
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ocular surface neoplasia (OSSN)- Case report
Similar to Ocular surface neoplasia (OSSN)- Case report (20)
More from Dr. vijay pratap
Recently uploaded
Recently uploaded (20)
Ocular surface neoplasia (OSSN)- Case report
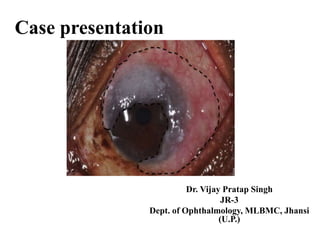
- 1. Case presentation Dr. Vijay Pratap Singh JR-3 Dept. of Ophthalmology, MLBMC, Jhansi (U.P.)
- 2. Personal information • Name- Gendarani • Age- 65 year • Sex- Female • Add- Kochabhawanr, navabaad, Jhansi u.p. • MRD No.- 35799
- 3. Chief complains • Flashy mass growing towards cornea right eye Х 2 Months • Redness (RE) Х 2 Months
- 4. History of present illness • According to patient’s she was apparently asymptomatic 2 month back when she developed flashy mass growing towards cornea on right eye which was gradual onset, rapid progressive and painless in nature and associated with DOV, redness and F.B. sensation in right eye. • She also complains on and off and mild to moderate grade fever not associated with chills, rigor and rashes. • There is no history of trauma, discharge, watering, and other ocular complains
- 5. Past history • Past history- No history of DM, HTN, TB, and any other chronic illness. • No history of significant weight loss. • No history on Chemo-radiation exposure.
- 6. Family history • No significant family history
- 7. Personal history • Strict vegetarian by diet. • Non alcoholic, non-smoker. • Bladder, bowel habit -N
- 9. General examination Inspection- • Patient well oriented, conscious, no neurological deficit seen. • No skin lesions seen. Palpation- • Abdomen –soft, non-tender • No organomegaly noticed. • No palpable lymph nodes or skin lesions seen
- 10. Vitals • Pulse rate- 92/ min • Respiratory rate- 19/min • Temperature- 37.4 c • BP- 140/100 mm of Hg
- 11. Ocular examination • Head- centrally placed. • Forehead – B/L symmetrical. Right eye Left eye Vision 6/60 6/18 Perception of light + + Projection of light Present in all quadrant Present in all quadrant Orbital margin Intact on palpation Intact on palpation Eye lid and lashes WNL WNL Ocular movement WNL in all direction WNL in all direction Conjunctiva and sclera Flashy mass growing from Upper fornix and covering over upper half of the cornea Muddy Cornea Clear AC ND ND
- 12. Right eye Left eye Iris Seems to normal colour and normal pattern Normal colour and normal pattern Pupils R/R/R R/R/R Lens Grayish white reflex Grayish white reflex Fundal glow Poor Poor Fundus Could not be assessed due to hazy media Media hazy Disc-wnl FR- dull Rest wnl BCVA (Pre-op.) 6/24 6/12
- 13. Investigation • Slit lamp- A flashy mass arising from bulbur conjunctiva and enchoroding over upper half of the cornea with high vascularity. • USG B-scan- echogenic lens with vitreous deneration no sign of intraocular masses both eye • Chest X-ray- No significant abnormality seen
- 14. Blood investigations Hb 12.7 gm/dl TLC 11000 cells/mm3 Platelet count 69000 cells/mm3 DLC N-65 L-30 E-04 M-01 B-00 PLATELET COUNT 3.29 Lac cells/ mm3 ESR 18 mm/1st hour (wintrobe) BT & CT 2:10 min, 3:40 min RBS 85 mg/dl Serum urea 19.4 mg/dl Serum creatinine 0.93 mg/dl HbsAg NR HIV NR
- 15. Provisional diagnosis • On behalf of history, examination and investigation – Ocular surface squamous neoplasia (OSSN)
- 16. Differential diagnosis The differential diagnosis of OSSN includes :- • Pannus • Actinic disease • Vitamin A deficiency • Benign intraepithelial dyskeratosis • Pinguecula • Pterygium • Pyogenic granuloma • Keratoacanthoma • Pseudoepitheliomatous hyperplasia • Malignant melanoma and nevi
- 17. Treatment • Medical management- Immunosuppressant drugs like Mitomycin-c and Cyclosporine. • Surgical management- excision biopsy Outcome - 3rd post-op. day BCVA- 6/12
- 18. OSSN Ocular Surface Squamous Neoplasia (OSSN) was a term given by Lee and Hirst which has three grades :- I. Benign dysplasia • Papilloma • Pseudotheliomatous hyperplasia • Benign hereditary intraepithelial dyskeratosis II. Preinvasive OSSN • Conjunctival/corneal carcinoma in situ III. Invasive OSSN • Squamous carcinoma • Mucoepidermoid carcinoma
- 19. Imaging modalities • Optical coherence tomography (OCT) has been employed as an in vivo diagnostic modality in the detection of OSSN. There are distinctive features of OSSN, such as hyper reflectivity, thickened epithelium, and abrupt transition from normal to abnormal tissue seen on ultra high resolution OCT that differentiates it from other conjunctival lesions such as pterygia. • Impression cytology have been reported in the literature as a noninvasive method to diagnose and clinically monitor patients with OSSN. However, it can only assess superficial tissue and is unable to discern the depth of involvement. • Confocal microscopy has also been reported to be helpful in guiding treatment since it is able to reveal cellular details. Its disadvantages include difficulty of use and limited field of view. • High frequency ultrasound may be helpful in determining the extent of invasion into the eye in cases of SCC.
- 20. Prognosis • The recurrence rate of OSSN after surgical excision can occur in over half of cases and may occur years later. The rate of recurrence is substantially higher in the setting of positive surgical margins. Even if the surgical margins are negative, up to one- third of eyes may experience a recurrence within 10 years. The conjunctival lesions that tend to fare the worst involve over half of the limbal stem cells. • A recurrent OSSN can grow rapidly and be more invasive, and thus needs to be treated with aggressive medical, surgical, or combination therapy. The conjunctival lesions that tend to fare the poorest involve over half of the limbal stem cells. Overall, SCC is generally associated with local invasion rather than wide- spread systemic metastases.
- 21. • The overall prognosis in OSSN is good. Modern treatment strategies are effective with local recurrence rates reported to be 5% and regional lymph node metastasis at <2%. Aggressive variants like muco-epidermoid and spindle cell carcinoma and OSSN in immunocompromised patients have a worse prognosis.