1. Journal of Hospital Infection (2008) 70, 166e173
Available online at www.sciencedirect.com
www.elsevierhealth.com/journals/jhin
Enhanced surgical site infection surveillance
following caesarean section: experience of
a multicentre collaborative post-discharge system
V.P. Ward a,*, A. Charlett a, J. Fagan b, S.C. Crawshaw c
a
Health Protection Agency, London, UK
b
Nottingham City Hospital, Nottingham, UK
c
NHS East Midlands, UK
Received 29 November 2007; accepted 2 June 2008
Available online 23 August 2008
KEYWORDS Summary The caesarean section rate in the UK has more than doubled
Caesarean section; during the last two decades and is continuing to rise. The majority of stud-
Antibiotic prescribing; ies carried out to determine the incidence of infection associated with this
Surgical site infection;
procedure have been restricted to the inpatient stay, which may give mis-
Risk factors
leading results. Women undergoing caesarean section have routine contact
with a community midwife after discharge. This provided an opportunity to
assess whether a collaborative surveillance approach between hospital and
community staff was feasible using routinely available information. Follow-
ing a successful pilot study, 11 maternity units in the East Midlands partici-
pated in an extended study. Complete records were available for 5563
(88%) women. Overall, 758 (13.6%) wound problems were reported, 84%
of which developed after discharge. Of these, 488 (8.9%) met national def-
initions for surgical site infection (SSI); however, there was a marked inter-
unit difference in incidence, ranging from 2.9% to 17.9%. Statistical models
were used to examine these differences using 12 possible risk factors. Five
risk factors were found to be significantly associated with the development
of a surgical site infection: body mass index, age, blood loss, method of
wound closure and emergency procedures. These results suggest that
caesarean section is associated with high infectious morbidity, the extent
of which would have been considerably underestimated without post-
discharge monitoring. Almost all women with wound problems were
treated with antibiotics, regardless of how minor the problem, with 97%
* Corresponding author. Address: Laboratory of Healthcare Associated Infection, Health Protection Agency, 61 Colindale Avenue,
London NW9 5HT, UK. Tel.: þ44 208 327 7332.
E-mail address: valerie.ward@hpa.org.uk
0195-6701/$ - see front matter ª 2008 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.jhin.2008.06.002
2. SSI surveillance following caesarean section 167
being prescribed in the community. This indicates a requirement for local
review of antibiotic prescribing practice.
ª 2008 The Hospital Infection Society. Published by Elsevier Ltd. All rights
reserved.
Introduction a multicentre prospective study carried out by the
US Centers for Disease Control (CDC).8
In the past 15 years, the proportion of caesarean Of the 1029 women who had caesarean de-
section births has been increasing steadily in liveries, inpatient and community records were
England, and now accounts for 24% of all births.1 available for 896 (87%). Using the criteria of the
More than 150 000 women were delivered in this study hospital, SSIs were classified as major if
way in 2005, making this procedure one of the wounds were discharging pus or inflamed and
most commonly performed major operations.2 required antibiotic therapy; or there was spreading
Although it has undoubtedly reduced infant and cellulitis and fever (>38 C), complete or partial
maternal mortality, studies have shown that the (50%) dehiscence, or required surgical revision/
procedure is associated with significant infectious debridement. Wound problems that did not meet
morbidity involving the operative site. Wound in- these definitions were classified as minor. A total
fection rates ranging between 7% and 41.1% have of 213 (23.7%) wound infections were identified
been reported.3,4 Although this wide variation from the records, 111 of which were classified as
may be due to differences in the criteria used to major. The majority of infections (89%) were
diagnose infection, case-finding, and the use of identified after discharge. All patients had been
antibiotic prophylaxis, the majority of studies routinely prescribed antibiotic prophylaxis. These
have been restricted to the inpatient stay. Under- results confirmed that wound infection was a signif-
estimation of the incidence of infection ranging icant problem following caesarean section and that
from 20% to 70% has been reported in general a combined hospital/community monitoring ap-
surgery if patients are not monitored after they proach was feasible.
leave hospital.5 A National Audit Office report On the basis of these results, it was decided to
considered that post-discharge surveillance was extend the study to other maternity units in the
important if National Health Service (NHS) Trusts same region. The primary objective of the main
were to understand the full extent of hospital- study was to prospectively study the occurrence
acquired infection, yet it had been attempted in of surgical wound and uterine infections following
only a quarter.6 Their recommendation, subse- caesarean section in maternity units throughout
quently endorsed by the Committee of Public the East Midlands region using a standardised
Accounts, was that post-discharge surveillance approach with common case-definitions and
should be considered.7 case-finding methods. Factors associated with
It was decided to investigate the incidence of post-delivery infectious morbidity would also be
surgical site infection (SSI) in a one-year study that identified and, because it had been ascertained
included post-discharge surveillance at a single that all units routinely gave antibiotic prophy-
maternity unit in the East Midlands during laxis, compliance with policies would be assessed.
2001e2002. This study used the fact that women
undergoing caesarean section have routine contact Study setting
with a community midwife for a minimum of 10
days after discharge, or longer if there are any Eleven maternity units within the East Midlands
wound or other obstetric-related problems. This region participated in the surveillance between
provided an opportunity to assess whether a col- July 2003 and March 2005, collecting data for
laborative surveillance approach between infec- varying periods of between three and 18 months.
tion control teams, and hospital and community Initially, seven units undertook to collect data for
midwives was feasible; and whether the incidence 12 months, although two units in one Trust had to
of infection following caesarean section and in- stop after six months due to staffing issues.
formation on potential risk factors could be de- Towards the end of the study period, four of the
termined from routine records. Included in the risk remaining five units within the region opted to
factor data to be collected were factors shown to take part, and the study period was extended for
be independently important in predicting SSI in another six months.
3. 168 V.P. Ward et al.
Methods criteria. In order to reduce inter-observer varia-
tion in the application of these definitions, all signs
Study design and symptoms of infection were recorded. This
information was then used to assess whether the
This was a prospective multicentre study. Each diagnostic criteria for incisional and uterine infec-
unit nominated maternity and infection control tions were met.
staff to co-ordinate the study.
Data collection
Study population The surveillance protocol was discussed and agreed
with collaborating obstetricians, hospital and com-
All women who underwent caesarean section at any munity midwives, and infection control and audit
of the participating units during the study period staff. Clinical, risk factor, and infection data items
were included in the surveillance. Patients were to be collected were based on results from the
followed up from the day of surgery until the date of preliminary study, a brief review of the literature,
last contact with the community midwife. and discussions with local experts in the field.
Close collaboration between hospital and com-
Definitions of infection munity midwifery staff was necessary for effective
study of this patient group. The required demo-
Based on the experience of the CDC, deep in- graphic and inpatient information was routinely
cisional infections involving the fascial and muscle recorded in a variety of sources, including maternity
layers rarely occur after caesarean section unit databases, theatre records, and patient ante-
(T. Horan, personal communication). Therefore, natal records. In the UK, postnatal follow-up care is
for the purposes of this study, infections of the entered on to a patient-held record. Community
surgical site were classified as either incisional midwives were asked to ensure that any signs and
(wound) or uterine (endometritis). The definitions symptoms that could suggest the presence of in-
of incisional infection used were those adopted by fection were clearly and consistently recorded,
the Health Protection Agency (HPA) for the na- together with details of action taken. Once care of
tional Surgical Site Infection Surveillance Service the patient had been handed over to the health
(SSISS) and can be found at http://www.hpa. visitor, the community midwife returned the record
org.uk/infections/topics_az/hai/SSI_Protocol.pdf. to the hospital, where the required data were
As the SSISS does not currently include caesarean abstracted by the study co-ordinators.
sections, the CDC definitions for uterine infections Participating units could choose to enter the
were used.9 The criteria for defining incisional and data directly into a local database, or use a case
uterine infections are shown in Table I. These record form that was designed to be read using
definitions are based on a number of separate optical mark recognition (OMR) software. Units
Table I Criteria for defining incisional and uterine infections
Incisional infections
1 Purulent drainage.
2 Culture from wound swab, or aseptically aspirated fluid or tissue, yields organisms and pus cells present on
microscopy.
3 At least two of the following symptoms and signs of inflammation: pain or tenderness, localised swelling,
redness or heat, and
(a) incision deliberately opened by surgeon to manage the infection, unless incision culture-negative, or
(b) clinician’s diagnosis of incisional infection.
4 Wound spontaneously dehisces, or deliberately opened by surgeon, and at least one of the following symptoms
and signs of inflammation: localised pain or tenderness, fever (38 C), unless incision culture-negative.
5 Abscess or other evidence of infection found during reoperation, or by histopathological/radiological
examination.
Uterine infections
1 At least two of the following symptoms and signs of infection: fever (38 C), abdominal pain, uterine
tenderness, purulent drainage from uterus.
2 Organisms cultured from fluid or endometrial tissue obtained during operation, needle aspiration, or brush
biopsy.
4. SSI surveillance following caesarean section 169
that were able to collect much of the required analysis included a random term for maternity unit
information electronically from databases within in order to allow for any inter-unit variation in the
the hospital opted to use the Excel database incidence of infection. The factors analysed were
provided to ensure that the data were in the age, body mass index (BMI), ruptured membranes,
agreed format, and data fields correctly labelled. in labour at the time of surgery, preoperative
Information on wound problems that occurred stay, American Society of Anesthesiologists (ASA)
after discharge were manually retrieved from score, prophylactic antibiotics, emergency pro-
community records and transferred either to the cedure, grade of surgeon, duration of caesarean
electronic or paper record. section, blood loss, and method of wound closure.
Regardless of the preferred method of collec- Those factors where there was no evidence of an
tion, all data were forwarded to the regional association were sequentially removed from the
co-ordinating centre at the East Midlands Health regression model provided the regression coeffi-
Protection Agency for collation before being down- cients of the other factors in the model did not
loaded to the HPA Centre for Infections for consis- change markedly. All factors removed from the
tency checking and statistical analysis. All patient regression model were included in the final model
identifiers were removed, and a unique number to ensure that they were not associated.
allocated to each record. Data transfer was pass-
word-protected and information was held securely Results
at both sites according to Caldicott principles.
Although inpatient information was available for
Statistical methods the 6297 caesarean section procedures carried out
during the study period, inclusion was dependent
The variation in incisional and uterine infection on the return of the community follow-up records
rates between maternity units was assessed using to the hospital by the community midwives. Both
c2-tests of association. The assessment of the hospital and community information was available
length of follow-up was performed using a non- for 5563 (88%) of the patients.
parametric test for the equality of medians.
The strength of association between potential Length of follow-up
risk factors and the development of an infection
that met the study definitions was measured using Overall the median length of follow-up was 15 days
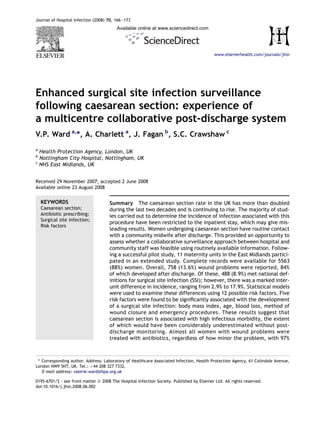
a random effects logistic regression analysis. This (Figure 1). For hospital stay, the median was 3 days,
20
18
16
14
12
Days
10
8
6
4
2
0
1 2 3 4 5 6 7 8 9 10 11
Maternity unit
Figure 1 Length of inpatient stay and community follow-up by unit. Grey bars: mean length of hospital stay; black
bars: mean community follow-up.
5. 170 V.P. Ward et al.
quartiles 3, 4. For community follow-up, the median two of the signs and symptoms associated with
was 11 days, quartiles 8, 17. There was marked endometritis; 95 (82.6%) of these included puru-
inter-unit variation in the length of follow-up, this lent drainage.
variation being highly significant (P 0.0001).
Antibiotic usage
Incidence of infection
All the maternity units routinely gave antibiotic
A total of 745 surgical wound problems and/or prophylaxis. Apart from 34 women who were
uterine infections were recorded in 738 (13.3%) of already on antibiotics for other reasons, 5493
the 5563 women (Figure 2). Of these, 488 (65.5%) met received prophylaxis, with 97% given as per the
the study definitions. For 370 incisional infections hospital policy.
that met the criteria, the mean was 6.7% (range: Of the 478 women who developed incisional
2.9e12.4). For uterine infections, 118 met the study and/or uterine infections, 459 (96%) were treated
definitions (mean: 2.1%, range: 0e5.5%). There was with antibiotics. A further 22 women received
wide inter-hospital variation for the two types of in- antibiotics despite there being little or no evi-
fection, both of which were highly significant dence to support their use. Almost all of the 257
(P 0.0001). Only 78 of the 488 SSIs (16%) were diag- women (99%) with wound problems that did not
nosed during the inpatient stay, with the remainder meet the study definitions were also treated with
being identified after discharge from hospital. antibiotics.
Almost all (98%) incisional infections met one of
two of the five possible criteria for infection. Of Risk factors
the 370 identified, 204 (55.1%) had purulent
drainage from the incision, and 158 (42.7%) had Since 98% of women had received prophylactic
two or more signs and symptoms of infection plus antibiotics, this factor was not included in the
clinician’s diagnosis. Many surgeons consider pus analysis. Univariable analysis indicated that seven
to be the most important criterion for infection. of the remaining 11 variables were significantly
There were marked inter-unit differences between associated with infection: BMI (P 0.0001), emer-
the proportions of infections associated with puru- gency procedures (P ¼ 0.002), ruptured mem-
lent drainage, ranging from 0 to 91%. branes (P ¼ 0.01), in labour at the time of surgery
For the 118 uterine infections reported that met (P 0.001), duration of procedure (P ¼ 0.002) and
the study definitions, 115 were based on at least wound closure method (P ¼ 0.003).
20
928
18
16
Incidence per 100 operations
14 444
12
10 848
8 360 858
256
6 440
257 281
823
4 68
2
0
1 2 3 4 5 6 7 8 9 10 11
Maternity unit
Figure 2 Incidence of incisional and uterine infections that met the study definitions by unit. Numbers above bars
indicate numbers of patients. Grey bars: incisional infection; black bars: uterine infection.
6. SSI surveillance following caesarean section 171
A total of 2328 women had elective surgery, 128 increased by 70% (P 0.0001) for each 10-unit
(5.5%) of whom developed an incisional wound increase in BMI. Maternal age was associated with
infection. The corresponding number for the 3234 subsequent development of an infection, with older
women who had emergency procedures was 242 women being less likely to develop infection. This
(7.5%). This difference was statistically significant finding was also observed by Myles et al., although
(P ¼ 0.003). Conversely, there was no significant dif- it was not significant in their multivariable model.10
ference for uterine infections, with 1.9% of women There was an estimated 3% increase in the odds of
who had elective surgery developing an infection developing an infection for each additional 100 mL
compared to 2.3% who had emergency procedures. of blood loss and a 25% increase for women undergo-
With regard to wound closure methods, a num- ing emergency procedures. For wound closure, the
ber of consultant obstetricians had requested that risk was 39% higher when staples were used. Other
this information be collected at the protocol de- methods were associated with a five-fold increase,
velopment stage. The majority (70%) of women although this only involved nine women.
had continuous sutures, 23% of wounds had been
stapled and 2% had intermittent/other methods of Discussion
closure. For infections that met the study defini-
tions, the incidence was significantly higher when This study has demonstrated the feasibility and
staples were used, being 12.2% compared to 7.5% usefulness of post-discharge surveillance in a group
with continuous sutures (P 0.0001). of patients undergoing one of the most com-
The other factor of interest to obstetricians was monly performed operative procedures. Hospital-
grade of surgeon. Registrars performed 75% of acquired infections delay recovery, may increase
caesarean sections, consultants 14%, and senior the duration of hospital stay, and have economic
house officers (SHOs) 12%. There was only weak consequences for the primary and secondary
evidence that consultants had a lower infection healthcare sectors.11e13 In a Department of Health
rate than registrars. SHOs had a slightly higher (DH)-commissioned study undertaken in 1994e
incidence of infection. However, most (71%) of the 1995, it was estimated that the average additional
caesarean sections performed by SHOs were un- inpatient cost of surgical wound infections follow-
dertaken at two of the 11 maternity units. Of the ing caesarean section was £524.11 Inevitably this
72 infections that developed in the women oper- cost will have risen over the ensuing decade.
ated on by an SHO, only 12 occurred in the other In the 5563 patients followed up during their
nine maternity units, which limited the ability of hospital stay and after discharge, there was an 8.9%
this study to assess whether this observed excess incidence of SSI that met the study definitions. This
was real or due to other hospital-related factors. incidence is broadly similar to results reported in
The risk factors were then assessed using a mul- recent studies that used CDC definitions of infec-
tivariable logistic regression model (Table II). Five tion.14e17 Without post-discharge surveillance there
factors remained statistically significant after would have been a considerable underestimate of
controlling for any potential confounding effects the incidence of infection at all units, since 84%
of the other factors. BMI remained strongly associ- were identified after discharge. This is consistent
ated with the subsequent development of a surgical with a recently published UK study showing that
site infection. The odds of developing an infection 71% of infections were diagnosed in the community.14
Table II Multivariable analysis of all infections meeting study definitions
Factor Category N (%) Estimated OR 95% CI P-value
BMI (per 10 units) e 4897 (88.0) 1.70 1.47e1.97 0.0001
Age (per 10 years) e 5558 (99.9) 0.82 0.69e0.99 0.04
Blood loss (per 100 mL) e 5525 (99.3) 1.03 1.01e1.05 0.009
Type of surgery Elective 2328 (41.8) Referent
Emergency 3234 (58.1) 1.25 1.00e1.56 0.05
Unknown 1 (0.1) e
Type of closure Continuous 3906 (70.2) Referent
Intermittent 102 (1.8) 0.73 0.27e1.96
Staples 1273 (22.9) 1.39 1.08e1.79
Other 9 (0.2) 5.35 1.00e28.61 0.01
Unknown 273 (4.9) e
OR, odds ratio; CI, confidence interval; BMI, body mass index (kg/m2).
7. 172 V.P. Ward et al.
Effective surveillance following caesarean sec- consensus regarding the choice of drug, regimen,
tion requires a multidisciplinary approach between or method of administration, and whether pro-
infection control nurses, hospital and community phylaxis should be restricted to high-risk pa-
midwives and other healthcare personnel. The tients.20 Several different regimens were used by
principles of clinical governance apply to all who the 11 maternity units that took part in the study.
provide or manage patient care services in the NHS, Further analysis is being done to compare these
and require them to work in partnerships to provide regimens and to assess whether these impact on
integrated care to promote quality and improve the the incidence of infection.
patient experience of healthcare.18 By using the With regard to the treatment of wound prob-
fact that women undergoing caesarean section lems, 96% of women who developed SSI that met
have routine contact with a community midwife the study definitions received antibiotics. How-
for a minimum of 10 days, this study demonstrates ever, it should be noted that almost all of the 257
the feasibility of a collaborative approach to post- women (99%) with wound problems that did not
discharge surveillance. meet the study definitions were also treated with
Strategies to prevent, or at least decrease, the antibiotics. In line with good antibiotic steward-
risk of infection are needed. There is evidence to ship there is a need for reviewing and monitoring
suggest that infection rates can be reduced when antibiotic prescribing locally.
routine surveillance with feedback of rates to staff In the course of this study, data on a number of
is included in infection control programmes.19 For risk factors for the development of infection were
the duration of the study, midwives and infection collected. BMI, age, blood loss, method of wound
control staff from participating units met with closure, and emergency surgery were found to be
the project team at bi-monthly intervals. As significantly associated with the development of
well as feeding back results, various issues identi- SSI. Work is ongoing to further examine the factors
fied during the study were discussed and possible that comprise risk indices developed specifically by
solutions offered. Several positive outcomes were CDC for uterine and incisional wound infections and
reported. The benefits of cross-departmental/ to assess the utility of these indices in a UK setting.
multiprofessional working were being realised and Both midwives and infection control nurses af-
staff were more receptive to the need for infection firmed the need to carry out surveillance in this
control measures in view of the unexpectedly high group of patients, but there are clearly workload
incidence of wound problems reported. As well as implications. Standardisation of maternity records,
hand hygiene campaigns, theatre audits had particularly those used in the community, and
been carried out when one unit reported a very electronic linkage of data are high priorities if
high number of staff and students present during routine surveillance following caesarean section is
caesarean sections. As a result, new procedures to be incorporated into quality improvement pro-
had been instituted to limit the number of staff grammes locally, regionally and nationally.
in theatre during a delivery. The choice of wound
closure method varied, and may be influenced by
individual preference, speed of insertion and sur- Acknowledgements
geon experience. However, some obstetricians
began to review their practice after issues with We thank the staff of participating hospitals and
wound closure methods were highlighted. Issues the East Midlands Health Protection Unit for their
around the standards of record-keeping, unifor- help and support.
mity of information in the maternity records and
delays in returning postnatal records to the hospi- Conflict of interest statement
tal were also addressed. A marked improvement None declared.
was reported as the study progressed. When ex-
amining infection trends over the period of the Funding sources
study, the decrease in the incidence of infection None.
was statistically significant over time (P ¼ 0.003),
with the decrease being more marked for the
units who had participated for longer. References
Prophylactic antibiotics were administered to
1. NHS Institute for Innovation and Improvement. Delivering
98% of patients and compliance with prescribing
quality and value. Focus on: Caesarean section. Coventry:
policy was good. Antibiotics are now routinely NHS Institute for Innovation and Improvement; 2006.
prescribed for this group of patients in many 2. Office of Health Economics. Compendium of health statis-
healthcare facilities, although there is no tics. 18th edn. London: Radcliffe Publishing; 2007.
8. SSI surveillance following caesarean section 173
3. Hillan EM. Postoperative morbidity following Caesarean 11. Reilly J, Allardice G, Bruce J, et al. An economic analysis of
delivery. J Adv Nurs 1995;22:1035e1042. surgical wound infection. J Hosp Infect 2001;49:245e249.
4. Henderson E, Love EJ. Incidence of hospital-acquired infec- 12. Smyth ETM, Emmerson AM. Surgical site infection surveil-
tions associated with caesarean section. J Hosp Infect 1995; lance. J Hosp Infect 2000;45:173e174.
29:245e255. 13. Plowman R, Graves N, Griffin MAS, et al. The socio-
5. Holtz TH, Wenzel RP. Postdischarge surveillance for nosoco- economic burden of hospital-acquired infection. London:
mial wound infection: a brief commentary. Am J Infect Public Health Laboratory Service; 1999.
Control 1992;20:206e213. 14. Johnson A, Young D, Reilly J. Caesarean section surgical site
6. Report by the Comptroller and Auditor General e HC 230 infection. J Hosp Infect 2006;64:30e35.
Session 1999e2000. The management and control of 15. Killian CA, Graffunder EM, Vinciguerra TJ, et al. Risk factors
hospital acquired infection in acute NHS Trusts in England. for surgical-site infections following caesarean section.
London: Stationery Office; 2000. Infect Control Hosp Epidemiol 2001;22:613e617.
7. House of Commons. Forty-second report from the commit- 16. Opoien HK, Valbo A, Grinde-Anderson A, et al. Post-cesar-
tee on public accounts. The management and control of ean surgical site infections according to CDC standards:
hospital acquired infection in acute NHS Trusts in England. rates and risk factors. A prospective cohort study. Acta
London: Stationery Office; 2000. Obstet Gynecol Scand 2007;86:1097e1102.
8. Horan T, Culver D, Gaynes R. Results of a multicenter study 17. Tran TS, Jamulitrat S, Chongsuvivatwong V, et al. Risk fac-
on risk factors for surgical site infections (SSI) following tors for postcesarean surgical site infection. Obstet Gynecol
C-section (CSEC). Am J Infect 1996;24:84. 2000;95:67e71.
9. Horan TC, Gaynes RP. Surveillance of nosocomial infections. 18. Report of the Expert Maternity Group. Changing childbirth
In: Mayhall CG, editor. Hospital Epidemiology and Infection (Part 1). London: Stationery Office; 1995.
Control. 3rd edn. Philadelphia: Lippincott Williams 19. Haley RW, White JW, Culver DH, et al. The efficacy of infec-
Wilkins; 2004. p. 1659e1702. tion surveillance and control programmes in preventing
10. Myles TD, Gooch J, Santolaya J. Obesity as an indepen- nosocomial infection in US hospitals. Am J Epidemiol 1985;
dent risk factor for infectious morbidity in patients who 121:182e205.
undergo cesarean delivery. Obstet Gynecol 2002;100: 20. Smaill F, Hofmeyr GJ. Antibiotic prophylaxis for cesarean
959e964. section. Cochrane Database Syst Rev 1999;(2). CD000933.