
Recommandé
Contenu connexe
Similaire à Inorganic chemistry Chapter 1.pdf
Similaire à Inorganic chemistry Chapter 1.pdf (20)
Dernier
Dernier (20)
Inorganic chemistry Chapter 1.pdf
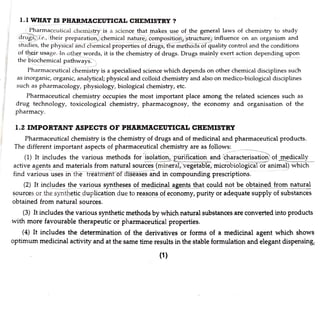
- 1. 1.1 WHAT IS PHARMACEUTICAL CHEMISTRY ? Pharmaceutical chemistry is a science that makes use of the general laws of chemistry to study drugs i.e., their preparation, chemical nature, composition, structure) influence on an organism and studies, the physical and chemical properties of drugs, the methods of quality control and the conditions of their usage. In other words, it is the chemistry of drugs. Drugs mainly exert action depending upon the biochemical pathways. Pharmaceutical chemistry is a specialised science which depends on other chemical disciplines such as inorganic, organic, analytical; physical and colloid chemistry and also on medico-biological disciplines such as pharmacology, physiology, biological chemistry, etc. Pharmaceutical chemistry occupies the most important place among the related sciences such as drug technology, toxicological chemistry, pharmacognosy, the economy and organisation of the pharmacy. 1.2 IMPORTANT ASPECTS OF PHARMACEUTICAL CHEMISTRY Pharmaceutical chemistry is the chemistry of drugs and of medicinal and pharmaceutical products. The different important aspects of pharmaceutical chemistry are as follows: (1) It includes the various methods for isolation, purification and characterisation) of medically active agents and materials from natural sources (mineral, vegetable, microbiological or animal) which find various uses in the treatment of diseases and in compounding prescriptions. (2) It includes the various syntheses of medicinal agents that could not be obtainedfrom natural sources or the synthetic duplication due to reasons of economy, purity or adequate supply of substances obtained from natural sources. (3) It includes the various synthetic methods by which natural substances are converted into products with more favourable therapeutic or pharmaceutical properties. (4) It includes the determination of the derivatives or forms of a medicinal agent which shows optimum medicinal activity and at the same time results in the stable formulation and elegant dispensing (1)
- 2. ganic Vol- Pharmaceutical Chemistry (Inorganin 2 (5) It includes the determination of chemical and biological incompatibilities among the ingredients of a prescription. the various and (6) It helps in the establishment of safe and practical standards with respect to both dosas quality in order to maintain uniform andtherapeutical standards for all torms of medication tion hg (7) It helps in the improvement and promotion of the use of chemical a8ents for preventi ilness, alleviation ofpain,cure of diseases and search for new therapeutical agents especiallv there exists no satisfactory remedy. when 1.3 INORGANIC PHARMACEUTICAL CHEMISTRY inorganic substances as drugs, i.e., their preparation, chemical nature, compoSition, structure,influe on an organism, etc. Inorganic pharmaceutical chemistry is a science that makes use of the laws of chemistry to s ence The main source ofinorganicdrugs happens to be the natural source such as minerals. There many reports on the use of minerals in medicine. Some interesting examples of these include miners waters, salts, partially purified inorganic chemicals, calcined inorganics (ash or bhasma), and chemical. transtormed inorganics. At a later stage, many of these were found to be poisonous substances but ars being still used cautiously by some doctors in sufficiently small quantities. Thus, the ancient physicians were quite familiar with the use of antimony, arsenic and mercury. are re are In ancient Indian medicine system mercury was supposed to occupy a dominant position for sometime and whole treatises were written giving its therapeutic and other properties. Many noble metals like gold and copper were also used in medicine. The use of minerals as medicinal agents were not restricted to any single country but all ancient cultures were quite familiar with their medicinal uses. Although many inorganic chemicals are rarely employed today, yet few inorganic chemicals are being still used in modern medicine. Synthetic organic chemicals are able to replace the more toxic inorganic pharmaceuticals. Most of these belong to one or other of the following categories: (1) Those that find use for replacing or replenishing the normal content of the body. These are required for normal physiological processes and are required in diet. But disease conditions are able to deplete their amounts in the body. Hence they have to be replenished or replaced. Calcium, sodium potassium, magnesium, iron, chloride, phosphate, bicarbonate, oxygen, etc., are examples of this category. (2) Those that are used for changing reactions of body fluids, ie, acidify or alkalise. Mineralacids antacids, alkalis etc., belong to this category. (3) Those that find use as medicinal and therapeutic agents in disease conditions. These may be able to change physical (eg., topical agents, protectants), physiological and/or biochemical processes (eg astringents, respiratory stimulants, hypnotics, expectorants). Some may be used as correctives or n infections (eg., dental products, antidotes, antimicrobials etc.). (4) Those that find use as pharmaceutical aids. Bentonite, talc, antioxidants, pigments etc. are example of this category. (5) Those that find use in analytical and quality control processes. Most of inorganic chemica included in the Pharmacopoeia belong to this category. Titrants such as permanganate, dichromat iodine, bromate etc., buffers like phosphoric acid salts, boric acid salts, ammonium salts etc. are useru examples of this group.
- 4. 4 Vol-I P h a r m a c o u t l o a l ChomistrY (Inorgania v. O 1S based on the published information divided in different major parts. zaenn Part comprised of chapters. Part I generally brings together drugs that have similar use or actions af the chapters are w to guide the reader to the drug that may be of interest in related chapters. MOs m ences are us wili c o n providing background information on that group of drugs having iary comn, actions. Fart Il includes monographs on new drugs, on drugs under investiga dSSea, and on obsolescent drugs still of interest. Jt also provides details regarding e n e e s o tequire drug therapy. Part m, in this publication gives composition of the proprietary meaic orH Public in differernt countries and ae generally described by the manufacturers. rne been omitted. u y the pharmaceuticals which are commonly and currently in use are inCiuaed 1n the plarmacopoeia. The substances which are found to be undesirable from past experience and wich are y not in use are excluded. The chemicals which are used for application or internal coisumption Dy n u m a n beings, form the part of pharmacopoeia, The chemicals which are commerclauy avallaole in Pure state and which are commonly used for other p u r p o s e s are excluded. In the pnartldoPela only m i n i m u m standards for a chemical are prescribed. However the manufacture may supPPY u e s e with re sngent standards. Thus a medication has to comply strictly with any one of the pharmacopoeias n o t it may be considered substandard and usuallynotprescribed by standard medical practitioners. Only those mentioned in the pharmacopoeia are considered official as per the legislation ot thecountry 1.5 HISTORY OF P H A R M A C O P O E I A Every country has legislation on pharmaceutical preparations that sets standards and obligatory quality indices for medicaments, raw materials, and preparations employed in the manufacture of drugs. These regulations are presented in separate articles-general and specific relating to individual drugs, and are published in the form of a book called a Pharmacopoeia. The word Pharmacopoeia is derived from the Greek words pharmakon, a drug or medicine and poieo, to make. The first British Pharmacopoeia (B.P.) was published in 1864. It was including monographs on benzoic acid, gallic acid, tartaric acid, tannic acid, camphor, lactose, sucrose and seven alkaloids along with their salts. The first United State Pharmacopoeia (U.S.P.) was released on 15th December, 1820. Indian Pharmacopoeia In India, in the pre-independence days, B.P. was employed as the official book of standards. The first edition of the Indian Pharmacopoeia (I.P.) was published in 1955. It was having a large number of crude drugs and their preparations. The third edition of the I.P. got published in 1985. Addendum Ito third edition has been published in 1989. The Addendum I to the Pharmacopoeia of India 1985 amends the Indian Pharmacopoeia 1985 and constitutes a part of Indian Pharmacopoeia, third edition. The General Notices and Appendices included in the Indian Pharmacopoeia 1985 and as amended in this Addendum apply both to the matter contained in the Indian Pharmacopoeia 1985 and to the matter contained in this Addenduun.
- 5. Introduction to Pharmaceutical Chomistry In India there are laws dealing with certain of the substances which are the subject of monographs which follow. These monographs should be subject to the restrictions imposed by those laws wherever they are applicable. It is expedient that enquiry be made in each case in order to ensure that the provisions of any laW are being complied with. In general, the Drugs and Cosmetics Act, 1940, the Dangerous Drugs Act, 1930, and the Poisons Act, 1919, and the rules framed thereunder should beconsulted. Under the Drugs and Cosmetics Act, the Indian Pharmacopoeia is the book of standards for drugs incuded therein and the standards as included in the Indian Pharmacopoeia would be official. If considered necessary these standards can be amended and the Secretary of the Indian Pharmacopoeia Committee is authorised to issue such amendments. Whenever such amendments are issued, the Indian Pharmacopoeia would be deemed to have been amended accordingly. The Govermment of India constituted a permanent Indian Pharmacopoeia Committee in 1948 for the preparation of the Indian Pharmacopoeia and keeping it up-to-date. The first edition of the Indian Pharmacopoeia was published in 1955, followed by a supplement in 1960. The second edition of the Indian Pharmacopoeia and its supplement were published in 1966 and 1975 respectively. The third edition of the Indian Pharmacopoeia was published in 1985. Each later edition supersedes the previous one. There are also supplements (Addendum), on each in 1960, 1975, 1990 and 1992. In order to keep the Pharmacopoeia accurate, authoritative and up-to-date, the Ministry has established a Central Indian Pharmacopoeia Laboratory (at Ghaziabad) and an Indian Pharmacopoeia Committee. TheAddendum () to the third edition amends the Indian Pharmacopoeia 1985 and is published by Government of India, Ministry of Health and Family Welfare on the recommendationof Indian Pharmacopoeia Committee (in accordance with Drugs and Cosmetics Acts, 1940, Dangerous Drugs Act, 1930 and the Poisons Act 1919, and the rules framed thereunder). Indian Pharmacopoeia, 1996 2 volumes, 1182 p, figs. The latest edition of the Indian Pharmacopoeia was published in 1996. Underthe Drugs and Cosmetics Act, 1940, the Indian Pharmacopoeia is the legally recognised book of standards for the quality of drug substances and their preparations included therein. Contents: Volume I: Notices. Preface. Acknowledgements. Introduction. General notices. Monographs (A-O). Volume II: Monographs (P-Z). Infra-red reference spectra. Apperndices. Index. "The Indian Pharmacopoeia is the legally recognised book of standards for the quality of drug substances and preparations included therein. This new edition, which supersedes the 1985 edition and its addenda, includes many new drugs and their dosage forms and, omits others as also amends the specifications and updates standards of others keeping in view the advances in pharmaceutical sciences. "The contents are accommodated in two volumes as was the case with the earlier edition. It contains 1149 monographs and 123 appendices dealing with reagents and test procedures to be used for ascertaining compliance with the standards. Some new tests have been added. A special feature is the inclusion of infra-red reference spectra of a number of drug substances. The general notices, which
- 6. Pharmaceutical C h e m i s t r y ( I n o r g a n i c Vo in tinted provide the basic guidelines for the interpretation and application ofstandardsy paper to highlight this important part of the compendium. a p p l i c a t i o n of s t a n d a r d s , a r e printed acket) "The Pharmacopoeia is indispensable forallconcerned with the quality or arg y "The Addendum 2000 veterinary is a companion is indispensable for all concerned with the quality of drugs." (jac 1996 which volume to the Indian P h a r m a c o p o e i a . jacket) No. 19078 armacopoeia Addendum 2000 anmends as well as adds new drugs and j 1996 with a view to keeping the Pharmacopoeia existing monographs and appendices, it contains 44 new monograp undergone major amendments. The appendix on Bacter new version which includes the quantitative tests in additio p r e p a r a t i o n s to the Indian Phar updated to the extent possible. Besides amending raphs. Some m o n o g r a p h s har the have with a terial E n d o t o x i n s Test has been replaced wit tion to the c o n v e n t i o n a l gel clot test. "The veterinary Supplement2000to the Indian P h a r m a c o p o e i a 1996 is indispensable for all c o n c e r n e d with the quality of veterinary medicines." (jacket) No. 19079 "India has a huge livestock wealth. It needs me diseases in animals. As medicines for veterinary use cons armamentarium, it was thought appropriate to prepare details specifically for drugs and preparations meant 2000 is the first ever such publication. As it is an adjunct compendi 1996, standards for the quality of medicines included therein will have the same legal authority as those included in the Indian Pharmacopoeia 1996." m e d i c i n e s for diagnosis, prevention and t r e a t m e n t of c o n s t i t u t e a significant portion of the total drug a separate volume containing all relevant for veterinary use. The Veterinary Supplement endium to the Indian P h a r m a c o p o e i a "The monographs of the Venterinary Supplement 2000 are divided into two parts. Part I deals with non-biological preparations whereas Part II c o v e r s biological products. As the quality standards are the same for all medicines, whether used in humans or in animals, monographs of drugs and preparations included in this Supplement but already official in IP 1996 contain information on doses and strengths of dosage forms only." eir "Four appendices describe the details of procedures specifically for testing certain biological veterinaryproducts. The tests included in various appendices of the Indian Pharmacopoeia 1996 are to be referred to for other preparations. For ease of reference, the General Notices in the Indian Pharmacopoeia 1996, which are the key to the interpretation of the standards, are reproduced after editing suitably, and are printed on distinctive blue paper, as in the Indian Pharmacopoeia 1996." Constant collaboration between countries in the field of public health and drug production necessitated the establishment of common, unified requirements for the quality of drugs, and consequently, unified methods of analysing them. For this purpose, the International Pharmacopoeia was created. It is published under the auspices of the World Health Organization and is a collection of recommended requirements on drug quality. The International Pharmacopoeia is not a legal document for any country, but it provides the basis for establishing national requirements on drug quality. At present, the 2nd edition of the International Pharmacopoeia (published in 1968) along with the supplement to it (1971) are in use. Specialists of many countries took part in preparing the second edition of the International Pharmacopoeia. In 1981, the first volume of the 3rd edition of the International Pharmacopoeia was published. It includes the general methods of analysis. This book has been dealing with the study of inorganic substances, that have been official in the Indian Pharmacopoeia. The word 'oficial, normally represents what is official in I.P., B.P., U.S.P. and in anv other authoritative book of the country. All the important inorganic compounds that are official in I.P. and have been commonly used in pharmacy, have been described here.
- 7. Jol-I) o-I) nted Introduction to Pharmaceutical Chemistry In Pharmacopoeia, each pharmaceutical has been described under a monograph. The various standards described require other chemicals, apparatus, techniques, processes etc., which are not the subject of other monographs. All such items are again described in appendices to the Pharmacopoeia, with precise specifications for these necessities. For a pharmaceutical chemist and an analyst the apPpendices are considered as important as the main body of monographs. Only those pharmaceuticals which are commonly used in the recent past have been included in the Pharmacopoeia. Substances which have proved to be undesirable from past experience have to be removed from Pharmacopoeia. Substances which are commercially available in excellent purity and are commonly used for other purposes are also generally not included, due to redundancy. However, if such substances find use internally, then they are included in the monographs. The standards prescribed for a chemical are the minimum. It does not prevent a manufacturer from supplying these with more stringent standards. If a substance has not been included in the Pharmacopoeia, it does not imply that it cannot be used or marketed. Such non-official substances must correspond to standards prescribed either in the earlier editions of the Indian Pharmacopoeia or in other recognised Pharnmacopoeia (of other countries). In this country products corresponding to the British Pharmacopoeia (B.P.) and United States Pharmacopoeia (U.S.P) are generally marketed. Other better known Pharmacopoeias International Pharmacopoeia (1.P.),European Pharmacopoeia (E.P.) and U.s.s.R.P. To avoid confusion between Indian and International in the abbreviation, sometimes IND. P. or P.l. may be written for Pharmacopoeia of India. However, unless otherwise specified, in this country 1P. will be generally understood as Indian Pharmacopoeia. There are other compendia prescribing standards for pharmaceuticals. Some of these have been: British Pharmaceutical Codex (B.P.C.) and National Formulary (u.s.N.E.). Any substance which fails to correspond to any official standard should not be used, in the interests of proper health. hich eia the ave h a ned of ug ant ent eia as th ne ir Medicinal substances and pharmaceutical aids included in monograph of the latest edition of the Pharmacopoeia deem to be official substances in the country of Pharmacopoeia. It is of utmost inmportance to understand the difference between chemical individual and an official substance with same name. An individual chemical can be pure to any specified purity but the official substance isa commercial product which is required to comply with certain standards of purity specified in the Pharmacopoeia and may often have some other substances, added for specific reasons; for example Chloroform of the Pharmacopoeia contains 1-2% of added ethyl alcohol to prevent the formation, and to inactivate any poisonous phosgene (carbonyl chloride) gas that may be formed in contact with the air during storage. 2COC1, Carbonyl Chloride (phosgene) OCH CO OCH Official Substance eS al to er 2HC1 2CHCl O CI HOC,H 2HC CO Cl HOC,H (Diethyl carbonates (relatively non-poisonous) To specify, a particular compound/substance being official, the official name is specified with capital initials eg. Sodium Chloride, Aluminium Hydroxide. However, the reference/meaning is clear from the context, the capital initials are not employed/repeated unnecessarily.
- 8. Vol-l Pharmaceutical Chemistry (Inorganji 8 Pharmacopoeial Description/Presentation Mostly, all pharmacopoeias consist of the three main sections namely (a) Introductic a) Introduction : It is a useful pointer to pharmaceutical progress since last edition becau summarises the various changes/additions/deletions in the current edition. Attention should be tion includi General Notices; () Monographs of the official drugs; and (c) Appendices P later part OGeneral Notices" at the outset so as to avoid misunderstanding and misinterpPre of the text. 1o1 ) Monograph of Official Drugs, Preparations and Substances :The word O g P Imple the written study of a subject. "As the medicinal substances are to be used for the cure and or preventin of diseases, therefore, these are considered as very important and hence their written studies appear Monograyphs' in the Pharmacopoeia. For the convenience, the monographs are somewnat stereOtyped in style and the arranged in the alphabetical order of their names. The pharmacopocial monogrphs (fo example in LP. 1985) give the following information about the drugs and pharmaceutcal aids (1) Title: The title is stated in English and refers to the official name of the compouna. Sometimes sub-titles are given. These are synonyms and could be used in place of the main title eg, Calciur carbonate can also be called precipitated chalk, iron and ammonium citrate can also be called feri ammonium citrate; milk of magnesia can also be called magnesium hydroxide mixture. 2 Formula weight and molecular weight: Following the title has been the chemicalformula of the pure compound, with its molecular weight,eg, MgCl,.6H,O Mol. wt.202.30; KMnO, Mol.wt. 158.03 etc These two items are not given, provided the correct chemistry is not known or the compound is uf indefinite composition. For example, for iron ammonium citrate, formula and mol.wt. are not given. 3) Category: This describes the therapeutic or pharmacologic or pharmaceutical application of the compound. Usually this is the main application, although the compound may be having other applications. Some main categories for inorganic pharmaceuticals mentioned in the Pharmacopoeia include haematinic; antacid; laxative; pharmaceutical aid; astringent, etc. 4) Dose: These are the quantities for the guidance of the prescriber or the physician to achieve the desired therapeutic effects in adults. It can be altered as and when required, eg., CaCO, dose 1 to 5 gm. This is omitted for substances not used for internal administration. Usual strength may be given for pharmaceutical dosage forms, like injection etc., which is the most commonly marketed dosage strength. 5) Description: This gives a physical description of the substance like crystalline or amorphous nature, colour, odour, taste, etc. These properties help in the preliminary evaluation of the integrity of an article and not themselves the standards or tests of purity, eg, CaCO, fine, white microcrystalline powder, odourless, tasteless. t6) Solubility: Solubility is described in popular terms, which are defined in the Pharmacopoeia under general notices. This is usually 8iven in water, sometimes in hot or boiling water, in alcohol, in glycerol, in solvent ether and sometimes in other organic solvents, acids or alkalis. Colubility for an article given in the monograph may be considered primarily as information, but it it is given under the quantitative solubility test, then it 18 a standard. If the exact solubility of the article is not known, a descriptive term is used to indicate its solubility. The following table reveals the meaning of such term.
- 9. Introduction to Pharmaceutical Chemistry TABLE 1.1 Descriptive Terms Relative Quantities of Solvent for 1 part of Solute Less than 1 part From 1 to 10 parts From 10 to 30 parts From 30 to 100 parts From 100 to 1000 parts From 1000 to 10,000 parts More than 10,000 parts Very soluble Freely soluble Soluble Sparingly soluble Slightly soluble Very slightly soluble Practically insoluble '(7) Standard : It is an important part ofmonograph, which specifies the quantitative purity of the title compound, where the compound is of definite composition, e.g., (1) Potassium bromide is having not less than 98.0 per cent of KBr, calculated with reference to the dried substance, e.8, (2) Hydrogen peroxide solution is an aqueous solution of hydrogen peroxide. It contains not less than 5.0 per cent w/v and not more than 7.0 per cent w/v of H,O, corresponding to about 20 times its volume of available oxygen. It is having not more than 0.025 per cent w/v of a suitable stabilising agent. If the composition has been not definite, the standards are vaguely defined, e.g., (1) Bentonite is a natural, colloidal, hydrated aluminium silicate, e.g., (2) Dried aluminium hydroxide gel consists largely of hydrated aluminium oxide and varying small quantities of basic aluminium carbonate and bicarbonate. It contains not less than 47.0 per cent of Al,Og Standards stated in the monograph of the Pharmacopoeia apply only to articles which are intended for medicinal use and not to articles sold for other purposes, e.g., starch. (8) Identification: This usually involves specific chemical test or tests for identifying the substance. Colour reactions, precipitating tests, and gas evolving reactions are commonly used for inorganic pharmaceuticals. Identification tests are not absolute proof of identity. It provides a means of verification only, e.g., phenol. Phenol FeCl, solution gives violet colour. (9) pH: The pH values given in the monograph are for the guidance of manufacturing pharmacist to develop various dosage forms and to avoid physiological complications, e.g, calcium amino salicylate. 2 per cent w/v solution gives pH 6.0-8.0. (10) Limits for impurities: For different chemicals different limit tests have been included, as also different amounts of such impurities permissible for that chemical. The various tests that are included could be any of these: acidity or alkalinity, ph, specific impurities (like phosphates, sulphides, magnesium, Darium etc.), arsenic, heavy metals, chloride, sulphate etc. These will be dealt with in another chapter on Quality control and Tests of purity. Limit tests for impurities are generally represented in parts per million by weight (ppm) or as a percentage. These are approximate values. (11) Assay: It is a step-by-step description of a chemical analytical method for the active substance. If the assay method described in the Pharmacopoeia is applied to the chemical, the standards prescribed in the monograph earlier should be realised. For most inorganic pharmaceuticals, titrimetric or gravimetric methods are used.
- 10. rganic Vol- Pharmaceutical Chemistry (Inorganic (12) Storage: This is the last item under the monog the activity of the chemical. These are generally brief and general, Condition. For inorganic pharmaceuticals, the Pharmacopoeia uses thee e etc. this implies the substance is stable and gets protected from dust, airt Container, (b) tightly-closed containers; the substance in such cases Be or moisture or carbon dioxide (e.g., reducing agents, hygroscop e etc, it may also include sur iso incude such compounds as are volatile or contain dissolved gases etc. 1t compounds as are volatile or contain dissolved gases etc. (c) light-resi ce are arected by light are stored in amber or dark-coloured containers; (d) cool place; tnis is applicablet, Substances which are affected by warm climate (e.a.. thermolabile substances); for some solution reezin8 1s to be avoided; (e) single-dose containers:this is generally prescribed ror sonne njectable, which once opened, should not be used again. Precautions to be taken where there is a possibility of effect of atmosphere,moisture eservi, the monograph. These directions are useful in preser. ded more as guidance than a ting intot eric oxyy etc.); it m ubstances whi light s a possibility of effect of atmosphere, moisture, heat and lig ditiona are indicated where appropriate in the monog Protection against light is necessary, the bottle must further be covered with a black paper. e.g., Ferrous fumarate- Store in a light resistantcontainer. graph. In certain specified instances when additio .8, Insulin injection Store in multiple dose containers at a temperature between 2 to 8'C. It should not be allowed to freeze. 1.P.also prescribes conditions for the storage of some official substances which are likely to deteriorate, if not stored properly. The terms used under definite meanngs of the pharmacopoeia are: Terms Pharinacopoeial meanings Any temperature not exceeding 8° and usually between 2°C and 8° C. Any temperature betweern 8°C and 25°C. An article for which storage in a cool place is directed, may alternatively, be stored in a refrigerator (at temperature between 2°C and 8°C), unless otherwise specified in the individual monogrph. The temperature prevailing in a working area. Cold Cool Room Temperature Any temperature between 30°C and 40°C. Warm Any temperature above 40°C. Where no specific directions are indicated in the individual monograph, it is to be understood that the storage conditions include protection from moisture, freezing Excessive Heat Storage under non-specifie and excessive heat. (13) Appendices The General Notices and Monographs are followed by a comprehensive section of Appendices. The Appendix 1 describes the apparatus that are needed for various pharmacopoeial tests and assays. In particular the standards and tolerances tor Nessler's cylinders, thermometers, volumetric glassware and weights and balances are laid down in this Appendix. The Appendix 3 includes the details of various chemical tests and assays. Some physical tests and determinations like loss on drying, determination of pH, melting range etc. rorm part or Ppenaix >. Useful directions on cleaning glassware oscribed in Avpendix 6. Reagents and solufiorns needed in the various tests and assays, their method of preparation, standards etc. have been described fully in Appendir7 Th assays, .. in the Pharmacopoeia for weights ana measures ana ot elements and their atomic weights have been described in the Appendix 9. aQE hroadly includes following 91 categories of Appendices (with several sub-appendices)
- 11. Introduction to Pharmaceutical Chemistry 11 Appendix Number Number of Sub-appendices under each Appendix (3) Type ofAppendix (1) (2) 6 Apparatus for Tests and Assays Biological Tests and Assays Chemical Tests and Assays 41 29 3. 7 Microbiological Tests and Assays Physical Tests and Determinations 19 General Information 7. Reagents and Solutions . Reference Substances 9. Tables 2 1.6 EXTRA PHARMACOPOEIA (MARTINDALE) Although no explanations have been included in the Pharmacopoeia, it is having wealth of information. Anyone who consults the Pharmacopoeia often, should familiarise himself with the general notices and the various appendices. Most comprehensive information on every type of pharmaceutical or drug can be obtained from the Extra Pharmacopoeia (Martindale, 29th Edn.). This excellent work has been especially rich in therapeutic and clinical information on the drugs. There are several other useful literature references for inorganic pharmaceuticals. Some of these have been included at the end of this book. The Extra Pharmacopoeia was first edited, compiled and published in 1883 by William Martindale (1840-1902), a practising pharmacist. Its main aim was to provide physicians and pharmacists with practical and up-to-date information concerning drugs and gelenicals to supplement that was included in the British Pharmacopoeia. Four editions of "Martindale" were published in the span of three years. Up to 1910, the accumulation of information became so great that the subject matter had to be divided into two volumes. The first double-volume edition, the 15th, appeared in 1912. The copyright of the Extra Pharmacopoeia was acquired by the Pharmaceutical Society of Great Britain in December 1933, upon the death of Dr. W. H. Martindale, son of William Martindale, and since then the society is continuing to issue it under the editorship of the Director of its Department of Pharmaceutical Sciences. The 24th edition of volume I was published in 1958 and 23rd edition of Volume II in 1955. A supplement was published in 1961. The 25th edition appeared in February 1967 while the 26th edition was released in July 1972. Now the highly acclaimed Martindale (1993) now in its 30th edition, contains up-to-date authorative information on drugs and medicine in use throughout the world. It is written for the practising pharmacists and physicians and for all those involved in use of drugs and medicines. This new edition of Martindale has been markedly changed in order to meet the requirements of today's reader. These changes include a massive increase in formation on proprietary medicines, a significant shift to a more clinical emphasis, an increase in the number of referenced reviews, and shortening of the usual period between editions to meet the need for up-to-date information. 1.7 BRITISH PHARMACOPOFÍa The reason for the appearance of a British Pharmacopoeia is ascribed to the Medical Act of 1858, Section 54 which stressed the need of publication of a book having a list of medicines and compounds,
- 12. Pharmaceutical C h e m i s i y ( L n o r g a n i c V they are Vo.-i 12 poeia, 1864 w a s a n o u t c o m e of the comi rmacopoeia Londinensis (1618), oeia (1807). New e d i t i o n s and a d d e n d u m foll dendurm n in 1874, a 3rd e d i t i o n in 1885, a f u r t h e r adde weights and measures by w h i c h mbinatior the m a n n e r ofpreparing them, together with true prepared and mixed. The First British Pharmacopo three old and reputed Pharmacopoeias namely Pharn Pharmacopoeia (1699) and Dublin Pharmacopoeia (18 quick succession, the 2nd in 1867, an addendum in 1890 and a 4th edition in 1898. Edinbu followed Preparations ar The British Pharmacopoeia 1864 included separate parts: Materia Medica and P r e p a r a t i o n s a parts: M a t e r i a M e d i c a and Compounds. In the 1867 edition the contents had been several other Pharmacopoeias. ad been arranged a l p h a b e t i c a l l y as per A gap in revision delayed the next edition until 1914. he technic: oeia 1914 it w a s r e a l i s e d that the In Britain after publication of the British Pharmacopoe. complexity of the drug sepecifications was increasing prepare the Pharmacopoeias. As such in 1928, the became responsibility of the C o m m i s s i o n . It was ther ng and a d i f f e r e n t kind ofset up w a s needed onwards led heBritish P h a r m a c o p o e i a from 1932 edition and. P. must be revisec hen r e c o m m e n d e d that the B.P. every ten years. n 1952 revision, a range of diagnostic materials was included. An important a d d i t i o n was made t: n c l u d e s t a n d a r d s and tests for antitoxins and insulin. The interim between 1932 and next 7th edition 1948, was covered by s e v e n addenda. In 7th edition of1948, generic n a m e s were provided for substances newly i n t r o d u c e d into medicine. Methods of analysis, disintegration tests for tablets and sterilization methods were expanded. Manynew monographs related to penicillins and sex h o r m o n e s w e r e included At this time, it was decided that the normal interval between new editions should be five instead of 10 years, due the rapid pharmaceutical and pharmacological progress that had been made. The next edition appeared in 1953. The titles of drugs and preparations w e r e given in English instead of Latin. A b b r e v i a t e d Latin title was retained as a synonym. Capsules, constituted as new group. The implant methods for sex hormones and their standards were described. The 9th edition (1958) was having 160 new monographs. Tranquilising drugs and s p e c t r o p h o t o m e t r i c analysis were added. The tenth edition appeared in 1963. In Medicines Order 1970, the duties of the British Pharmacopoeia Commission were defined. The thirteenth edition of British Pharmacopoeia (1980) was the first edition of Pharmacopoeia that was prepared strictly under the provisions ot Medicines Act. Currently the British Pharmacopoeia starts publishing in two volumes due to an expansion of drug information. The British Prarmacopoeia (1993) has provided authoritative standard for the quality of many substances, preparations and articles used in medicine and pharmacy for some 130 years. This new edition consolidates and extends the 1988 edition with its 1989, 1990, 1991 and 1992 addenda, and for the convernience for the user also incorporates tne monographs of the European Pharmacopoeia. Volume I deals with medicinal and pharmaceuical substances. It also includes the infrared reference sDectra needed for the identification of manyorthe materials. Volume II contains sections on formulated ducts, radio-pharmaceutical preparations and. surgical preparations, blood products, immunological produ n a t e r i a l s . addendum to the British Pharmacopoela 193 includes monographs for a substantial of substances and preparations tor the irst ime. Also included are the followino:
- 13. 13 Introduction to Pharmaceutical Chemistry Several new European Pharmacopoeia monographs, revisions to monographs, edited texts relevant to the human medicine that have been published fascicule 17 of the second edition of the European Pharmacopoeia, replaces the limit test for particulate matter. An indication of the approximate levels of impurities controlled by chromatographic tests wherever appropriate. A new supplementary section containing auxilliary material of relevance to users of the Pharmacopoeia. 1.8 EUROPEAN PHARMACOPOEIA European Pharmacopoeia is regarded to be an official book of standards adopted by Germany, France, Italy, Netherlands, Switzerlandand Belgium. Council of Europe issued an order in July, 1964 to frame out European Pharmacopoeial Commission for compiling European Pharmacopoeia. The first edition of European Pharmacopoeia appeared in 1969 and its official standards become applicable within the respective member countries. The second edition is being published in a series of volumes. 1.9 PHARMACOPOEIA INTERNATIONALIS (INTERNATIONAL PHARMACOPOEIA) There appears to be no uniformity in terminology and strengths of pharmaceutical preparations used in various countries. As early as 1874 view had been expressed that some world uniformity in the standards for potent drugs must prevail. These views got further support at an international conference in 1902 and an agreement was framed. No progress was achieved until a second international conference got held in 1925 where an International Agreement on the Unification of Formulae for seventy-seven potent drugs and preparations got reached. The Health Organisation of the League of Nations established in 1936, a Technical Commission of pharmacopoeial experts. After the World War II over in 1946, the work was undertaken by the World Health Organisation. Volume I of the long-awaited Pharmacopoeia was finally published in 1951, in Latin, with translations into English and French. It was having monographs for over two hundred drugs and chemicals; with appendices on reagents, tests and biological assays. The Volume IL, published in 1955 included formulae for preparations having various drugs and substances already present in Volume I. The supplement of 1959 incorporated some newer drugs and substances with the method of preparations and the appropriate tests. The second edition got published in 1967, followed by a supplement in 1971. The third edition got published in the form of several volumes, Volume I appeared in 1979. Although the International Pharmacopoeia cannot be imposed legally on any country, the pharmacopoeial authorities of all countries are expected to give due considerations to its standards so as for achieving uniformity of standards as far as practicable. 1.10 UNTTED STATES PHARMACOPOEIA (USP) In 1817,Dr.Lyman Spalding of New York proposed a plan to the Medical Societyof the Country at New York for publishing a National Pharmacopoeia. The first edition ofUnitedStatesPharmacopoeia was compiled, edited and published on 15th December,1820 which was having 217 drugs in about 272 pages.Subsequent editions of USP appeared after the gap of ten years. In 1905, the nineth edition of USP was published. However, it was given the title of USP VIII, as to show that it was eighth revision. USP considers 25°C as the standard temperature for specific gravity and solubility statements. The 1940 Convention directed that the Pharmacopoeia must berevised every 5 years. On July 5, 1974, unification of the USP and NF (National Formulary) was announced. Since then the subsequent editions consolidate USP and NF into a single volume. All drug substances and drug products were covered in USP whereas NF is devoted exclusively to pharmaceutical ingredients. The XXII edition of USP combined with XVII edition of NF was published in January, 1990.
- 14. corporates upd etd ehology that are relevant to the development Sourceup nd provisio of me sugport ior the cortinuing education of graduates, with speial emphasis s 12thedition has ben completely revised and ireh suyect areas.The new Codex provide a reference source on all as eutics and demonsy nd use. The nes from conception and development to production and ergraduates ard s Per covers the multidisaplinary natureof pharmar 12 and th e phermaceytics content of the syllabus for pharmacy prepa three pharmaceutical data, arranged in monograph form The C harmacrutical Society, using known experts to write individual Pharn assriated with product development and innovation. Part II includes The Codex is edited quick ual chapters. 1890 TI Com 1.12 ANNOTED EXTRACTS FROM PHARMACOPOEIAMONC sever BT WAY OF A REPRESENTATIVE EXAMPLE A In comp prep becar NH ever 2HCI, 240 inclt Cao 24N,2044 1948 new OH met Amodiaquin hydrochloride At t Other Name: Camoquin (available in certain overseas countries only) yea A Standard is Given in the British Pharmacopoeia 1973. Description: A yellow odourless crystalline powder with a bitter taste. Solubility: Soluble at 20°, in 22 parts of water and in 70 parts of alcohol; very shgnuy ins grc (1s and in chloroform. ad Acidity. A2h solution has a pH of 4.0 to 4.6. Moisture Comtent: 6 to 10o, determined by drying over phosphorus Storage. It should be stored in airtight containers. phosphorus pentoxide in vacu ldentification Test: To 1 ml of 2% solution precipitate is produced. st: To 1 mi of 2% solution add 0.5 ml of cobalt thioy Melting Point: About 158C. Soluton Determination in body fluids: Spectrofluorimery: In plasma or serun World Health Organisation, 1974, 51, 431. Ultraviolet Absorption: In 0.1 N hydrocholoric acid, maxima a * (E 1, 1 cm 366). m, 237 nm,and Metabolism Absorption: Readily absorbed after oral administration. or serum G.M. Trent
- 15. Introduction to Pharmaceutical Chemistry 15 Blood Concentration: After an oral dose of 10 mg/kg, plasma concentration of 300 to 560 mg/ml are attained in 4 hours; therapeutic concentration are attained 1 to 2 hours after dosing. Distribution: Widely distributed troughout the tissues, high concentrations are found in the liver, spleen, kidneys, and lungs with smaller amounts in the brain and cerebrospinal fluid, in the blood, higher concentrations are found in red cells than in the plasma. Excretion: Slowly excreted in the urine but the rate may be increased if the urinary pH is decreased. Action and Uses: Amodiaquin hydrochloride is an antimalarial drug, which has actions and uses similar to those described under chloroquine phosphate A dose equivalent to 200 to 400 milligrams of the base given orally once a week is usually adequate for the suppression or so-called prophylaxis of malaria in an adult; 130 milligrams of the hydrochloride is equivalent to 100 milligrams of the base. A single dose equivalent to 600 milligrams of the base is often sufficient to control a malarial attack although the equivalent to 400 to 600 milligrams of the base daily for 3-days may be necessary. The dose in terms of the base for a child corresponding to 600 milligrams of the base for an adult is: up to one year 75 to 150 milligrams; 1 to 5 years, 125 to 250 milligrams; 6 to 12 years, 270 to 450 milligrams. Amodiaquin has been used for the treatment of chronic discoid lupus erythematosus, a single dose equivalent to 200 milligrams of the base is given daily until the condition iscontrolled Undesirable efects: Undesirable effects are rare with antimalarial dose but it may cause nausea, vomitting, diarrhoea. Long continued use of the drug may result in blue-gray deposits in the cornea, fingernails, and hard palate. The corneal deposits slowly resolves after stopping treatment. Preparation Amodiaquin Tablet: Available as tablets containing amodiaquin hydrochlorideequivalentto 200 mg of amodiaquine base. A standard for these tablets is given in the British Pharmacopoeia 1973. Containers and Storage: See the entry on tablets for general information on containers and storage containers should be airtight. Labelling: A lable on the container should state the amount of the medicament as the equivlent amount of amodiquine base. Advice for patients: A tablet should be taken at regular intervals, preferably after meals. For prophylaxis, doses should be taken during the period at risk and for 4 weeks thereafter 1.13 THE DRUGS AND COSIMETICS ACT, 1949 Scope The Drugs and Cosmetics Act, 1940 has been enacted for the purpose of proper enforcement and the purpose is that no substandard drugs be sold in the market and no one will sell even genuine drug without licence. The Drugs and Cosmetics Act does not contain any special provisions which would override the general provisions of code of criminal procedure, and general provisions of Cr. P.C. will apply. The Drug Act is mainly concerned with the standard and quality of drugs manufactured in this country and therefore controls the manufacture, sale and distribution of drugs. This act is not related to excise duty or impositions on narcotic drugs.
- 17. Introduction to Pharmaceutical Chemistry 17 purpose are contained in Rules of the Drug Rules published (or notified). The Pharmacopeia prescribes the standard proportion of contents of the drug or cosmetic. If these content proportions are not maintained then the defendant is liable for legal action. Misbranded drugs A drug shall be deemed to be misbranded: (a) if it is so coloured, powered or polished that damage is concealed or if it is made to appear of better or greater therapeutic value than it really is; or (6) if it is not labelled in the prescribed manner; or c) if its label or container or anything accompanying the drug bears any statement, design or device which makes any false claim for the drug or which is false or misleading in any particular manner. Adulterated drugs: The drug shall be deemed to be adulterated: (a) if it consists, in whole or in part, of any filthy, putrid or decomposed substance; or (6) if it has been prepared, packed or stored under insanitary conditions whereby it may have been contaminated with filth or whereby it may have been rendered injurious (c) if its container is composed in whole or in part of any poisonous or deleterious substance which may render the contents injurious to health; or (d) if it contains any harmful or toxic substance which may render it injurious to health; or (e) if it bears or it contains, for the purposes of colouring only, a colour other than one which is prescribed; or health; or ) if any substance has been mixed therewith so as to reduce its quality or strength. Spurious drugs: A drug shall be deemed to be spurious: (a) if it is imported under a name which belongs to another drug; or (b) if it is an imitation of, or is a substitute for, another drug or resembles another drug in a manner likely to deceive or bears upon it or upon its label or container the name of another drug unless it is plainly and conspicuously marked so as to reveal its true character and its lack of identity with such other drug; or C) if the label or container bears the name of an individual or company purporting to be the manufacturer of the drug, which individual or company is fictitious or does not exist; or (d) if it has been substituted wholly or in part by another drug or substance; or (e) if it purports to be the product of a manufacturer of whom it is not truly a product. Licence to sel, stock, exhibit or offer for sale or distribute drugs by retail other than those specified in [Schedules C, C (1) and [X] [Rule 61 (1)] Licence Form 20 is to be filled in by the official drug distributor having following proforma: 1..s hereby licensed to sell, stock or exhibit for sale or distribute by retail drugs other than those specified in [Schedules C, C (1) and x] of the Drugs and Cosmetics Rules, 1945, and to operate a pharmacy on the premises situated at.subject to the conditions specified below and to the provisions of the Drugs and Cosmetics Act, 1940 and the Rules thereunder. 2. The licence shall be in force from.. to
- 18. janic Vol Pharmaceutical Chemistry (Inorgaan 18 3. Name(s) of qualified person(s) in charge... 4. Categories of drugs . . . Date.. Licence No.. Licensing Authority] Conditions for Licence (1) This licence shall be displayed in a prominent place in a part of the premises open to the puh (2) The licence shall comply with the provisions of the Drugs and Cosmetics Act 1940 and the R. (3) (1) No drug shall be sold unless such drugs are purchased under cash or credit memo from (i) No sale of any drug shall be made to a person notholding ndition the requisite shall licence not apply to sell, to stoct the sal i Ru thereunder for the time being in force. duly licensed dealer or a duly licensed manufacturer. exhibit for sale or distribute the drug, provided that this condition shall not apPly to the sal of any drug to. a) an officer or authority purchasing on behalf of Government, or (0) a hospital, medical, educational or research institution, or a registered medical practitione for the purpose of supply to his patient [or] (a) a manufacturer of beverages, confectional biscuits and other non-medical products, wvher such drugs are required for processing those products. 4) The licensee shall inform the Licensing Authority in writing in the event of any change inth constitution of the firm operating under licence. Where any change in the constitution of firm take. place, the current licence shall bedeemed to be valid for a maximum period of three months from th cdate on which the change takes place unless, in the meantime, a fresh licence has been taken fromth licensing authority in the name of firm with the changed constitution. Questions Questions 1. What is meant by pharmaceutical chemistry? 2. Discuss the important aspects of pharmaceutical chemistry. 3. What is the importance of chemistry in pharmacy? 4. Discuss the history of pharmaceutical chemistry. 5. What is meant by Pharmacopoeia? Discuss the history of Pharmacopoeia. 6. What is meant by the term monograph? What are the contents of monograph? 7. Define and explain the following terms: (a) Assay (b) Monograph (c) Official compound (d) Pharmacopoeia. 8. Write in brief about "storage of pharmaceutical compounds". 9. Explain the terms: (i) Pharmacopoeia (i) Monographs 10. What are B.P., U.S.P. and I.P.? Explain briefly ? 11. What are the contents of monog:aphs in general ? 12. Give a brief extract of pharmacopeial monograph ot a representative pharmaceutical, 13. (n Give Standard the of quality, (ii) Misbranded drug. () Adulterated drug, (i») Spurious drug. 13. Give the definitionof: 14. Describe how the development of pharmaceuticals can be carried out