Disha NEET Physics Guide for classes 11 and 12.pdf
Pediatric Trauma IEP Newsletter April 2016
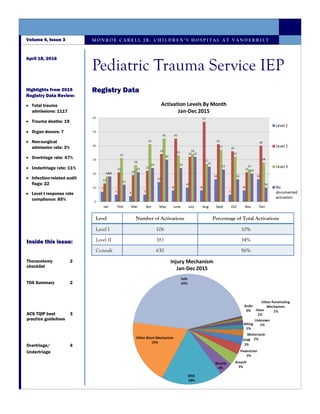
1. Registry Data
M O N R O E C A R E L L J R . C H I L D R E N ’ S H O S P I T A L A T V A N D E R B I L T
April 18, 2016
Volume 4, Issue 3
Pediatric Trauma Service IEP
Highlights from 2015
Registry Data Review:
Total trauma
admissions: 1117
Trauma deaths: 19
Organ donors: 7
Non-surgical
admission rate: 3%
Overtriage rate: 47%
Undertriage rate: 11%
Infection-related audit
flags: 22
Level I response rate
compliance: 85%
Inside this issue:
Thoracotomy
checklist
2
TDS Summary 2
ACS TQIP best
practice guidelines
3
Overtriage/
Undertriage
4
Level Number of Activations Percentage of Total Activations
Level I 106 10%
Level II 381 34%
Consult 630 56%
2. Family conversations:
According to Federal regulations, the
family of each potential donor is to be
informed of their loved one’s
opportunity to donate. Per your
hospital’s policy, TDS is the designated
party responsible for presenting the
opportunity of donation.
During the organ donation process, the
hospital and OPO will develop a plan
for the opportunity of donation to be
presented to the family, or discuss the
registered donor options, at the most
appropriate time.
Triggers:
It is the responsibility of the patient’s
nurse or designee to contact TDS
within one hour of a patient first
meeting one of the following clinical
indicators:
GCS ≤5 due to condition/illness
Beginning discussion of end of life
and/or withdrawal
Organ donation is no longer an option
when a patient is extubated. Always
notify TDS if the patient’s medical
status declines or if the plan of care
changes.
Pathways:
There are two pathways to donation
that can take place at the end of life.
Donation after Brain Death
TDS will input orders as the
Attending Physician, StarPanel
chart will change to Donor, Last
Name
Donation after Circulatory Death
Patient will remain under the
care of ICU Attending and work
in conjunction with TDS to input
orders. Name will not change.
Thoracotomy Checklist
Tennessee Donor Services
Page 2
Pediatric Trauma Service IEP
PED Thoracotomy Checklist
Pre-arrival actions Immediate actions
Thoracotomy tray out on mayo stand Patient’s left arm positioned above their head
10 blade and handle out on mayo stand Left chest painted with betadine
Procedural lights ON and positioned at proceduralist’s pref-
erence
Procedure lights focused on left chest
Betadine at bedside Move mayo stand within arm’s reach of proceduralist
Notify OR of procedure possibility and request assistance Open thoracotomy tray and place within arm’s reach of
Yankuer suction catheter and suction canister devoted to
procedure
ETT placed by PED team
OR blue towels NGT/OGT placed by RN3
Standby items (open upon trauma leaders request)
Activation of MTP Level I infuser
10ml syringes 16fr foley catheter
Central line kit Sutures
The PED will be adding the following checklist to the thoracotomy tray cabinet to assist in expediting the procedure.
3. Background:
> 60% of injuries involve the musculoskeletal system.
> 50% of hospitalized trauma patients have at least one musculoskeletal injury that could be life threatening, limb threatening,
or result in significant functional impairment.
Orthopaedic injuries are often associated with significant health care costs, decreased productivity in the workplace, and, in
some cases, long-term disability.
Open fractures:
Patients with open fractures receive intravenous antibiotics within 60 minutes of presentation to your ED.
All patients with open fractures are evaluated for the potential need for tetanus vaccination.
Patients with open fractures are taken to the operating room for surgical irrigation and debridement within 24 hours of
presentation to your ED.
Mangled extremity:
All patients who present to the emergency department with a mangled extremity undergo prompt orthopaedic evaluation (as
defined by institutional protocol).
All patients with a mangled extremity have timely (as defined by institutional protocol) operative management.
Compartment syndrome:
All patients diagnosed with compartment syndrome who require an amputation of the involved extremity are identified and
reviewed by the trauma PIPS or equivalent committee within the hospital.
Pelvic trauma/ associated hemorrhage:
Patients with hemorrhage from pelvic fractures are evaluated promptly by orthopaedics (as defined by institutional protocols)
A team with angiographic capabilities is consulted and promptly (as defined by institutional protocols) evaluates all patients
with pelvic fractures, evidence of contrast extravasation on cross-sectional imaging, and either hemorrhage or hemodynamic
stability.
Supracondylar humerus fractures
All patients with radiographic evidence of a supracondylar humerus fracture are promptly (as defined by institutional protocol)
evaluated by an orthopaedic surgeon
All patients with supracondylar fractures who do not receive timely management (for example, surgical repair within 18 hours
for Gartland Type III fractures) are identified and reviewed by the trauma PIPS or equivalent committee within the hospital.
Any patient with evidence of global forearm dysfunction or ischemia following supracondylar humerus fracture is identified
and reviewed in the trauma PIPS or equivalent committee within the hospital.
Rehabilitation of the multisystem trauma patient:
All delays in discharge of multisystem trauma patients due to inadequate or unavailable rehabilitation services are identified
and reviewed by the trauma PIPS or equivalent committee within the hospital.
Current Orthopaedic metrics being collected on the ACS application:
Time to IV antibiotics for open fractures should be less than 1 hour from presentation to your ED (and # of pts).
Time to operative I+D (not ER or ICU) for open tibia fractures should be less than 24 hours from presentation to your ED.
The percent of femoral shaft fractures (shaft only) treated with an IMN, plate and screws, or external fixation within 24 hours
of presentation to your ED.
ACS TQIP Orthopaedic Best Practice Guidelines
Page 3
Volume 4, Issue 3
4. Definitions:
Undertriage is a level II/III activation or “no activation” with an injury severity score (ISS) 16-75 call divided by the total
patients with “limited” or “no activation”. Other factors to consider in the definition of a major trauma patient may include
those requiring blood transfusion as part of their initial resuscitation or requiring intubation, intensive care unit admission,
emergent surgery or interventional catheter-based control of hemorrhage, or intracranial pressure monitoring.
Overtriage is the level I trauma activation with an ISS 0-15 cell divided by the total patients with level I activations.
ACS criteria pertaining to overtriage and under triage:
Rigorous multidisciplinary performance improvement is essential to evaluate overtriage and undertriage rates to attain the
optimal goal of less than 5 percent undertriage (CD 3–3). Undertriage cases should be reviewed in depth.
Rates of undertriage and overtriage must be monitored and reviewed quarterly (CD 16–7).
Injury severity score:
The Injury Severity Score (ISS) is an anatomical scoring system that provides an overall score for patients with multiple injuries.
Each injury is assigned an Abbreviated Injury Scale (AIS) score and is allocated to one of six body regions (Head, Face, Chest,
Abdomen, Extremities (including Pelvis), External). Only the highest AIS score in each body region is used. The 3 most severely
injured body regions have their score squared and added together to produce the ISS score.
An example of the ISS calculation is shown below:
Review of undertriage/overtriage cases:
Our PM&I committee reviews undertriage/overtriage rates monthly and these rates are also shared with our FlightCom/
LifeFlight staff.
Each case is reviewed with the FlightCom manager to look for areas of opportunity.
In the majority of cases, the identified opportunity is attributed to one of the following:
Pre-hospital crew’s failure to report specific injuries or abnormal vital signs.
MCJCHV level I or level II criteria not followed leading to either overtriage or undertriage.
Criteria misinterpreted or taken to the extreme (i.e.– dog bite to face considered penetrating injury to the head).
Proposed solution:
Education sessions with FlightCom provided by both the Trauma Program Manager and CRPC/Outreach team.
TPM component will focus on the criteria itself and identifying proper activation levels based on criteria.
Monroe Carell Jr. Children’s Hospital at Vanderbilt
Overtriage and Undertriage
Region Injury Description AIS Square Top Three
Head & Neck Cerebral contusion 3 9
Face No injury 0
Chest Flail chest 4 16
Abdomen
Minor contusion of liver
Complex rupture of spleen
2
5
25
Extremity Fractured femur 3
External No injury 0
50Injury Severity Score