![Team approach to preventing drug related errors ,[object Object],[object Object],[object Object],[object Object],[object Object],[object Object],[object Object]](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommandé
Recommandé
Contenu connexe
En vedette
En vedette (17)
Similaire à Mediation safety - Third Lecture
Similaire à Mediation safety - Third Lecture (20)
Plus de Kurt Wilson
Plus de Kurt Wilson (10)
Dernier
Dernier (20)
Mediation safety - Third Lecture
- 6. Team approach to preventing drug related errors
- 8. Voting
- 12. How would I deal with this?
- 17. What would be the safest and quickest way to confirm the correct dose?
- 18. What would be the safest and quickest way to confirm the correct dose?
- 19. What would be the safest and quickest way to confirm the correct dose?
- 20. What would be the safest and quickest way to confirm the correct dose?
- 21. What would be the safest and quickest way to confirm the correct dose? Confidence 1 2 3 4
- 22. What would be the safest and quickest way to confirm the correct dose? Phone the GP surgery to confirm dose? Ask patient to confirm dose? Check patient own medication to confirm dose? Look in case notes for recent letter from RA clinic to confirm dose?
- 23. Pharmacy Stamp Age D o B 21/1/54 Name (including forename and address) Alice Major 1 High Street Anytown Dispenser’s Endorsement Number of days’ treatment N.B. Ensure dose is stated NP Pricing Office Pack & Quantity Methotrexate 10mg Daily (4) Signature of Prescriber A Doctor Date 6/4/00 For Dispenser No. of Prescns. On form A Doctor A Surgery Anytown NHS PATIENTS – please read the notes overleaf FP10C 0899
- 24. Pharmacy Stamp Age D o B 21/1/54 Name (including forename and address) Alice Major 1 High Street Anytown Dispenser’s Endorsement Number of days’ treatment N.B. Ensure dose is stated NP Pricing Office Pack & Quantity Nystatin oral suspension 1mL QDS (OP) Chlorhexadine 0.2% mouthwash 10mL BD (300mL) Clotrimazole 1% cream BD (OP) Signature of Prescriber A Doctor Date 6/4/00 For Dispenser No. of Prescns. On form A Doctor A Surgery Anytown NHS PATIENTS – please read the notes overleaf FP10C 0899
- 25. Background ENT
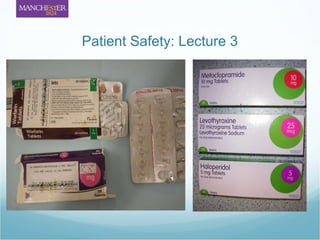
- 26. Methotrexate
- 34. 'Tweeting' medics expose patients “ Patient confidentiality is paramount and medical students and doctors obviously need to be very careful about any information they post online” A British Medical Association spokesman BBC NEWS / NEWS FRONT PAGE "You must make sure that your conduct at all times justifies your patients' trust in you and the public's trust in the profession." General Medical Council “ content may risk violation of patient privacy, even without using names or other identifiers” http://news.bbc.co.uk/1/hi/health/8266546.stm (24.09.09)
- 37. How to upload assignments
Notes de l'éditeur
- In this module we have given you an overview of the scale of medication errors and the range of errors that can occur. National systems are in place to help minimise errors (e.g. restriction of staff permitted to administer intrathecal medication) NPSA. The remainder of the module is allowing you to develop an approach to identify and minimise errors when you are a practicing health care professional.
- Back in the first lecture we showed you the common drugs implied with drug related errors at a local Trust and the types of errors which commonly occur. Drug related errors can occur at any stage of the medication process. Each healthcare professional has a responsibility to maximise their role in helping prevent medication errors. Many roles in today’s NHS overlap, but each professional should practice to minimise medication errors from: Selection - most effective and safe Prescribing – clear instructions and monitoring plans
- Dispensing – safe practice, clear lines of communication to clarify issues identified
- Administration – clear instructions from the prescriber and dispensing process (e.g. infuse over X no of minutes on label and on prescription) Monitoring – clear roles for all health care professionals – MTX (FBC), Opiates (RR), Gentamicin (TDM) Special kardexs for warfarin so INR is monitored. Nurse knows not to administer unless dosed. Community pharmacists check yellow anticoagulant book before dispensing to unsure monitored).
- As a team it is all our responsibilities to minimise drug related incidents. An error at any of these stages could present as patient harm. We should all be alert for drug related errors and act when we see one, put into practice procedures to minimise the risk.
- Last week we gave you a case with some options to vote on and your confidence on your vote. Here are the results from the medicine and pharmacy cohorts. The confidence is…..
- Do you remember the tap analogy from week 1? Some things that we are asked about are easy for us to answer with confidence. For example, think of this problem: A glass is being filled from the tap. Unfortunately, the glass is left under the tap and the water starts to overflow in to the sink. In your opinion, which of the following options would be best to deal with this situation effectively and keep your hands dry whilst doing so?
- Most people said they would go for option A, and be pretty sure they had made the right decision. And they were pretty confident with their choice of turning off the tap. What if when you tried to turn off the tap, the water flow continued. Your strategy to approach the problem changes as you gather additional information. As you approach a situation you need to continually reassess the information presented which may change your management strategy. Your options here might change and so might your monitoring. If a patient with RA presented your initial treatment may be an NSAID. By talking to the patient you may find that the patient has a contra-indication to the NSAID and your choice of options may change. The patient may have a caution to the NSAID and your monitoring frequency would probably change. You may even change your choice of NSAID to choose one to minimise the risk to that caution. As you gather information your options will change as will your confidence – you need to adopt a style of prescribing / monitoring to ensure you build in safety as you gather information.
- Today we have a case of a patient on methotrexate. This patient was started methotrexate for RA by the hospital (the hospital was responsible for the dosing and monitoring, the GP for the prescribing). Shared care arrangements are put in place for the prescribing and monitoring of MTX. Patient is increased according to tolerance and response to 17.5mg weekly over a 6 month period. The patient took 7x2.5mg tablets each week. Patient is admitted to hospital for an elective right knee replacement (Jan 2000). The following kardex is written. Patient is admitted for 8 days.
- Any issues with this prescription? You might want to have a look at this week’s BNF extract regarding methotrexate…
- (hopefully ID dose is incorrect – why? Methotrexate for RA is issued in 2.5mg tablets to prevent confusion with 10mg tablets used for chemo) What would you do about it? – clarify dose
- You have identified the dose – how would you find out the correct dose? Phone the GP surgery to confirm dose?
- You have identified the dose – how would you find out the correct dose? Ask patient to confirm dose?
- You have identified the dose – how would you find out the correct dose? Check patient own medication to confirm dose?
- You have identified the dose – how would you find out the correct dose? Look in case notes for recent letter from RA clinic to confirm dose?
- A Phone the GP surgery to confirm dose B Ask patient to confirm dose C Check patient own medication to confirm dose D Look in case notes for recent letter from RA clinic to confirm dose Are you confident that your chosen action will find the correct dose?
- Have a brief discussion with your neighbours… can you think of pros and cons to each option?
- The error goes un-noticed. 4 months later (April 2000) at the end of a routine appointment the Patient asks GP to prescribe MTX in a way which involves less tablets like when she was in the hospital. The following prescription is issued which is dispensed by a community pharmacy. Any issues? Changed to daily. How did the error occur? Communication error with patient and data entry error. What could be done to prevent it? Under shared care protocol GP would not change dose without consultation with hospital. Pharmacy computers would flag this dose up which must have been overridden.
- GP identifies error on prescription at next issue and corrects prescription (not on computer record). 8 days later patient contacts GP of feeling unwell. The following prescription is issued. Any issues / points for discussion? Should the pharmacist & doctor have identified these symptoms as a side effect of MTX. Were the notes accessed?
- 18 th April 2000: admitted to ENT ward. Fax of history not received by admitting doctor Clerked in using PODs Any issues? Incorrectly clerked in compounding error. Nurse gives 10mg dose daily but prescription not corrected. Hospital pharmacy do not service ENT wards, prescription arrives in dispensary – asks nurse to ask doctor to confirm with surgery. 10mg daily confirmed by non medical member of staff at GP surgery. 21 April patient deteriorating. Bloods taken on admission insufficient for blood counts and not performed. 22 nd April Bloods chased. Reveal extent of methotrexate overdose – low platelets and WBC. Transfer to haematology – patient dies 8 days later (GI haemorrhage, pancytopenia, methotrexate toxicity.
- This is not a ficticous case – this is a true account of an incident in Cambridgeshire in 2000. Since 2004 the NPSA have received Of the 165 reports of incidents directly associated with oral methotrexate • 139 (84 per cent) occurred in general or acute hospital settings and 26 (16 per cent) occurred in primary care settings*; • 140 caused no harm to the patients involved, 13 caused low harm, eight caused moderate harm, two caused severe harm and two led to the patients’ deaths;
- Also specific guidance on prescribing and administration.
- How did you vote? Option A – the ENT doctor phoned the surgery and confirmed a dose of 10mg Daily Option B – The patient was confused or poorly informed about their methotrexate Option C – The 10mg daily dose was dispensed Option D – May not have been in the same hospital for their appointments but knowing a shared care arrangement was dosed at the hospital the true dose may have been obtained. Know the limitations of the resources you use. Know the high risk drugs. Know the ADRs, cautions and contraindications of drugs you prescribe. Have an understanding of the errors which can occur and why they occur. Keep informed of NPSA alerts.
- This case is an example of the Swiss cheese effect. Numerous healthcare professionals had an opportunity to intervene before it was too late – GP, community pharmacy, ENT doctor, nurse, hospital pharmacist. In this module we are going to get you to identify the barriers to put in place prevent ‘the Swiss cheese phenomenon’ to improve patient safety
- So how does the rest of the module work? On the VLE (virtual learning environment) Blackboard you will find your group and case allocation. We have divided you into small groups of 5 students.
- From now until 9 th november The case study is a patient who has the potential (or has experienced) many patient safety incidents related to medication. You are looking at the patients complete life using resources from primary and secondary care including clips of interviews with either the patient or carers. This is similar to the methotrexate incident review board who after the incident looked at all the times the incident could be prevented to perform a route cause analysis of the incident to help prevent similar cases in the future. The resources are on BB. You need to identify the drug problems in the case and attempt to find the root cause of each problem. As a group you must agree an action plan to deal with the problems. You should explain your rationale behind your actions. You may discuss several actions but the group must agree one approach and back up that choice. The debate in deciding the agreed decision will be enlighting as in practice you have to take one course of action until further information is presented. You also need to indentify potential drug safety problems and decide on how to monitor these in the patient. Once you have completed this as a group you need to reflect and consider generic lessons learned and what actions can be implemented to improved patient drug safety for other patients. For example in the MTX case (potential problems before the critical incident) 1. Patient has RA and prescribed potentially toxic medication of methotrexate with complex administration regimen. Mechanisms to prevent: NPSA alert on weekly administration of MTX to all HCP and use of 2,5mg tablets only for RA Shared care protocol with monitoring and prescribing arrangements Use of methotrexate cards to keep patient informed with blood monitoring (plus patient counselling)
- Identify and collect materials from blackboard Discuss the case Pharmacy students have a scheduled slot on Thursday afternoons to discuss with each other & academic staff Message board use – open to all professions – can post questions (check medics access to BB) You will need to work as a group to produce a brief report Timeline- provisional report Feedback Final report and question and answer session
- PC with internet access in the lecture theatre and SHOW them blackboard/message boards/google/twitter? Consent to share emails
- Medics posting messages on networking websites like Facebook and Twitter are breaching patient confidentiality, a leading journal reveals. Research in the Journal of the American Medical Association found examples of web gossip by trainee doctors sharing private patient stories and details. Over half of 78 US medical schools studied had reported cases of students posting unprofessional content online. "Sharing patient stories that are de-identified and respectful, as health professionals might do on personal blogs, can encourage reflection, empathy and understanding. "However, content may risk violation of patient privacy, even without using names or other identifiers," they warned. elect privacy settings on social networking sites and should be told to perform periodic Web searches of their own name to vet listed online content. If you opt to use Twitter, bear confidentiality in mind.
- For pharmacy student we need to decide on a weighting of this report The marks allocation will be assigned to constructive, realistic etc. Example of feedback statements (well written/useful and poory written/not useful)? use description not judgement keep it friendly identify and reinforce strengths collect objective evidence collaborate on constructive solutions not capitulate on the standards. Do not let your own prejudice affect feedback Describe the impact
- Tell students about the afternoons when we are available for drop in support? Also, Brian Pollard has agreed to come along to the final question and answer session. This will make it very popular with the medics, as he is happy for us to let them know that he is heavily involved in 5 th year assessment in pharmacology, practical prescribing, medication safety and therapeutics, and their exempting exams (i.e. qualification) are in January!
- In the module in BB Click on the left course tools ‘discussion’ Click on drop box for correct weeks assignment Create message Label with correct group name and profession Click on add attachment
- Develop a problem solving approach to dealing with medication-related patient safety issues Access appropriate medicines information reference sources Review patient specific information (e.g. medical history, laboratory test results, interview transcripts) as an aid to decision-making Devise a patient-centred plan to optimise care