
Recommandé
Contenu connexe
Similaire à TASBC - Copy.pptx
Similaire à TASBC - Copy.pptx (20)
Dernier
Dernier (20)
TASBC - Copy.pptx
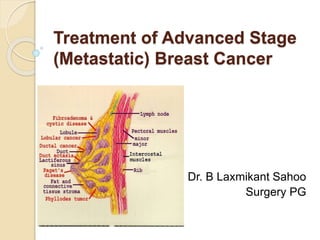
- 1. Treatment of Advanced Stage (Metastatic) Breast Cancer By. Dr. B Laxmikant Sahoo Surgery PG
- 2. Breast Cancer: Statistics According to an article publised in scientific reports. Breast cancer is the most prevalent type of cancer among females in many countries in the past few years. An estimated 22,61,419 new cases were diagnosed in women across the world in 2020.
- 3. the 5-year survival rate of women with this disease is 99%. If the invasive breast cancer is located only in the breast. If the cancer has spread to the regional lymph nodes, the 5-year survival rate is 86%. Where as If the cancer has spread to a distant part of the body, the 5-year survival rate is 29%. Breast cancer is the second most common cause of death from cancer in women in the developed countries after lung cancer. Bone is the most common site of metastasis for breast cancer (65.1%, including single and multiple metastatic sites), followed by lung (31.4%), liver (26.0%) and brain (8.8%) metastasis.
- 4. Aetiological factors Carcinoma of the breast is extremely rare before the age of 20 years. Most breast cancers are diagnosed after age of 50. Breast cancer occurs more commonly in women with a family history of breast cancer than in the general population. There is some evidence that there is a link with diets low in phytoestrogens. Alcohol consumption is associated with an increased risk. Breast cancer is more common in nulliparous women and In postmenopausal women. Breast cancer is more common in the obese. Having a first child at an early age and breast-feeding in particular appears to be protective against breast cancer.
- 5. Pathology Breast carcinoma is usually classifed primarily by its histological appearance. There are two main types/stages of breast cancer : 1. The tumor is limited by the basement membrane of terminal duct- lobular unit (TDLU) (in situ carcinoma) and or 2. The tumor has invaded the stroma and reached beyond the basement membrane of TDLU to become invasive carcinoma.
- 6. The spread of breast cancer Local spread - The tumour increases in size and invades other portions of the breast. It tends to involve the skin and to penetrate the pectoral muscles and even the chest wall if diagnosed late. Lymphatic metastasis - Lymphatic metastasis occurs primarily to the axillary and the internal mammary lymph nodes. Tumours in the posterior one-third of the breast are more likely to drain to the internal mammary nodes. Involvement of supraclavicular nodes and of any contralateral lymph nodes represents advanced disease. Spread by the bloodstream - It is by this route that skeletal metastases occur, although the initial spread may be via the lymphatic system. In order of frequency the lumbar vertebrae, femur, thoracic vertebrae, rib and skull are affected and these deposits are generally osteolytic. Metastases may also commonly occur in the liver, lungs and brain and, occasionally, the adrenal glands and ovaries.
- 7. Clinical presentation Breast cancer is found most frequently in the upper outer quadrant but can be found in any portion of the breast, including the axillary tail. It commonly present as a hard lump, which may be associated with indrawing of the nipple or overlying skin. As the disease advances locally there may be skin involvement with peau d’orange or frank ulceration and fixation to the chest wall. This is described as cancer-en-cuirasse when the disease progresses around the chest wall.
- 9. Investigations Mammography – though it is an important screening tool but a normal mammogram does not exclude the presence of carcinoma. Ultrasound – it is particularly useful in young women with dense breasts in whom mammograms are difficult to interpret, and in distinguishing cysts from solid lesions. It can also be used to localise impalpable areas of breast. It is not useful as a screening tool and
- 11. Magnetic resonance imaging Used to distinguish scar from recurrence in women who have had previous breast conservation therapy for cancer(although it is less accurate within 9 months of radiotherapy because of abnormal enhancement) to assess multifocality and multicentricity in lobular cancer and to assess the extent of high-grade ductal carcinoma in situ (DCIS). It is less useful in low-grade DCIS. it is the best imaging modality for the breasts of women with implants. as a screening tool in high-risk women (because of family history).
- 12. Needle biopsy/cytology Fine-needle aspiration cytology (FNAC) is the least invasive technique of obtaining a cellular diagnosis and is rapid and very accurate if both operator and cytologist are experienced but invasive cancer cannot be distinguished from in situ disease. Large-needle biopsy with vacuum systems – can be used for the management of microcalcifications or in the complete excision of benign lesions such as fibroadenomas. Though a histological specimen taken by core biopsy allows a definitive preoperative diagnosis, differentiates between DCIS and invasive disease and also allows the tumour to be stained for receptor status.
- 13. Positron emission tomography PET scan are used as a staging investigation in patients with T3,T4,N2,N3 breast cancer and in patients with T1 ,T2,N0,N1 breast cancer in presence of symptoms/signs suggestive of metastasis. Inflammatory lesion (namely, mediastinal lymphadenopathy and pleuropulmonary lesions due to pulmonary tuerculosis) may give false –positive results.
- 14. Triple assessment In any patient who presents with a breast lump or other symptoms suspicious of carcinoma, the diagnosis should be made by a combination of clinical assessment, radiological imaging and a tissue sample taken for either cytological or histological analysis, the so-called triple assessment.
- 15. How is the stage determined? Staging systems, 7 key pieces of information are used: The extent (size) of the tumor (T): How large is the cancer? Has it grown into nearby areas? The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes? If so, how many? The spread (metastasis) to distant sites (M): Has the cancer spread to distant organs such as the lungs or liver? Estrogen Receptor (ER) status: Does the cancer have the protein called an estrogen receptor? Progesterone Receptor (PR) status: Does the cancer have the protein called a progesterone receptor? HER2 status: Does the cancer make too much of a protein called HER2? Grade of the cancer (G): How much do the cancer cells look like normal cells?
- 16. Details of the TNM staging system TX: Primary tumor cannot be assessed. T0: No evidence of primary tumor. Tis: Carcinoma in situ (DCIS, or Paget disease of the breast with no associated tumor mass) T1 (includes T1a, T1b, and T1c): Tumor is 2 cm (3/4 of an inch) or less across. T2: Tumor is more than 2 cm but not more than 5 cm (2 inches) across. T3: Tumor is more than 5 cm across. T4 (includes T4a, T4b, T4c, and T4d): Tumor of any size growing into the chest wall or skin. This includes inflammatory breast cancer.
- 17. N categories for breast cancer NX: Nearby lymph nodes cannot be assessed (for example, if they were removed previously). N0: Cancer has not spread to nearby lymph nodes. N0(i+): The area of cancer spread contains fewer than 200 cells and is smaller than 0.2 mm. The abbreviation "i+" means that a small number of cancer cells (called isolated tumor cells) were seen in routine stains or when a special type of staining technique, called immunohistochemistry, was used. N0(mol+): Cancer cells cannot be seen in underarm lymph nodes (even using special stains), but traces of cancer cells were detected using a technique called RT-PCR. RT-PCR is a molecular test that can find very small numbers of cancer cells.
- 18. N2: Cancer has spread to 4 to 9 lymph nodes under the arm, or cancer has enlarged the internal mammary lymph nodes N2a: Cancer has spread to 4 to 9 lymph nodes under the arm, with at least one area of cancer spread larger than 2 mm. N2b: Cancer has spread to one or more internal mammary lymph nodes, causing them to become enlarged.
- 19. N3: Any of the following: N3a: either: Cancer has spread to 10 or more axillary lymph nodes, with at least one area of cancer spread greater than 2 mm, OR Cancer has spread to the lymph nodes under the collarbone (infraclavicular nodes), with at least one area of cancer spread greater than 2 mm. N3b: either: Cancer is found in at least one axillary lymph node (with at least one area of cancer spread greater than 2 mm) and has enlarged the internal mammary lymph nodes, OR Cancer has spread to 4 or more axillary lymph nodes (with at least one area of cancer spread greater than 2 mm), and to the internal mammary lymph nodes on sentinel lymph node biopsy. N3c: Cancer has spread to the lymph nodes above the collarbone (supraclavicular nodes) on the same side of the cancer with at least one area of cancer spread greater than 2 mm.
- 20. M categories for breast cancer M0: No distant spread is found on x-rays (or other imaging tests) or by physical exam. cM0(i+): Small numbers of cancer cells are found in blood or bone marrow (found only by special tests), or tiny areas of cancer spread (no larger than 0.2 mm) are found in lymph nodes away from the underarm, collarbone, or internal mammary areas. M1: Cancer has spread to distant organs (most often to the bones, lungs, brain, or liver) as seen on imaging tests or by physical exam, and/or a biopsy of one of these areas proves cancer has spread and is larger than 0.2mm.
- 21. Staging of breast cancer Classical staging of breast cancer by means of the TNM (tumour–node– metastasis) or UICC (Union Internationale Contre le Cancer) criteria is used less often with increased knowledge of the biological variables that affect prognosis.
- 22. Stage 0 Stage 0 cancers are limited to the inside of the milk duct and are non-invasive (does not invade nearby tissues). Ductal carcinoma in situ (DCIS) is a stage 0 breast tumor. Lobular carcinoma in situ (LCIS) used to be categorized as stage 0, but this has been changed because it is not cancer. Still, it does indicate a higher risk of breast cancer.
- 23. In situ carcinoma It is a preinvasive cancer that has not breached the epithelial basement membrane. This was previously a rare, usually asymptomatic, finding in breast biopsy specimens but is becoming increasingly common because of the advent of mammographic screening; It may be ductal (DCIS) or lobular (LCIS). Although mastectomy is curative, this constitutes overtreatment in many cases. Patients with a high score benefit from radiotherapy after excision, whereas those of low grade, whose tumour is completely excised, need no further treatment. Tumours are also stained for Her-2 or c-erbB2 (a growth factor receptor) as patients who are positive can be treated with the monoclonal antibody trastuzumab (Herceptin®), either in the adjuvant or relapse setting.
- 24. Stages I-III Treatment for stages I to III breast cancer usually includes surgery and radiation therapy, often with chemo or other drug therapies either before (neoadjuvant) or after (adjuvant) surgery. Stage I: These breast cancers are still relatively small and either have not spread to the lymph nodes or have only a tiny area of cancer spread in the sentinel lymph node (the first lymph node to which cancer is likely to spread). Stage II: These breast cancers are larger than stage I cancers and/or have spread to a few nearby lymph nodes. Stage III: These tumors are larger or are growing into nearby tissues (the skin over the breast or the muscle underneath), or they have spread to many nearby lymph nodes.
- 25. Treatment of cancer of the breast The two basic principles of treatment are to reduce the chance of local recurrence and the risk of metastatic spread. Treatment of early breast cancer will usually involve surgery with or without radiotherapy. Systemic therapy such as chemotherapy or hormone therapy is added if there are adverse prognostic factors such as lymph node involvement, indicating a high likelihood of metastatic relapse.
- 26. Algorithm for management of operable breast cancer Achieve local control Appropriate surgery Wide local excision (clear margins) and radiotherapy, or Mastectomy ± radiotherapy (offer reconstruction – immediate or delayed) Combined with axillary procedure Await final pathology and receptor measurements Use risk assessment tool; stage if appropriate Treat risk of systemic disease Offer chemotherapy if prognostic factors poor; include Herceptin if Her-2 positive Radiotherapy Hormone therapy if oestrogen receptor or progesterone receptor positive.
- 27. Treatment of advanced (Metastatic) Breast Cancer What is advanced stage ? If cancers have spread (metastasized) beyond the breast and nearby lymph nodes to other parts of the body stage IV. Treatment can often shrink tumors (or slow their growth), improve symptoms, and help some women live longer. These cancers are considered incurable.
- 28. For women with stage IV breast cancer, systemic drug therapies are the main treatments. Hormone therapy Chemotherapy (chemo) Targeted drugs Immunotherapy Some combination of these Surgery and/or radiation therapy may be useful in certain situations
- 29. RADIOTHERAPY Radiotherapy is shown to decrease the risk of locoregional and systemic recurrence and improve survival. The indication includes the following;- Patients with locally advanced breast cancers T3,T4,N1,N2,N3 disease, Following breast concervative surgery After mastectomy if tumour size > 5cm,skin or chest wall involvement,lymphovascular invasion present. Or axillary lymphnodes positive for metastasis.
- 30. CHEMOTHERAPY This is the most common systemic treatment for breast cancer. Regimens Cyclophosphamide(C) ,Methotraxate (M),and 5-fluorouracil(F) (CMF) Anthracycline-based regimen : CAF (A,Adriamycin[doxorubicin]),CEF(E,epirubicin ) Taxane(docetaxel,paclitaxel)-based regimens. Adjuvant chemotherapy is indicated for all invasive carcinoma >1cm in diameter,tumours >0.5 cm with poor prognostic factors and node positive tumours.
- 31. Systemic (drug) treatments for stage IV breast cancer Treatment often continues until the cancer starts growing again or until side effects become unacceptable. If this happens, other drugs might be tried. The types of drugs used for stage IV breast cancer depend on the hormone receptor status, the HER2 status of the cancer, and sometimes gene mutations that might be found.
- 32. Hormone receptor-positive cancers Women with hormone (estrogen or progesterone) receptor-positive cancers are sometimes treated first with hormone therapy (tamoxifen or an aromatase inhibitor). This may be combined with a targeted drug such as a CDK4/6 inhibitor, everolimus, or a PI3K inhibitor. Women who haven’t yet gone through menopause are often treated with tamoxifen or with medicines that keep the ovaries from making hormones along with other drugs.
- 33. Hormone receptor-negative cancers Chemo is the main treatment for women with hormone (estrogen and progesterone) receptor-negative cancers, because hormone therapy isn’t helpful for these cancers.
- 34. HER2-positive cancers The first therapy given is usually chemotherapy in combination with trastuzumab (Herceptin) and pertuzumab (Perjeta), both HER2 targeted drugs. If the cancer grows, other options might include: ◦ an antibody-drug conjugate ◦ a kinase inhibitor with an anti-HER2 drug or with a chemo drug or both ◦ other HER2 targeted drugs with chemo Hormone therapy might be added to these drug combinations if the cancer is also hormone-receptor positive.
- 35. HER2-low cancers For breast cancers that are considered HER2-low, and have spread to distant sites, the antibody- drug conjugate fam-trastuzumab deruxtecan (Enhertu) might be an option.
- 36. HER2-negative cancers in women with a BRCA gene mutation These women are typically treated with a targeted drug called a PARP inhibitor, such as olaparib or talazoparib. Chemotherapy drugs and hormone drugs are also very helpful in treating these cancers.
- 37. HER2-negative breast cancers in women with a PIK3CA gene mutation About 30% to 40% of metastatic ER-positive breast cancers have a PIK3CA gene mutation. Alpelisib is a targeted drug known as a PIK3 inhibitor that can be used along with the hormone drug fulvestrant to treat postmenopausal women with advanced hormone receptor-positive breast cancer. For this drug to work, there must be a PIK3CA mutation found on a biopsy done on the tumor tissue or of the cancer cells in the blood (liquid biopsy).
- 38. Triple-negative breast cancer (TNBC) An immunotherapy drug along with chemotherapy might be used in people with advanced triple-negative breast cancer whose tumor makes the PD-L1 protein. For women with TNBC and a BRCA mutation, drugs called PARP inhibitors (like olaparib or talazoparib) may be considered. For breast cancers in which the cancer cells show high levels of gene changes called microsatellite instability (MSI) or changes in any of the mismatch repair (MMR) genes (MLH1, MSH2, MSH6, and PMS2), immunotherapy with the drug pembrolizumab might be used. Pembrolizumab might also be an option for TNBC that has other gene or protein changes. For TNBC that does not have any specific gene or protein changes, chemo alone or the antibody-drug conjugate sacituzumab govitecan (Trodelvy) might be an option.
- 39. Local or regional treatments for stage IV breast cancer Although systemic drugs are the main treatment for stage IV breast cancer, local and regional treatments such as surgery, radiation therapy, or regional chemotherapy are sometimes used as well. These can help treat breast cancer in a specific part of the body, but they are very unlikely to get rid of all of the cancer. These treatments are more likely to be used to help prevent or treat symptoms or complications from the cancer. Radiation therapy and/or surgery may also be used in certain situations, such as: ◦ When the breast tumor is causing an open or painful wound in the breast (or chest) ◦ To treat a small number of metastases in a certain area, such as the brain ◦ To help prevent or treat bone fractures ◦ When a cancer is pressing on the spinal cord ◦ To treat a blood vessel blockage in the liver ◦ To provide relief of pain or other symptoms anywhere in the body
- 40. Advanced cancer that progresses during treatment Treatment for advanced breast cancer can often shrink the cancer or slow its growth (sometimes for many years), but after a time, it tends to stop working. ◦ For hormone (estrogen or progesterone) receptor-positive cancers that were being treated with hormone therapy, switching to another type of hormone therapy sometimes helps. ◦ If the cancer is no longer responding to any hormone drugs, chemotherapy immunotherapy, or PARP inhibitors might be options depending on specific features of the cancer or any gene changes that might be present.
- 41. HER2-positive cancers that no longer respond to trastuzumab (Herceptin) might respond to other drugs that target the HER2 protein. Options for women with HER2-positive cancers might include: ◦ Pertuzumab (Perjeta) with chemo and trastuzumab ◦ Ado-trastuzumab emtansine (Kadcyla) ◦ Fam-trastuzumab deruxtecan (Enhertu) ◦ Margetuximab (Margenza) with chemo ◦ Lapatinib (Tykerb) and the oral chemo drug capecitabine ◦ Lapatinib and an aromatase inhibitor (for hormone receptor-positive cancers) ◦ Neratinib (Nerlynx) and the chemo drug capecitabine (this combination can be helpful for cancers that have spread to the brain) ◦ Tucatinib (Tukysa), trastuzumab, and the chemo drug capecitabine (this combination can be helpful for cancers that have spread to the brain)
- 42. References Bailey & Love's Short Practice Of Surgery, 27Th Edition Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61-70. doi:10.1038/nature11412. Henry NL, Shah PD, Haider I, Freer PE, Jagsi R, Sabel MS. Chapter 88: Cancer of the Breast. In: Niederhuber JE, Armitage JO, Doroshow JH, Kastan MB, Tepper JE, eds. Abeloff’s Clinical Oncology. 6th ed. Philadelphia, Pa: Elsevier; 2020. Jagsi R, King TA, Lehman C, Morrow M, Harris JR, Burstein HJ. Chapter 79: Malignant Tumors of the Breast. In: DeVita VT, Lawrence TS, Lawrence TS, Rosenberg SA, eds. DeVita, Hellman, and Rosenberg’s Cancer: Principles and Practice of Oncology. 11th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2019. National Cancer Institute. Physician Data Query (PDQ). Breast Cancer Treatment – Health Professional Version. 2021. Accessed at https://www.cancer.gov/types/breast/hp/breast-treatment-pdq on August 30, 2021. National Comprehensive Cancer Network (NCCN). Practice Guidelines in Oncology: Breast Cancer. Version 7.2021. Accessed at https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf on August 30, 2021.