
Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
Similaire à Occlusal trauma
Similaire à Occlusal trauma (20)
Dernier
Dernier (20)
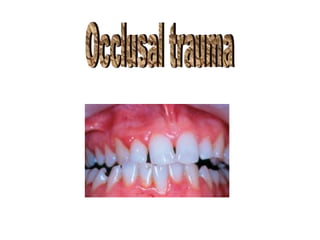
Occlusal trauma
- 2. Definition: Occlusal trauma :- injury resulting in tissue changes within the attachment apparatus as a result of occlusal force (s).
- 3. Primary occlusal trauma :- injury resulting in tissue changes from excessive occclusal forces applied to a tooth or teeth with normal support. It occurs in the presence of:1- normal bone level 2- normal attachment level 3- excessive occlusal force (s).
- 5. Secondary occlusal trauma :- injury resulting in tissue changes from normal or excessive occlusal forces applied to a tooth or teeth with reduced support . it occurs in the presence of :1- bone loss. 2- attachment loss. 3- normal / excessive occlusal force(s).
- 7. Histological studies : The histological features of occlusal trauma have been studied extensively in animal . and human autopsy materials Alteration of the periodontium that have been associated with occlusal trauma will vary with the magnitude & direction of applied force and location (pressure versus tension). These changes many include:, widening / compression of the periodontal ligament ( , bone remodeling (resorption /repair ,hyalinization-necrosis , increased cellularity ,vascular dilatation / permeability , thrombosis root resorption and cemental tears
- 10. Despite isolated reports of apical migration of junction epithelium accompanying excessive occulsal forces , studies generally have failed to disclose associated pocket formation while demonstration remarkable stability of the sharpey,s fiber and periodontal fibers coronal to the alveolar bone. In the absence of existing inflammation , it was noted that bony changes accompanying occlusal trauma may be reversed by discontinuing offending occlusal force.
- 14. Clinical studies Clinical indicators include :1- mobility ( progressive). 2- occlusal prematurities. 3- thermal sensitivity. 4- wear facets. 5-muscle tenderness. 6- fractured teeth. 7- migration of teeth.
- 16. Radioqraphic indicators :1-Discontinuity and thickening of lamina dura . 2- widened periodontal ligament space 3-evidence of root resorption and or bone loss
- 21. How to diagnose trauma from occlusion?
- 22. 1-history: a-teeth which are sensitive (not related to recession,caries,or broken fillings). b-muscle pain c-problems with TMJ (clicking,limitation in opening,or deviation).
- 23. 2-examination: a- attrition of teeth there are 2 different types of bruxism(clenching,grinding). b-decrease in vertical dimension. The functional attrition is normally compensated by continuous deposition of cementum in the apical area which differs from bone in that it has no resorption. c-some teeth with edges chipped. d-broken restorations. e-mobility of teeth(without periodontal disease or bone lesion). f-changes in position of teeth g-signs &symptoms of pulpal hyperemia or pulpitis without any obvious This could develop to pulpal necrosis then develop to peri apical lesion. cause.
- 24. • 3- x-ray;periapical x-ray Widening in space of pdl
- 25. 4- occlsal analysis a-impression-cast-bite registration-mounted on fully adjustable articulater.the analyze occlusion and determine area of premature contact. b-occlusion indicater
- 26. Treatment; not every trauma from occlosion require treatment just keep these patient under observation. We should not change the pattern of occlusion unless we are sure that pattern is causing the problem. For example; sometimes the cause is the muscles[uncoordinated] so no matter how much we trim the teeth we wont solve the problem.
- 29. Treatment; 1-interfering hopeless tooth-extraction. 2-new restoration of interfering teeth. 3-diminshed occlusal table require placement [bridge,partial denture….] 4-bite plane,night guard,now called [inter-occlusal appliance] a-prevent teeth from fully interdigitating. b-help in preventing or minimizing isomeric contraction of muscles. c-abolish the effect of mechanoreceptors. 5-exercise for more harmonious occlusion. 6-portable electromyography contain warning system[feed back] measures the electric potential on the muscles.
- 32. THANKS