Naglisod ko ug ginhawa, kutas akong “Maglisod man gyud ni siya ug lihok-lihok kay BP: 100/70 mmHg ginhawa.” as stated by the client. naglisod siya ug ginhawa, ako na lang siyang tabangan.” as stated by SO. >Dyspnea/difficulty in breathing > Dyspnea/difficulty in breathing Objective: Objective: Labored breathing 5. Fatigue r/t poor physical condition Used of accessory muscle Labored breathing Restlessness Used of accessory muscle secondary to generalized weakness due to Hyperventilation Restlessness/confusion hypoxic states Fluctuating Oxygen Saturation: <90% Wide-eyed appearance (without Oxygen), >90% (with oxygen Hyperventilation Subjective: supplementation) Inability to perform activities such as Changes in RR, depth and rate: 42cpm bathing and tooth brushing “Kapoy man magsige ug lihok”, as verbalized Cyanotic/cool & clammy skin Weakened state by patient. Pallor Unable to go to CR > Dyspnea/difficulty in breathing Objective: Labored breathing Hyperventilation Changes in RR, depth and rate Cyanotic/cool & clammy skin Apprehension Weak appearance Drowsy Unable to perform activities
- 3. NURSING CARE PLAN Identified Problem: Patient reports difficulty in breathing with cough Nursing Diagnosis: Ineffective Airway Clearance r/t brochospasm and accumulation of secretions CUES OBJECTIVES INTERVENTIONS RATIONALE EVALUATION Subjective: Short Term Objective: Independent: STO: Within 8 hours of nursing Auscultated breath sounds. Noted Bronchospasm is present with obstruction Outcome Partially Met: “Naglisod ko ug ginhawa, care, the patient will be adventitious breath sounds. in airway and may/may not be manifested After the 8 hours of kutas akong dughan. Gi-ubo able to expectorate with adventitious breath sounds. nursing care, the patient ko” As stated by the client. secretions readily and was able to expectorate demonstrate reduction of Assessed and monitored respiratory Respirations may be shallow and rapid, secretions, partially > Dyspnea/difficulty in congestion as evi-denced rate. with prolonged expiration in comparison to relieved of congestion as breathing by noiseless respiration, inspiration. Tachypnea may be present. evidenced by improved reduction of adventitious oxygen exchange breath sounds, & Assisted patient to assume position Elevation of HOB facilitates respiratory (absence of cyanosis, Objective: improved oxygen of comfort (moderate high-back function by use of gravity, decreasing oxygen saturation > Labored breathing exchange (absence of rest). Changed positions every 2 pressure of diaphragm and enhancing 90%) and reduced Used of accessory muscle cyanosis, oxygen hours. ventilation of different lung segments. adventitious breath Restlessness saturation > 90%) after sounds, but still with Wide-eyed appearance providing appropriate Kept environmental pollution to a Precipitation of allergic type of respiratory increased respirations. Hyperventilation nursing care. minimum (dust, smoke, allergens) reactions that can trigger onset of acute Presence of adventitious according to individual situation. episode. breath sounds: LTO: Rales/crackles on both Long Term Objective: Taught and encourage deep- Provides patient with some means to cope Outcome Met: lung fields Within the 3-day nursing breathing and coughing exercises. with or control dyspnea and reduce air After the 3-day nursing Wheezing on inspiration care, the client will be traffic. care, the client was able Productive cough able to maintain patent to maintain patent airway Difficulty vocalizing airway with breath Increased fluid intake to 3000ml/day Hydration helps decrease the viscosity of (but with reduced breath Changes in RR sounds clear and within cardiac tolerance. secretions, facilitating expectoration. Fluids sounds) and potential Cyanotic/cool & clammy potential complications Recommended intake of fluids during meals can increase gastric compli-cations were skin are prevented between, instead of during, meals. distention and pressure on the diaphragm. prevented after Use of orthopneic position (pneumothorax, cardiac Provided warm/tepid liquids. Using warm liquids may decrease independent and Reduced tolerance to arrest, respiratory failure, bronchospasms. collaborative nursing activity etc.) after providing intervention was done. Vital Signs: appropriate nursing and Observed for signs and symptoms To identify infectious process and promote Temp: 37.0 C collaborative of infections. timely interventions. PR: 136 bpm interventions. RR: 42 cpm Collaborative: BP: 100/70 mmHg Administered medications as indicated:
- 4. > Bronchodilators: salbutamol Inhaled anticholinergic agents are considered the first-line of meds for asthma and other COPD - because they have a longer duration of action w/ less toxicity of potential. > Methylxanthine derivatives: Decreases mucosal edema and smooth aminophylline muscle spasm by indirectly increasing cyclic Adenosine Monophosphate (AMP). May reduce muscle fatigue/respiratory failure by increasing diaphragmatic contractility. > Leukotriene antagonist: Reduces leukotriene activity to limit Montelukast inflammatory response. > Antiinflammatory: budesonide Decreases local airway inflammation and edema by inhibiting effects of histamine and other mediators. > Antimicrobials: cephalosporins Antimicrobials may be indicated for control of respiratory infection/pneumonia. Enhances airflow and improve outcome. Provided supplemental Enhances expectoration of sputum, humidification: partial rebreather improve pulmonary function, and reduces mask, 6L/min; nebulization. lung volumes. Assisted in respiratory treatment: Breathing exercises help enhance diffusion; chest physiotherapy. nebulizer meds can reduce bronchospasm and stimulate expectoration. Monitored pulse oximetry, CXR. Establishes baseline for monitoring progression/regression of disease process and complications. Pulse oximetry- can detect changes in Oxygen saturation.
- 5. NURSING CARE PLAN Identified Problem: Due to the difficulty in breathing and coughing, adventitious breath sounds are determined upon auscultation in both lung fields, hypoxia is present. Nursing Diagnosis: Ineffective Breathing Pattern r/t hyperventilation secondary to bronchospasm CUES OBJECTIVES INTERVENTIONS RATIONALE EVALUATION Subjective: Short Term Objective: Independent: Short Term Objective: “Hangak…” Within the 8 hours of Auscultated breath sounds. Noted Bronchospasm is present with obstruction “Naglisod ko ug ginhawa, nursing care, the patient adventitious breath sounds. in airway and may/may not be manifested Outcome met. kutas akong ginhawa.” as will be free of cyanosis with adventitious breath sounds. Within the 8 hours of stated by the client. and other signs and nursing care, the patient symptoms of hypoxia Count patient RR in one full minute. Respirations may be shallow and rapid, was free of cyanosis and >Dyspnea/difficulty in (confusion, restlessness) with prolonged expiration in comparison to other signs and breathing after providing inspiration. Tachypnea may be present. symptoms of hypoxia appropriate nursing care. (confusion, restlessness) Assisted patient to assume position Elevation of HOB facilitates respiratory after providing Objective: of comfort (moderate high-back function by use of gravity, decreasing appropriate nursing care. Labored breathing rest). Changed positions every 2 pressure of diaphragm and enhancing Used of accessory muscle hours. ventilation of different lung segments. Restlessness Long Term Objective: Long Term Objective: Wide-eyed appearance Within the 3-day nursing Kept environmental pollution to a Precipitation of allergic type of respiratory Hyperventilation care, the client will be minimum (dust, smoke, allergens) reactions that can trigger onset of acute Outcome met Presence of adventitious able to establish and according to individual situation. episode. Within the 3-day nursing breath sounds: maintain normal or care, the client was able Rales/crackles on both effective respiratory Taught and encourage deep- Provides patient with some means to cope to establish and maintain lung fields pattern and be free of breathing and coughing exercises with or control dyspnea and reduce air normal or effective Wheezing on inspiration potential complications and use of purse-lipped breathing. traffic. respiratory pattern and Productive cough (pneumothorax, cardiac free of potential Difficulty vocalizing arrest, respiratory failure, Kept resuscitation bag at bedside. Provides adequate ventilation when patient complications Changes in RR, depth and etc.) after providing requires it. (pneumothorax, cardiac rate appropriate nursing and arrest, respiratory failure, Cyanotic/cool & clammy collaborative Observed for signs and symptoms To identify infectious process and promote etc.) after providing skin interventions. of infections. timely interventions. appropriate nursing and Use of orthopneic position collaborative Apprehension Collaborative: interventions. Reduced tolerance to Provided supplemental Enhances expectoration of sputum, activity humidification: partial rebreather improve pulmonary function, and reduces Vital Signs: mask, 6L/min; nebulization. lung volumes. Temp: 37.0 C PR: 136 bpm Monitor Arterial Blood Gases, pulse Establishes baseline for monitoring RR: 42 cpm oximetry, CXR. progression/regression of disease process
- 6. BP: 100/70 mmHg and complications. Pulse oximetry- can detect changes in Oxygen saturation. NURSING CARE PLAN Identified Problem: Due to the difficulty in breathing and coughing, adventitious breath sounds are determined upon auscultation in both lung fields, hypoxia is present. Nursing Diagnosis: Impaired Gas Exchange r/t ventilation perfusion imbalance secondary to hyperventilation CUES OBJECTIVES INTERVENTIONS RATIONALE EVALUATION Subjective: Short Term Objective: Independent: Short Term Objective: “Hangak…” Within the 8 hours of Auscultated breath sounds. Noted Bronchospasm is present with obstruction “Naglisod ko ug ginhawa, nursing care, the patient adventitious breath sounds. in airway and may/may not be manifested Outcome partially met. kutas akong ginhawa.” as will demonstrate with adventitious breath sounds. Within the 8 hours of stated by the client. improved ventilation and nursing care, the patient oxygenation as Counted patient RR in one full Respirations may be shallow and rapid, will demonstrate > Dyspnea/difficulty in evidenced by SaO2 minute. with prolonged expiration in comparison to improved ventilation and breathing >90%, respiratory rate inspiration. Tachypnea may be present. oxygenation as within 16-20 cpm, evidenced by SaO2 decreased adventitious Assessed skin and mucous Cyanosis may be peripheral ( noted in >90%, , decreased Objective: breath sounds and membrane color. nailbeds) or central (noted around lips or adventitious breath Labored breathing absence of cyanosis after earlobes). sounds and absence of Used of accessory muscle providing appropriate cyanosis after providing Restlessness/confusion nursing intervention. Monitored level of Restlessness and anxiety are common appropriate nursing Wide-eyed appearance consciousness/mental status. manifestations of hypoxia. intervention. But Hyperventilation respiratory rate is not Presence of adventitious Evaluated level of activity tolerance. During acute respiratory distress, patient within 16-20 cpm breath sounds: Provided calm, quiet environment. may be totally unable to perform basic self- (42cpm). Rales/crackles on both Limited patient’s activity and care activities because of hypoxemia and lung fields Long Term Objective: encouraged bed rest during acute dyspnea. Rest interspersed with care Wheezing on inspiration Within the 3-day nursing phase. activities remains an important part of Long Term Objective: Changes in RR, depth and care, the client will be treatment regimen. rate able to establish and Outcome met. Cyanotic/cool & clammy maintain normal or Assisted patient to assume position Elevation of HOB facilitates respiratory Within the 3-day nursing skin effective respiratory of comfort (moderate high-back function by use of gravity, decreasing care, the client was able Use of orthopneic position pattern and be free of rest). Changed positions every 2 pressure of diaphragm and enhancing to establish and maintain Apprehension potential complications hours. ventilation of different lung segments. normal or effective Diaphoretic (pneumothorax, cardiac respiratory pattern and Nasal Flaring arrest, respiratory failure, Kept environmental pollution to a Precipitation of allergic type of respiratory free of potential Fluctuating Oxygen etc.) after providing minimum (dust, smoke, allergens) reactions that can trigger onset of acute complications
- 7. Saturation: <90% (without appropriate nursing and according to individual situation. episode. (pneumothorax, cardiac Oxygen), >90% (with collaborative arrest, respiratory failure, oxygen supplementation) interventions. Taught and encourage deep- Provides patient with some means to cope etc.) after providing Vital Signs: breathing and coughing exercises with or control dyspnea and reduce air appropriate nursing and Temp: 37.0 C and use of purse-lipped breathing. traffic. collaborative PR: 136 bpm interventions. RR: 42 cpm Kept resuscitation bag at bedside. Provides adequate ventilation when patient BP: 100/70 mmHg requires it. Observed for signs and symptoms To identify infectious process and promote of infections. timely interventions. Collaborative: Provided supplemental Enhances expectoration of sputum, humidification: partial rebreather improve pulmonary function, and reduces mask, 6L/min; nebulization. lung volumes. Monitored pulse oximetry, CXR. Establishes baseline for monitoring progression/regression of disease process and complications. Pulse oximetry- can detect changes in Oxygen saturation. NURSING CARE PLAN Identified Problem: Hypoxia leading to cyanosis Nursing Diagnosis: Impaired Cardiopulmonary Tissue Perfusion r/t alteration in gas exchange secondary to bronchospasm CUES OBJECTIVES INTERVENTIONS RATIONALE EVALUATION Subjective: Short Term Objective: Independent: Short Term Objective: “Hangak…” Within the 8 hours of Auscultated breath sounds. Noted Bronchospasm is present with obstruction Outcome met. “Naglisod ko ug ginhawa, nursing care, the patient adventitious breath sounds. in airway and may/may not be manifested After the 30-minute kutas akong ginhawa.” as will be able to identify and with adventitious breath sounds. health teaching the stated by the client. demonstrate ways and patient was able to interventions that will help Count patient RR in one full minute. Respirations may be shallow and rapid, identify and perform >Dyspnea/difficulty in improve her circulation with prolonged expiration in comparison to interventions (deep- breathing after 30 minutes of health inspiration. Tachypnea may be present. breathing exercises, teaching. coughing, pursed-lip Assisted patient to assume position Elevation of HOB facilitates respiratory breathing exercises) that Objective: of comfort (moderate high-back function by use of gravity, decreasing aided in her circulation
- 8. Labored breathing rest). Changed positions every 2 pressure of diaphragm and enhancing status. Used of accessory muscle hours. ventilation of different lung segments. Restlessness Long Term Objective: Wide-eyed appearance Within the 3 days of Kept resuscitation bag at bedside. Provides adequate ventilation when patient Long Term Objective: Hyperventilation nursing care, the patient requires it. Outcome met. Presence of adventitious will demonstrate After 3-day nursing care, breath sounds: improved perfusion and Patient Health Teaching: the patient was able to Rales/crackles on both circulation as evidenced Taught and encourage deep- Provides patient with some means to cope maintain improved lung fields by normal skin color, breathing and coughing exercises with or control dyspnea and reduce air perfusion and circulation Wheezing on inspiration reduction of breathing and use of purse-lipped breathing. traffic. as evidenced by normal Fluctuating Oxygen difficulty, relaxed state, skin color, SaO2 at 96%, Saturation: <90% (without SaO2 >90% and absence Taught patient about the treatment To provide information on how the patient decreased breathing Oxygen), >90% (with of cyanosis after regimen and disease process. will be able to prevent disease recurrence. difficulty, and patient is oxygen supplementation) providing appropriate at relaxed state. Productive cough nursing and medical Encouraged increase in total fluid Hydration helps decrease the viscosity of Difficulty vocalizing intervention. intake to at least 3000 mL/day, secretions, facilitating expectoration. Fluids Changes in RR, depth and within cardiac tolerance. during meals can increase gastric rate distention and pressure on the diaphragm. Cyanotic/cool & clammy skin Kept environmental pollution to a Precipitation of allergic type of respiratory Pallor minimum (dust, smoke, allergens) reactions that can trigger onset of acute Use of orthopneic position according to individual situation. episode. Apprehension Reduced tolerance to Collaborative: activity Provided supplemental Enhances expectoration of sputum, Vital Signs: humidification: partial rebreather improve pulmonary function, and reduces Temp: 37.0 C mask, 6L/min; nebulization. lung volumes. PR: 136 bpm RR: 42 cpm Monitored pulse oximetry, CXR. Establishes baseline for monitoring BP: 100/70 mmHg progression/regression of disease process and complications. Pulse oximetry- can detect changes in Oxygen saturation.
- 9. NURSING CARE PLAN Identified Problem: deprivation from oxygen decreases the energy level Nursing Diagnosis: Fatigue r/t poor physical condition secondary to generalized weakness due to hypoxic states CUES OBJECTIVES INTERVENTIONS RATIONALE EVALUATION Subjective: Short Term Objective: Independent: Short Term Objective: “Hangak…” Within the 8 hours of Recommended scheduling activities Prevents overexertion, allows for some Outcome met: “Naglisod ko ug ginhawa, nursing care, the patient for periods when the patient has activity within patient ability. The patient reported kutas akong ginhawa.” as will report improve sense most energy. improve sense of energy stated by the client. of energy as evidenced as evidenced by able to “Kapoy man magsige ug by able to do activities in Encouraged patient to do whatever Provides for sense of control and feeling of do activities in an lihok”, as verbalized by an acceptable level of what is possible. a accomplishment. acceptable level, and patient. fatigue and report report in increase energy increase energy level Demonstrated proper performance Protects patient from injury during activities. levels after providing > Dyspnea/difficulty in after providing of ADLs, position changes. appropriate nursing care. breathing appropriate nursing intervention. Encouraged nutritional intake/ use Necessary to meet energy needs for Objective: of supplements as appropriate. activity. Long Term Objective: Labored breathing Long Term Objective: Outcome met: Used of accessory muscle Within the 3-day of Monitored breath sounds. Hypoxemia and hypoxia increases sense of Within the 3-days of Hyperventilation nursing care, the client fatigue, impairs ability to function. nursing care, the client Changes in RR, depth and will be able to perform was able to perform rate ADLs and participate in Provided rest periods between Conserves patient’s energy. ADLs and participated in Cyanotic/cool & clammy desired activities at level activities desired activities at level skin of ability after providing of ability after providing Use of orthopneic position appropriate nursing and Collaborative: appropriate nursing and Apprehension collaborative Provided supplemental oxygenation: Provides increase in oxygenation thus collaborative Weak appearance interventions. partial rebreather mask, 6L/min; increases energy level. interventions. Drowsy nebulization. Unable to perform activities Evaluated need for individual Aid in patient’s performance of certain Vital Signs: assistance/assistive devices. activities. Temp: 37.0 C PR: 136 bpm RR: 42 cpm BP: 100/70 mmHg
- 10. NURSING CARE PLAN Identified Problem: Patient is unable to carry out routinely activities such as bathing, brushing, and etc. due to lack energy supply secondary decreased oxygen needs Nursing Diagnosis: Self-Care Deficit (hygiene and self-toileting) r/t general weakness secondary to hypoxic state CUES OBJECTIVES INTERVENTIONS RATIONALE EVALUATION Subjective: Short Term Objective: Independent: Short Term Objective: “Hangak…” as stated by the Within the 8 hours of Assessed level of self-care abilities Aids in planning for meeting individual Outcome met: client. nursing care, the patient and deficits in performing ADLs. needs. After 8 hours of “Maglisod man gyud ni siya and the SO will be able to nursing care, the patient ug lihok-lihok kay naglisod identify and demonstrate Provided devices and equipment that Promotes performance of self-care and the SO was able to siya ug ginhawa, ako na lang alternate ways to perform will aid the client in performing self- activities within client’s limitation. Also identify and demonstrate siyang tabangan.” as stated self-care such as using care: promotes independence. alternate ways to by SO. bedpan or commode, > glass of water and toothbrush perform self-care such > Dyspnea/difficulty in having bed bath, and > bedpan or urinal for elimination as using bedpan or breathing providing devices to >basin with water for hygiene commode, having bed brush teeth on bed after bath, and providing providing appropriate Maintained a supportive, firm attitude. Patients need empathy and to know and devices to brush teeth Objective: nursing and collaborative Allowed patient sufficient time to to know caregivers will be consistent in on bed after providing Labored breathing interventions. accomplish tasks. their assistance. appropriate nursing and Used of accessory muscle collaborative Restlessness/confusion Provided positive feedback for efforts Enhances sense of self-worth, promotes interventions. Wide-eyed appearance and accomplishments. independence, and encourages patient to Hyperventilation continue endeavors. Inability to perform Long Term Objective: Long Term Objective: activities such as bathing Within the 3-day nursing Encouraged SO to allow patient to do Reestablishes sense of independence Outcome met: and tooth brushing care, the client will be as much as possible for self. and fosters self-worth and enhances After the 3-day Weakened state able to perform self-care rehabilitation process. nursing care, the client Unable to go to CR activities within the level was able to perform self- Vital Signs: of her own ability after Collaborative: care activities within the Temp: 37.0 C providing appropriate Assisted or supported family with Enhances likelihood of finding individually level of her own ability PR: 136 bpm nursing and collaborative alternative placements as necessary. appropriate situation to meet client’s after providing RR: 42 cpm interventions. needs. appropriate nursing and BP: 100/70 mmHg collaborative interventions.