Lecture 3. epid. charact. of vector borne infections
Malaria
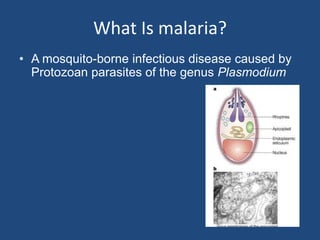
1. What Is malaria?
• A mosquito-borne infectious disease caused by
Protozoan parasites of the genus Plasmodium
2. What Is malaria?
• Transmitted only by Anopheles Mosquitoes
(>60 species!)
Seattle Biomedical Research Institute
3. Plasmodium species which
infect humans
Plasmodium vivax
Plasmodium ovale
Plasmodium falciparum
Plasmodium malariae
Plasmodium knowlesi
4. Components of the Malaria Life Cycle
Sporogonic cycle
Infective Period
Mosquito bites
uninfected
person Mosquito Vector
Parasites visible Human Host
Mosquito bites
gametocytemic
Prepatent Period Symptom onset
person
Recovery
Incubation Period
Clinical Illness
5. Malaria Life Sporogony
Cycle Oocyst
Life Cycle Sporozoites
Mosquito Salivary
Zygote Gland
Hypnozoites
Exo- (for P. vivax
and P. ovale)
erythrocytic
(hepatic) cycle
Gametocytes
Erythrocytic
Cycle
Schizogony
6.
7. Acute Symptoms
• Classical features include cyclic symptoms
– Cold stage: chills and shaking
– Hot stage: fever, headache, vomiting, seizures in
children
– Sweating stage: weakness
– Feel well for period of time, then cycle repeats itself
www.uhhg.org/mcrh/resources/video/malariappt.pdf
8. Clinical presentation
• Early symptoms
– Headache
– Malaise
– Fatigue
– Nausea
– Muscular pains
– Slight diarrhea
– Slight fever, usually not intermittent
• Could mistake for influenza or gastrointestinal
infection
9. Clinical presentation
• Acute febrile illness, may have periodic febrile
paroxysms every 48 – 72 hours with
• Afebrile asymptomatic intervals
• Tendency to recrudesce or relapse over months to
years
• Anemia, thrombocytopenia, jaundice,
hepatosplenomegaly, respiratory distress
syndrome, renal dysfunction, hypoglycemia,
mental status changes, tropical splenomegaly
syndrome
10. Malarial Paroxysm
• Can get prodrome 2-3 days before
– Malaise, fever,fatigue, muscle pains, nausea, anorexia
– Can mistake for influenza or gastrointestinal infection
– Slight fever may worsen just prior to paroxysm
• Paroxysm
– Cold stage - rigors
– Hot stage – Max temp can reach 40-41o C,
splenomegaly easily palpable
– Sweating stage
– Lasts 8-12 hours, start between midnight and midday
11. Malarial Paroxysm
• Periodicity
– Days 1 and 3 for P.v., P.o., (and P.f.) - tertian
– Usually persistent fever or daily paroxyms for
P.f.
– Days 1 and 4 for P.m. - quartian
12. Each disease has a distinct course
“Tertian Malaria”
(P.falciparum, P.ovale and
fever occurs every third da
“Quartan Malaria”
(P. malariae)
fever occurs every fourth
www.uhhg.org/mcrh/resources/video/malariappt.pdf
13. Each disease also has a distinct geographical
distribution
www.columbia.edu/itc/hs/medical/pathophys/parasitology/2006/PAR-05Color .pdf
14. Each disease also has a distinct geographical
distribution
www.columbia.edu/itc/hs/medical/pathophys/parasitology/2006/PAR-05Color .pdf
15. DIAGNOSIS
Gold standard:
Multiple thick and thin
smears
16. Other tests
Generally the complete blood counts and platelets
counts are of little benefit in the diagnosis but aid in
assessing the severity and complications of the
ongoing infection.
PfHRP2 dipstick or card test: monoclonal ab captures
the parasite antigens. Only for falciparum malaria.
LDH dipstick or card test
17.
18. Drugs used to treat Malaria-First group
• CHQ, Amiodaquine
• Quinine, Quinidine
• Mefloquine, Halofantrine
• Lumefantrine
19. Drugs used to treat Malaria-others
• Clindamycin
• Azithromycin
• Proguanil
• Dapsone
• Primaquine
20. How to select antimalarials
Type of malaria – vivax or falciparum?
Sensitive or resistant
Associated renal or liver damage
Associated metabolic-electrolyte imbalances
Pregnancy, weight
Drug reactions
Oral therapy possible?
21. Intravenous anti-malarial therapy-
Indications
Presence of vomiting
Inability to start oral therapy may also be due to
altered mental alertness and seizures.
Patients who are intubated and on ventillators.
Those who are critically ill.
22. Intra-venous therapy
Chloroquine: intravenous 10 mg/kg max 600mg
over 6-8 hrs followed by 15mg/kg max 900mg
over next 24 hrs as slow infusion.
Quinine : intravenous 20mg/kg over 4 hrs; then
10mg/kg(max 600mg)three times a day.
23. Intra-venous therapy-severe f.malaria
Artesunate 2.4mg/kg stat; followed by 2.4mg/kg at 12
hrs, 24hrs and then daily. OR
Artemether 3.2mg/kg stat im; then 1.6mg/kg od im.
PLUS
Add quinine 20mg salt/kg over 4 hrs; followed by
10mg/kg over 2-8 hrs slow infusion thrice a day.
PLUS
Doxy 100mg bd / tetra 250mg (4mg/kg) qds
24. Multidrug resistant malaria- 2nd line
Doxy 100mg bd (3mg/kg x 7 days)
Artesunate 2mg/kg od or quinine 10mg/kg tds
PLUS
1 drug of the following:
Tetra 250mg qds (4mg/kg qid x 7 days)
Clindamycin 10mg/kg bd x 7 days or
atovoquone-proguanil 20/8 mg/kg od x 3 days
26. chemoprophylaxis
• Chloroquine 5mg base/kg (max 300 mg) once a
week. Begin 1-2 weeks before travel, during stay and
continue till 4 weeks after returning from malarious
area.
• Mefloquine 5mg salt/kg (max 250 mg) once a week.
Regime same as above.
• Atovoquone/proguanil (250/100mg) 1 tab for travel
to resistant malarious area beginning 1-2 days before
travel and taken daily during stay and ctd till 1 week
after return from malarious area.