DGH idiopática: diagnóstico precoce e tratamento com GH
•Télécharger en tant que DOCX, PDF•
1 j'aime•717 vues

O documento discute a deficiência de hormônio do crescimento (DGH) idiopática em crianças. É importante que pais levem crianças com baixa estatura para avaliação precoce, pois quanto mais cedo o diagnóstico e tratamento, melhor será a altura adulta final. Além disso, o documento descreve outras indicações aprovadas para uso de GH, como baixa estatura idiopática, síndrome de Turner, insuficiência renal crônica e síndrome de Prader-Willi.

Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à DGH idiopática: diagnóstico precoce e tratamento com GH
Similaire à DGH idiopática: diagnóstico precoce e tratamento com GH (20)
Plus de Van Der Häägen Brazil
Plus de Van Der Häägen Brazil (20)
Dernier
Dernier (7)
DGH idiopática: diagnóstico precoce e tratamento com GH
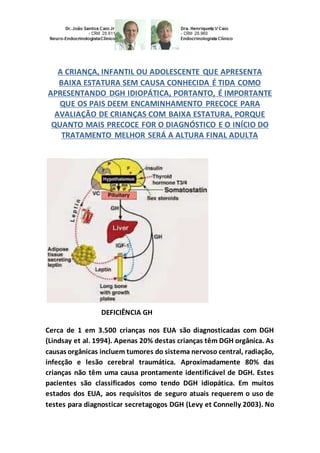
- 1. A CRIANÇA, INFANTIL OU ADOLESCENTE QUE APRESENTA BAIXA ESTATURA SEM CAUSA CONHECIDA É TIDA COMO APRESENTANDO DGH IDIOPÁTICA, PORTANTO, É IMPORTANTE QUE OS PAIS DEEM ENCAMINHAMENTO PRECOCE PARA AVALIAÇÃO DE CRIANÇAS COM BAIXA ESTATURA, PORQUE QUANTO MAIS PRECOCE FOR O DIAGNÓSTICO E O INÍCIO DO TRATAMENTO MELHOR SERÁ A ALTURA FINAL ADULTA DEFICIÊNCIA GH Cerca de 1 em 3.500 crianças nos EUA são diagnosticadas com DGH (Lindsay et al. 1994). Apenas 20% destas crianças têm DGH orgânica. As causas orgânicas incluem tumores do sistema nervoso central, radiação, infecção e lesão cerebral traumática. Aproximadamente 80% das crianças não têm uma causa prontamente identificável de DGH. Estes pacientes são classificados como tendo DGH idiopática. Em muitos estados dos EUA, aos requisitos de seguro atuais requerem o uso de testes para diagnosticar secretagogos DGH (Levy et Connelly 2003). No
- 2. entanto, uma pesquisacom endocrinologistaspediátricos na América do Norte descobriu que 95% dos endocrinologistas não acreditam que os testes de secretagogosé omelhor método de identificaçãopara verificar quem necessita do tratamento com GH (Hardin et al. 2007). Isto é em parte devido ao reconhecimento de que existem valores de corte arbitrários para a definição de DGH, a falta de reprodutibilidade dos resultados dos testes e o fato de que algumas crianças com velocidade de crescimento extraordinariamente anormal poderão ter resultados "normais" para testes de secretagogos. Não pode, contudo, ser um ressurgimento de entusiasmo para os testes de estimulação devido à recente aprovação do IGF-I recombinante no tratamento de crianças com deficiênciade IGF-I. São necessários testes secretagogos oude IGF-I, o teste de estimulação para distinguir o IGF-I e a deficiência de GH. O consenso de opinião de pesquisa do endocrinologista (Hardin et al. 2007), o Hormônio do Crescimento Research Society (2000) e do norte- americano Lawson Wilkins Pediatric Endocrine Society (Wilson et al. 2003) indicam que o diagnóstico de DGH exige a integração de critérios auxológicos, histórico médico, exames laboratoriais, radiológicos e avaliações. O encaminhamento para um endocrinologista deve ser feito para crianças com altura <percentil 3, aquelas com baixa velocidade de crescimentoe aquelas que demonstramdisparidade significativa entre a altura projetada e a esperada altura mid-parental (Juul et al. 1994).
- 3. Estudos indicamque quanto mais cedose iniciar o tratamentomelhor seráa altura final adulta, assimquanto mais cedoo diagnóstico, melhor o prognósticopara a altura. Alémdisso, os estudos indicammaior eficáciacom doses mais elevadas de GH, e tratamentodeve ser contínuo (Blethenet al. 1996;MacGillivray et al. 1996, 1998). Assim, é importante que os pais deemencaminhamentoprecoce para avaliação de crianças com baixa estatura, crianças comdeclíniode percentis de altura, e para as crianças que não crescememconcordânciacom a sua alturaadulta prevista. A duração do tratamentocom GH é controversa. Por muitos anos, o GH foi dado até que a fusão epifisária. Novos dados sugeremque o GH tembenefícios importantes paraamineralizaçãoóssea, massa magra (Saggese et al. 1996;Underwoodet al. 2003;Boguszewskiet al. 2005) e melhoraos fatores de riscocardíaco, como a diminuição do tecidoadiposovisceral e melhorao perfil lipídico(Colaoet al. 2002; Lanes et al. 2003;Underwoodet al. 2003). Esses benefícios têmlevadoa aprovação para o tratamentocom GH de adultos (em doses mais baixas) e sugeremque o tratamentocomGH deve ser efetuadoao longo da vida. A reavaliaçãopara determinar se aDGH é persistente é indicada. Apesar do recente desenvolvimentode diretrizes parao gerenciamentode pacientes emtransição (Claytonet al. 2005), as diferenças de opinião permanecemsobre como e quando essareavaliação deve ser realizada, adose ideal GH no períodode transição, e os respectivos papéis noadultoe nas crianças na gestãodo cuidado endócrinode pacientes emtransição. A dosagemideal de GH durante a puberdade também é controversa. Emcrianças normais, a produção de esteróides sexuais durante apuberdade estimula
- 4. independentemente ocrescimentoe aumentaa secreçãode GH, o que resultanoestirão. Os estudos sugeremque pacientes comDGH podem atingir um maior crescimentopuberal se tratados comdoses de GH mais elevadas do que aquelas utilizadas emcrianças pré-puberdade (Codner et al. 1997; Mauras et al. 2000;Saenger 2003). O IGF-I é específicoparaa fase da puberdade e o sexo, e boa evidênciasugere que amonitorizaçãodos níveis de IGF-I é útil para determinar adose ideal de GH (Park e Cohen 2004). Emnenhum momento issoé provavelmente mais importante do que durante a puberdade. Parece lógicoque as crianças com DGH devem dosar o GH de acordo com a manutenção de níveis específicosIGF-I para a fase da puberdade e o sexopara que o crescimentosejamaximizado. OUTRAS INDICAÇÕES DEUSO DE GH APROVADAS PELO FDA Baixaestaturaidiopática(BEI) Baixaestaturaidiopática(BEI) é definidapor uma alturade 2,25 ou mais desvios padrãoabaixo da média(ou menos do que o percentil 1,2) para a idade e o sexo, semevidência de doença subjacente ou DGH (Rekers- Mombarg et al. 1999). Esta definiçãoaplica-se a cercade 400.000 crianças nos EUA e inclui um diversificadogrupode pacientes. Nos EUA, oFDA aprovou GH para BEI em 2003. Aprovaçãosimilar nãoexiste naEuropa. O grau de melhoria resultante daalturado tratamentocom GH de crianças com BEI varia de acordo com o estudode investigação(Hintz et al. 1999;Finkelsteinet al. 2002;Leschek et al. 2004;Kempet al. 2005). O usode GH para a BEI
- 5. permanece controverso, emparte devidoàvariabilidade na melhoriada alturarelatada, mas também devidoàs medidas mal definidas de sucessoterapêutico(por exemplo, amelhoriada adaptação psicossocial) e o debate sobre se o objetivodotratamentodeve ser simplesmente uma altura"normal" ou altura"máxima" (Allene Fost 2004). Para complicar ainda mais as questões é o aumentoda consciência públicasobre a indicaçãoBEI, resultandoempedidos de terapiacom GH. A avaliação por um especialistaé recomendadaparacrianças com altura no percentil 3 oumenos, e velocidade de crescimentopobre. O encaminhamentoprecoce (antes dapuberdade) irá proporcionar tempo para um maior benefíciodaaltura e deve ser necessáriotratamento. A síndrome de Turner (ST) Meninas com ST têmum cromossomoX anormal ou ausente, resultando em baixa estaturae falênciaovariana(Saggese et al. 1996). STocorre em 1 em 2.500 nascimentosvivos dosexofeminino, tornando-se umacausa comum de baixa estaturaemmeninas. A variabilidade emcaracterísticas fenotípicas, muitas vezescontribui paraum atrasono diagnóstico; portanto, o cariótipoé recomendado para qualquer mulher jovem, com inexplicável baixaestatura(alturaabaixodo percentil 5), puberdade atrasada, ou quaisquer característicasclínicas daST(Savendahl et Davenport 2000). O tratamentocomGH aumenta a taxa de crescimento e a alturafinal de adultodas meninas com ST (Sas et al. 1999; Chernausek et al. 2000). Estudos indicamque a melhoriano crescimento estárelacionadaà dose e duração do tratamentoantes do inícioda terapiade reposiçãode estrogênio(Chernauseket al. 2000).
- 6. CARIÓTIPO SÍNDROME DE TURNER Alguns estudos sugeremque a adição de baixas doses de oxandrolona melhoraa alturafinal (Rosenfeldet al. 1998;Sas et al. 1999;Chernausek et al. 2000;Reiter et al. 2001). Umestudorecente (Davenport et al. 2007) sugere claramente que aterapiacom GH antes da idade de cinco anos é segurae melhoraa alturafinal. O diagnósticoprecoce promove a coordenaçãode estratégias de manejoparaprevenir morbidades relacionadas com ST (por exemplo, doenças cardiovascularese otológicas) e pode também aumentar a alturado adulto, permitindo uma maior duração da terapiade GH antes do inícioda reposiçãode estrogênio(Reiter et al. 2001). Insuficiênciarenal crônica(IRC) A baixaestaturaé comum emcrianças com IRC. Várias razões contribuempara a patogênese incluindoacidose metabólica, distúrbios de água e eletrólitos, desnutriçãoproteico-calórica, osteodistrofiarenal e tratamentocomcorticosteróides, que criamresistênciaàação do GH (Kuizonet Salusky 1999;Roelfsemaet Clark 2001). Anormalidadesno eixoGH-IGF-I podem tambémcontribuir (Roelfsemaet Clark 2001). A maioria dos pacientes comdoença renal têmaltos níveis de GH
- 7. secundário à diminuiçãoda depuraçãorenal; no entanto, eles têm também um decréscimononúmero de receptores de GH, aumentoda produção de proteínas de ligaçãoao IGF e uma redução da biodisponibilidade de IGF-I. Apesar destas alterações metabólicas, os estudos têmdemonstradoque a terapiade GH aumenta significativamente ocrescimentolinear (Fineet al. 1994a; Hokken- Koelegaet al. 2000;Haffner et al. 2000), adensidade mineral óssea(Van Dyck et al. 2001), opesocorporal, e a magra massa em IRC (Fine et al. 1994b). Alémdisso, oGH não aceleraa progressãodainsuficiênciarenal e não aceleraa necessidade de diálise (Tönshoff et al. 1992). O uso do GH em IRC é uma indicação aprovada pela FDA e o usode GH para esses pacientestemsidolimitada(<10% das crianças cadastradas no Transplante Renal PediátricoNorte-Americanode Estudo Cooperativo-2005). Uma possível razãoé a falta de dados de alturade indivíduos adultos uma vez que apenas estudos recentes têmincluídoa alturaadulta final (Fine et al. 1994b). Alémdisso, a alturapode ser percebida como uma preocupação menos graves no contexto de outros problemas médicos complexos experimentados por crianças com IRC. Noentanto, a faltade crescimentocontinuaaser um problema clínicosignificativodessas crianças, e otratamentocomo GH deve ser iniciadoo mais cedo possível. Síndrome de Prader-Willi (SPW) Nos EUA, o FDA aprovou o GH para o tratamentodaSPW em 2000. A
- 8. SPW é um distúrbiogenéticocausadopor deleçãoou ausênciade expressãode uma porção do cromossoma15, e derivadopaternalmente ocorre em cercade 1 em 25.000 nascimentos. Emboraos critérios diagnósticos estejamdisponíveis (Gunay-Aygunet al. 2001), os recursos não específicos paraSPWna infância muitas vezes contribuemparaum diagnósticotardio. As manifestações clínicas incluemumadiminuiçãodo crescimentodolinear, bemcomo a hipotonia, hiperfagia, obesidade, hipogonadismo, distúrbios dosono e perturbações docomportamento (Goldstone 2004). A disfunçãoresultade uma disfunçãohipotalâmica levandoà DGH. A eficáciado tratamentocom GH emmelhorar o crescimentolinear, aforçafísica, agilidade, e composiçãocorporal em crianças com SPW é bem documentada(Carrel et al. 1999, 2001, 2002). CARACTERÍSTICAS FACIAIS DA SÍNDROMEDEPRADER-WILLI Um estudorecente (Carrel et al. 2004) demonstraasegurançae a eficáciaem crianças. Estudos tambémdemonstrammudanças positivas no perfil lipídicoe aumentoda força muscular (Haqq et al. 2003). A morte súbitatemsido relatadaem17 crianças com SPW que foram tratadas com GH (Van Vliet et al. 2004). Estas crianças apresentavam obesidade mórbidaprecoce subjacente (IMC 31-42
- 9. kg/m 2), distúrbios respiratórios e/oupossíveisdistúrbios dosono, e em geral eram muitojovens (Eiholzer 2005). Continuaa ser possível, mas não certo, que a terapiacom GH possater contribuídopara estas mortes (Van Vliet et al. 2004;Eiholzer 2005).SeoGH for um fator contribuinte, a principal hipótese sobre acausa é a de obstruçãodas vias aéreas pela hipertrofiados tecidos moles;noentanto, até o momento não há nenhuma evidênciapublicadade que essahipertrofiatenhacontribuído para estas mortes. A maioriados endocrinologistasrecomendam estudos dosono e correçãode obstruçãodas vias aéreas antes de iniciar o tratamentocom GH (Allenet Carrel 2004). Muitosmédicos acreditam que os benefícios dotratamentosuperamos riscos do uso do GH em crianças com SPW. Pequenopara a idade gestacional (PIG) Cercade 90 mil crianças nascemPequenas para a Idade Gestacional (PIG) nos EUA a cada ano (Lee et al. 2003). A maioria apresenta aceleraçãodo crescimentopós-natal e têmcatch-up adequado por 2 anos, com a maioria alcançando crescimentonormal nos primeiros 6 meses (Kelnar 2003a). É importante saber que em recém-nascidos pré-termo, aaceleraçãodo crescimentopode ser adiadaaté a idade de 5 anos (Boonstraet al. 2003). Apesar docrescimentoadequado, emaproximadamente 10% dos pacientes, opadrão de crescimentocontinuaaser anormal com altura<- 2,5 DS (Davenport 2005).
- 10. O GH foi aprovado para crianças nascidas PIG em 2001 nos EUA e na Europa em 2003. Foram relatados benefícios do GH no aumento da altura adulta final e na densidade mineral óssea em crianças nascidas PIG para possível tratamento (Arends et al. 2003; Van Pareren et al. 2003; Dahlgren et Wikland 2005). Os endocrinologistas devem excluir outras causas potenciais para o crescimentopobre antes de tratar, mas é evidente que otratamentodeve ser oferecido quando outras causas são excluídas. Aspectos do tratamento que necessitam de estudo em curso incluem a determinação da dose ideal e a duração do tratamento. Estudos recentes (Hokken-Koelega et al. 1995; Drake et al. 2001) sugerem que as crianças que iniciam o tratamento com GH durante meados do final da infância, e aqueles com retardo de crescimento abaixo de 3 DS, podem precisar de doses mais elevadas de GH do que a dose tradicional. Muitas crianças nascidas PIG têm problemas médicos adicionais e têm documentado risco de doenças metabólicas como hipertensão, hiperlipidemia, resistência à insulina e doença cardiovascular mais tarde na vida (Harris et al. 2004). O monitoramento para estes problemas é importante para o endocrinologista e o médico pediatra. Síndrome do intestinocurto(SIC) O GH foi aprovado para terapiaSIC nos EUA para pacientes que receberam"apoionutricional especializado", incluindoaltoteor de carboidratos, dietade baixa gordura, dietaenteral ouparenteral e pacientes que recebemcertas dietas elementares. A aprovaçãonão se limitoua uma idade específica, mas há estudos pediátricos específicos que foram apresentados aoFDA. Os estudos comadultos usados para a aprovação Garner-documentandoa diminuiçãoda necessidade de nutriçãoparenteral, quandoGH foi dado por 6 semanas.
- 11. Os estudos sãonecessários paradeterminar adose e duração ótimada terapêuticapara pacientes pediátricos. A dose recomendadaatual é 0,1-0,8 mg/kg por dia (rDNA). Emadultos com SIC, a administraçãode GH promoveumelhora significativanaabsorção de nutrientes, dopeso corporal e da massa corporal magra (Seguy et al. 2003). Sãonecessários mais estudos aprofundados emcrianças. Síndrome de Noonan(SN) A Síndrome de Noonan, uma condição autossômicadominante que ocorre em 1:1.000 a1:2.500 nascidos vivos, é amais recente indicação de aprovado pelaFDA para tratamentocomGH. A síndrome é caracterizadapor algumas características clínicas semelhantes à síndrome de Turner e incluem:baixa estatura, estenose valvular pulmonar, dismorfiafacial e hipertelorismo(hipertelorismoconsiste numa malformação do crânio do bebê que causa um afastamentodos olhos e das órbitaoculares emexcesso), escavaçãotorácica, pescoçoem pá, retardomental moderado, surdez, hipogonadismo, criptorquidia, e alterações dacoagulação (Asokanet al. 2007). Parece haver anormalidades do eixoGH/IGF-I. Estudos indicamque o GH melhora a alturadessas crianças;no entanto, o número de estudos é pequeno(Kirk et al. 2001;Kelnar 2003b). Umgrupo de pacientes comsíndrome de Noonan, aqueles comuma mutação genéticaemPTPN 11, têmaltura basal inferior (Ferreiraet al. 2005).
- 12. Este gene é responsável pelatransduçãode sinal em células GH/IGF-I e alguns relatórios sugeremque os pacientes comsíndrome de Noonan com estamutação podem ter menor respostaao GH (Kirk et al. 2001). É possível que a terapia com o IGF-I recombinante possa proporcionar um melhor crescimento do que o GH neste subgrupo populacional. LOW HEIGHT IN CHILDREN, YOUTH AND TEEN BY GHD USING SOMATOTROPIN BY rDNA;DR. CAIO JR. ET DRA. CAIO. CHILD, INFANTOR TEENAGER HAS SHORTSTATURE OF UNKNOWN CAUSE IS PRESENTING AS GHD IDIOPATHIC, SO IT IS IMPORTANTFOR PARENTS TO REFERRAL FOR EARLY ASSESSMENTOF CHILDREN WITH LOW HEIGHT, BECAUSETHE MOREFOR EARLY DIAGNOSIS AND TREATMENTOF THE BEGINNING BETTER BE THE FINAL ADULTHEIGHT; PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY-GENETICS- ENDOCRINE-PEDIATRICS (SUBDIVISIONOF ENDOCRINOLOGY):DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. GHD About 1 in 3.500 childreninthe U.S. are diagnosedwithGHD (Lindsay et al. 1994). Only 20% of these childrenhave organic GHD. Organic causes include tumors of the central nervous system, radiation, infection, and traumatic brain injury. Approximately 80% of childrendonot have a readily identifiable cause of GHD. These patients are classifiedas having
- 13. idiopathic GHD. In many U.S. states, the current insurancerequirements require the use of tests todiagnose GHD secretagogues(Levy et Connelly 2003). However, asurvey of pediatric endocrinologistsinNorthAmerica found that 95% of endocrinologists donot believe that the tests secretagoguesis the best methodof identificationtoverify whoneed treatment withGH (Hardinet al. 2007). This is partly due to the recognitionthat there are values of arbitrary cut-off for defining GHD, lack of reproducibility of test results andthe fact that some childrenwith extremely abnormal growthrate may be "normal" for results of tests secretagogues. There may, however, be a resurgence of enthusiasmfor the stimulationtestsdue to the recent approval of recombinant IGF-I in the treatment of childrenwithIGF-I deficiency. Requiredsecretagogues or IGF-I tests, the stimulation test todistinguish are IGF-I and GH deficiency. The consensus of opinionresearch Endocrinologist (Hardinet al. 2007), GrowthHormone ResearchSociety (2000) andthe U.S. LawsonWilkins Pediatric Endocrine Society (Wilson et al. 2003) indicate that the GHD diagnosis requiresintegration auxológicos criteria, medical history, laboratory tests, imaging studies and reviews. The referral toan endocrinologistshouldbe done for childrenwithheight <3rdpercentile, those withlowgrowthrate and those that demonstrate significant disparity betweenthe projected height and the expectedmid-parental height(Juul et al. 1994). Studies indicate that the sooner you start treatment the better the final adult height, sothe earlier the diagnosis, the better the prognosis for the height. Moreover, studies indicate greater efficacy at higher doses of GH,
- 14. and treatment shouldbe continued(Blethenet al. 1996;MacGillivray et al. 1996, 1998). Thus, it is important that parents deemearly referral for evaluationof childrenwithshort stature childrenwithdeclining height percentiles, andfor childrenwho do not growin accordance with their expectedadult height. The durationof GH therapy is controversial. For many years, GH was givenuntil the epiphyseal fusion. Newdatasuggest that GH has important benefits for bone mineralization, leanmass (Saggese et al. 1996;Underwoodet al. 2003;Boguszewski et al. 2005) and improves cardiac risk factors, suchas decreasedvisceral adipose tissue andimproves the lipidprofile (Colaoet al. 2002;Lanes et al. 2003; Underwood et al. 2003). These benefits have ledtoapproval for the treatment of adults withGH (lower doses) and suggestedthat GH treatment shouldbe performed throughout life. Revaluationto determine whetherthe GHD is persistent is indicated. Despite the recent development of guidelines for the management of patients intransition (Claytonet al. 2005), differences of opinion remainabout how and when this reassessment shouldbe performed, the optimal dose GH in the transitionperiod, andtheir roles inadults and childreninthe management of endocrine care to patients intransition. The optimal dose of GH during puberty is alsocontroversial. Inhealthy children, the productionof sex steroids during puberty independently stimulates growthand enhances the secretionof GH, which results inspurts. Studies suggest that patients withGHD canachieve a higher pubertal growthwhen treatedwithhigher doses of GH than those usedin pre-
- 15. pubertal children(Codner et al. 1997;Mauras et al. 2000;Saenger 2003). IGF-I is specific for puberty andsex, and good evidence suggeststhat monitoring the levels of IGF-I is useful todetermine the optimal dose of GH (Park and Cohen 2004). Inno time it is probably more important than during puberty. It seems logical that childrenwith GHD shouldGH dose according to the maintenance of specific IGF-I levels topuberty andsex for that growthis maximized. OTHER INDICATIONS FOR USEOF GH APPROVED BY FDA Idiopathic short stature (ISS) Idiopathic short stature (ISS) is definedby a height of 2.25 or more standarddeviations belowthe average (or less than1.2 percentile) for age and sex, without evidence of underlying diseaseor GHD (Rekers- Mombarg et al. 1999). This definitionappliestoapproximately 400,000 childreninthe U.S. and includes a diverse groupof patients. Inthe U.S., the FDA approvedGH for ISS in 2003. Similar adoptiondoes not exist in Europe. The degree of enhancement resulting fromtime of treatment withGH of childrenbank varies according tothe researchstudy (Hintz et al 1999;Finkelsteinet al 2002;Leschek et al 2004;Kempet al 2005). The use of GH for the ISS remains controversial, inpart due to the variability inreportedimprovement inheight, but alsodue toill-defined measures of treatment success(e.g., improvedpsychosocial adaptation) and the debate about whether the goal of treatment shouldbe just a "normal" time or "maximum" height (Allenet Fost 2004). Further complicating matters is the increasedpublic awareness of the ISS
- 16. statement, resulting inorders of GH therapy. The evaluationby a specialist is recommendedfor children3 percentile inheight or less, and poor growthvelocity. The early referral (before puberty) will provide time for a greater benefit of time and treatment shouldbe necessary. Turner syndrome (TS) Girls withTS have an abnormal or missing X chromosome, resulting in short stature andovarian failure (Saggese et al. 1996). TS occurs in 1 in 2,500 live female births, making it acommon cause of short stature in girls. The variability inphenotypic characteristics, oftencontributestoa delay in diagnosis;Therefore, the karyotype is recommendedfor any young woman withunexplainedshort stature (height belowthe 5th percentile), delayedpuberty, or any clinical features of ST(Davenport et Savendahl 2000). GH treatment increasedthe growthrate andthe final adult height of girls withTS (Sas et al 1999;Chernausek et al 2000). Studies indicate that the improvement ingrowthis relatedtothe dose and duration of treatment before the onset of estrogenreplacement (Chernausek et al. 2000) therapy. Some studies suggest that the addition of low doses of oxandrolone improves the final height (Rosenfeldet al 1998;Sas et al 1999;Chernausek et al 2000;Reiter et al 2001). A recent study (Davenport et al. 2007) clearly suggests that GH therapy before the age of five is safe and improves the final height.
- 17. Early diagnosis promotes the coordinationof management strategies to prevent morbidity relatedtoST (e.g., cardiovascular and ear diseases) and may alsoincrease adult height, allowing a longer durationof GH therapy before the onset of estrogenreplacement(Reiter et al. 2001). Chronic renal failure (CRF) Short stature is common in childrenwithCRF. Several reasons contribute to the pathogenesis including metabolic acidosis, disorders of water and electrolytes, protein-calorie malnutrition, renal osteodystrophy and corticosteroidtherapy, whichcreate resistancetoGH action(Kuizon et Salusky 1999;Roelfsemaet Clark 2001). Abnormalities inthe axis GH- IGF-I may alsocontribute (Clark et Roelfsema2001). Most patients with kidney disease have highlevels of GH secondary todecreasedrenal clearance;however, they alsohave a noticeable decrease inGH receptors, increasedproductionof IGF binding proteins anda reduction in IGF-I bioavailability. Despitethesemetabolic disorders, studies have shown that GH therapy significantly increasesthe linear growth(Fine et al. 1994a; HokkenKoelegaet al. 2000;Haffner et al. 2000), bone mineral density (VanDyck et al. 2001), body weight, and leanbody mass in CRF
- 18. (Fine et al. 1994b). Moreover, GH does not accelerate the progressionof renal failure and accelerates the needfor non-dialysis (Tönshoff et al. 1992). The use of GH in CRF is an indicationapprovedby the FDA and the use of GH in these patients has beenlimited(<10% of childrenenrolled in the NorthAmericanPediatric Renal Transplant Cooperative Study- 2005). One possible reasonis the lack of height data adults since only recent studies have includedthe final adult height (Fine et al. 1994b). In addition, the height can be perceivedas aless serious concerninthe context of other complex medical problems experiencedby children withCRF. However, the lack of growthcontinues tobe a significant clinical problemthese children, andGH treatment shouldbe initiatedas early as possible. Prader-Willi syndrome (PWS) In the U.S., the FDA approved GH for treatment of PWS in 2000. PWS is a genetic disorder causedby deletionor lack of expressionof a portionof chromosome 15, and paternally derivedoccurs inabout 1 in 25,000 births.
- 19. Although diagnostic criteria are available (Gunay-Aygun et al. 2001), features not specific to PWS in childhood often contribute to late diagnosis. Clinical manifestations include a decreased linear growth, as well as hypotonia, hyperphagia, obesity, hypogonadism, sleep disorders and behavior disorders (Goldstone 2004). The disorder results from a hypothalamic dysfunction leading to GHD. The efficacy of GH treatment in improving linear growth, physical strength, agility, and body compositioninchildrenwithPWS is well documented(Carrel et al. 1999, 2001, 2002). A recent study (Carrel et al. 2004) demonstrates the safety and efficacy in children. Studies also show positive changes in lipid profile and increased muscle strength (Haqq et al. 2003). Sudden death has been reported in 17 patients with PWS who were treated with GH (Van Vliet et al. 2004). These children had underlying early morbid obesity (BMI 31-42 kg/m 2), respiratory disorders and/or possible sleep disorders, andwere mostly very young (Eiholzer 2005). It is still possible, but not certain, that GH therapy may have contributed to these deaths (Van Vliet et al 2004; Eiholzer 2005). If GH is a contributing factor, the main hypothesis about the cause of obstructionis airway by hypertrophy of soft tissues;however, todate there is no published evidence that this hypertrophy contributed to these deaths. Most endocrinologists recommend sleep studies and correction of airway obstruction before starting GH treatment (Allen et Carrel 2004). Many doctors believe that the benefits of treatment outweighthe risks of the use of GH in children with PWS. Small for gestational age (SGA) About 90 thousand childrenhad bornSmall for Gestational Age (SGA) in the U.S. each year (Lee et al. 2003). Most have acceleratedpostnatal growthand are suitable for 2 years catch-up, withmost reaching normal growthin the first 6 months (Kelnar 2003a).
- 20. It is important to know that in newborn preterm, growth acceleration can be postponed until the age of 5 years (Boonstra et al. 2003). Although adequate growth by approximately 10% of patients, the growthpatternremains abnormal height <-2.5 SD (Davenport 2005). GH was approvedfor children born SGA in 2001 in the U.S. and Europe in 2003 were reportedbenefits of GH in increasing the final adult height and bone mineral density in children born SGA for possible treatment (Arends et al 2003; Pareren Van et al 2003; Dahlgren et Wikland 2005). Endocrinologists should exclude other potential causes for poor growth before treating, but it is clear that treatment should be offered when other causes are excluded. Aspects of treatment that require ongoing study include determining the optimal dose and durationof treatment. Recent studies (Hokken-Koelega et al. 1995; Drake et al. 2001) suggest that child who starts GH treatment during mid-late childhood, and those with growth below 3 SD retardation, may need higher doses GH higher than the traditional dose. Many children born SGA have additional medical problems and have documented risk of metabolic diseases such as hypertension, hyperlipidemia, insulin resistance and cardiovascular disease later inlife (Harris et al. 2004). Monitoring for these problems is important for the pediatrician and endocrinologist. Short bowel syndrome (SBS) GH therapy has beenapprovedfor SBS in the U.S. for patients who received"specializednutritional support,"including high-carbohydrate, low-fat diet, enteral or parenteral nutritionandpatients receiving
- 21. certainelemental diets. The approval was not limitedtoa specific age, but there are specific pediatric studies weresubmittedtoFDA. The adult studies usedfor approval Garner-documenting the decreasedneedfor parenteral nutrition, whenGH was givenfor 6 weeks. Studies are neededtodetermine the optimal dose and durationof therapy for pediatric patients. SINTOMAS DO INTESTINO CURTO The current recommendeddose is 0.1-0.8 mg/kg per day (rDNA). In adults withSBS, administrationof GH causeda significant improvement in the absorptionof nutrients;the body weight and leanbody mass (Seguy et al. 2003). More in-depthstudies inchildrenare needed. Noonan syndrome (NS) The Noonan syndrome, an autosomal dominant conditionthat occurs in 1:1000 to1:2500 live births, is the latestindicationapprovedby the FDA for treatment withGH. The syndrome is characterizedby some similar to Turner syndrome and clinical features include:short stature, pulmonary valvular stenosis, hypertelorismandfacial dysmorphism(hypertelorism
- 22. is a malformationof the baby's skull causing a departure fromthe eyes and ocular orbit excess), thoracic dig, shovel neck, moderate mental retardation, deafness, hypogonadism, cryptorchidism, andcoagulation disorders (Asokanet al. 2007). There appear tobe abnormalities of GH / IGF-I axis. Studies indicate that GH enhances the height of these children;however, the number of studies is small (Kirk et al 2001;Kelnar 2003b). A groupof patients withNoonansyndrome, those witha genetic mutationin PTPN 11 have lower basal height (Ferreiraet al. 2005). This gene is responsible for signal transductioninGH / IGF-I cells, andsome reports suggest that patients withNoonansyndrome withthis mutation may have a reducedresponse toGH (Kirk et al. 2001). It is possible that treatment withrecombinant IGF-I canprovide better growththanGH in this patient subset. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. O tratamentocomGH por rDNA emadultos mantém a massa e a força muscular, melhorarespiratória, cardiológica, é termogênica - com lipólise que é exatamente oprocessocontráriodalipogênese formação de gordura... http://hormoniocrescimentoadultos.blogspot.com 2. Quando o sangue estácom concentraçãode glicose abaixodo normal, ele recebe glicosedofígado resultante daquebrado glicogênio... http://longevidadefutura.blogspot.com 3. Os fatores que influenciama lipólise e a lipogênese são:ingestão
- 23. calóricainadequada, gastoenergético, estímulohormonal, alterações psicológicas, sócios familiares e hereditários, emoutras palavras, podem queimar a gorduraprincipalmente intra-abdominal... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; "Growth Hormone Deficiency". Reino Unido Fundação Crescimento Infantil. Retirado 2009/01/16; "O atraso no crescimento (em crianças) - hormônio do crescimento humano (HGH)" (pdf). Instituto Nacional de Excelência Clínica. 2008-09-25 . Retirado 2009/01/16 ; James, William; Berger, Timothy; Elston, Dirk (2005). Doenças Andrews da pele: Dermatologia Clínica . (10th ed.). Saunders. ISBN 0-7216-2921-0; "O uso de hormônio de crescimento de substituição em doentes adultos com severa deficiência de hormônio do crescimento". A Sociedade de Endocrinologia. 2000-10-01 . Retirado 2009/01/18; "Human Growth Hormone Deficiency". HGH . Retirado 20 de janeiro de 2012; "hormônio do crescimento humano (somatropina) em adultos com deficiência de hormônio do crescimento" . Instituto Nacional de Excelência Clínica . 2006-07-01 . Retirado 2009/01/16; Rappold GA, Fukami M, Niesler B, et al. (Março de 2002). "deleções do gene SHOX homeobox (baixa estatura homeobox) são uma importante causa de atraso no crescimento em crianças com baixa estatura" . J. Clin. Endocrinol. . Metab 87 (3):. 1402-6 doi : 10.1210/jc.87.3.1402 . PMID 11889216; Saborio P, S Hahn, Hisano S, K Latta, Scheinman JI, Chan JC (Outubro de 1998). "insuficiência renal crônica: uma visão geral de uma perspectiva pediátrica" . Nephron 80 (2):. 134-48 doi : 10.1159/000045157.PMID 9736810 ; Molitch ME, Clemmons DR, Malozowski S, et al. (maio de 2006)."Avaliação e tratamento da deficiência de hormônio de crescimento de adultos: um Endocrine Society Clinical Practice Guideline". J. Clin. Endocrinol. . Metab 91 (5):. 1621-1634 doi : 10.1210/jc.2005-2227. PMID 16636129; AimarettiG, Corneli G, Razzore P, . et al . (Maio de 1998)"hormônio + arginina como testesprovocativos para o diagnóstico de GH Comparação entre hipoglicemia induzida por insulina e hormônio do crescimento (GH) de liberação de A deficiência em adultos " . J. Clin. Endocrinol. . Metab 83 (5):. 1615-8 doi : 10.1210/jc.83.5.1615. PMID 9589665 . Retirado 2008/07/23; "Orientação sobre o uso de hormônio de crescimento humano (somatropina) em crianças com deficiências de crescimento" (pdf). Instituto Nacional de Excelência Clínica. 2002-05-01.Retirado 2009/01/16 ; "Diretrizes de consenso para Adulto Growth Hormone Deficiency, 2007". Contato: Fones: 55 11 5087-4404 ou96197-0305 Nextel: ID:111*101625 Rua Estela, 515 - BlocoD - 12ºandar - Conj. 121/122 Paraiso - São Paulo - SP - Cep 04011-002
- 24. e-mails:drcaio@vanderhaagenbrasil.com drahenriqueta@vanderhaagenbrasil.com vanderhaagen@vanderhaagenbrasil.com Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr Video http://youtu.be/woonaiFJQwY Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl= pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,- 46.650481&spn=0,0&t = h&z=17