
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Hodgkins Non-Hodgkins Lymphoma Differences
Similaire à Hodgkins Non-Hodgkins Lymphoma Differences (20)
Plus de specialclass
Plus de specialclass (20)
Dernier
Dernier (20)
Hodgkins Non-Hodgkins Lymphoma Differences
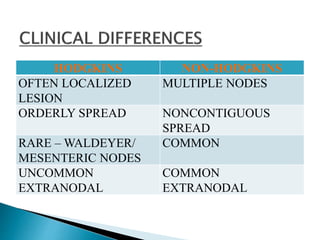
- 1. HODGKINS NON-HODGKINS OFTEN LOCALIZED LESION MULTIPLE NODES ORDERLY SPREAD NONCONTIGUOUS SPREAD RARE – WALDEYER/ MESENTERIC NODES COMMON UNCOMMON EXTRANODAL COMMON EXTRANODAL
- 3. Reed-Sternberg present ◦ Derived from germinal center or post germinal center B cells Background of Reactive Inflammatory Cells of Various types Variable Fibrosis * LACK THE MONOMORPHIC APPEARANCE OF OTHER LYMPHOMA
- 5. Account for 0.7% of new Ca in USA Arise in a Single or Chains of LN Most common Malignancy in YOUNG ADULTS ( 32y/o) Curable in most cases May progress to NHL or Leukemia ◦ spontaneously or after Tx.
- 6. Unknown EBV plays a role 50% present in R-S cells (Mixed Cellularity) High incidence Hx of IM Genetic Susceptibility
- 7. EBV (+) RS EXPRESS LATENT MEMBRANE PROTEIN-1 ◦ PROTEIN ENCODED BY EBV ◦ HAS TRANSFORMING ACTIVITY ◦ UPREGULATES NF- Kb EBV (-) RS cells ◦ ACQUIRED MUTATION OF NEGATIVE REGULATOR OF NF-kB
- 8. ACTIVATION OF NF-kB RESCUES DOOMED CELLS FROM APOPTOSIS RS cell PRODUCE CYTOKINE ACCUM. REACTIVE CELLS SUPPORT GROWTH & SURVIVAL OF TUMOR CELLS ◦ IL-5, IL-6, IL-13 ,TNF
- 9. Predictable Spread 1st to Contiguous Nodes ◦Nodal Disease First Spleen Liver BM Extranodal
- 10. Soft to hard , large Lymph Node Nodularity common in Nodular Sclerosis Foci of necrosis + Heterogenous c/s except for LYMPHOCYTE PREDOMINANCE Matted L.N. in Advanced cases
- 11. PAINLESS LYMPHADENOPATHY PAIN INVOLVED L.N. W/ ALCOHOL ◦ Paraneoplastic Symptom CUTANEOUS ANERGY ◦ Depressed Cellular immunity IMMUNE DYSFUNCTION ◦ UNKNOWN, PERSIST AFTER Tx. INCREASED RISK FOR 2ND CANCERS ◦ AML, BREAST Ca GASTRIC Ca Limited Disease is Cured w/ Local RadioTx
- 12. STAGE CRITERIA I In one lymph node only II In 2 or more LN on same side of the diaphragm III In the Lymph nodes, Spleen, or Both AND on Both sides of the diaphragm 1 Above the renal vessels (eg. Spleen, splenic, hilar, celiac, portal nodes 2 In the lower abdomen ( periaortic, pelvic, or imguinal nodes ) IV Extranodal involvement ( eg. Bone marrow, Lung, Liver ) A – absence of Systemic manifestation B – presence of Systemic manifestation NIGHT SWEATS, FEVER, WEIGHT LOSS
- 13. Stage I or II Stage III or IV Systemic s/s Usually absent Usually present Type Nodular sclerosis MC or LD 5 year disease free 90% 60-70% Systemic manifestation: NIGHT SWEATS, FEVER, WEIGHT LOSS
- 14. Tumor stage is most important Prognostic Variable ◦ Not Histologic Type ◦ R/T to current Tx protocols Long term survivors of ChemoTx and RadioTx ◦ Increased risk fro secondary Ca ◦ Breast Ca common in: Females Tx w/ RadioTx to chest during adolescence ◦ AML/ Myelodysplastic syndrome common ChemoTx
- 16. MOST COMMON 65-70% MALE = FEMALES ADOLESCENT & YOUNG ADULTS EXCELLENT PROGNOSIS
- 17. Stage 1 or 2 LOWER CERVICAL , SUPRACLAVICULAR & MEDIASTINAL L.N. RARELY ASSOC. EBV
- 18. LACUNAR TYPE Abundant COLLAGEN BAND NODULAR POLYMORPHOUS BACKGROUND DXTIC RS CELLS LESS FREQUENT
- 20. LACUNAR RS
- 22. 20-25 % MALES > FEMALES STRONGLY ASSOC. W/ EBV OLDER & YOUNG ADULTS ( BIPHASIC ) > 50% PRESENT AS STAGE 3-4 accompanied by SYSTEMIC SYMPTOMS Prognosis Very Good
- 23. FREQUENTLY SEE MONONUCLEAR & DXTIC RS CELLS DXTIC RS CELLS Are numerousMONONUCLEAR
- 25. UNCOMMON M>F OLDER ADULTS FREQUENT MONONUCLEAR AND DXTIC R-S CELLS ◦ REACTIVE T LYMPHOS PREDOMINATES 40% EBV ASSOC. PROGNOSIS EXCELLENT
- 27. 5% OF CASES , UNCOMMON MALES > FEMALES ( < 35 y/o ) ◦ Asymptomatic YOUNG MALES WITH CERVICAL OR AXILLARY LYMPHADENOPATHY ◦ MEDIASTINAL INVOLVEMENT IS RARE NOT ASSOC. W/ EBV PROGNOSIS EXCELLENT
- 28. NODULAR PATTERN DUE TO EXPANDED B-CELL FOLLICLES ◦ POPULATED BY L&H CELLS AND REACTIVE B-CELL ◦ DXTIC RS DIFFICULT TO FIND 3-5% PROGRESS DIFFUSE LARGE CELL
- 29. POPCORN RS CELLS L & H variants NUMEROUS MATURE LYMPHOCYTES
- 30. <5 % LEAST COMMON OFTEN ASSOC. EBV COMMON * OLDER PTS. * HIV * NON-INDUSTRIALIZED COUNTRIES SYSTEMIC SYMPTOMS PRESENT AS ADVANCED STAGE PROGNOSIS LESS FAVORABLE