2. TABLE OF CONTENTS
• Definition
• Introduction
• Age range and sex ratios
• Aetiology
• Incidence
• Histopathology
• Clinical features
• Management
• Prevention
3. DEFINITION
• Chondroblastoma refers to a benign bony tumor that is caused by the
rapid division of chondroblast cells which are found in the epiphysis
of long bones. They have been described as calcified chondromatous
giant cell tumors.
4. INTRODUCTION
• It is a, benign, locally aggressive, chondroid neoplasm .
• Affects the epiphyses or apophyses of long bones.
• Usually before physeal closure.
• It is thought to arise from an outgrowth of immature cartilage cells
(chondroblasts) from secondary ossification centers.
• Highly cellular, vascular,cartilaginous tumour of cancellous bone.
• Also known as Codman ‘s tumour.
5. AGE RANGE AND SEX RATIOS
• Increased male
preponderance.
• More common in the
second decade of life.
7. HISTOPATHOLOGY
• Lobular appearance: Due to eosinophilic
matrix production which may be
alternating in some areas and merging
in some other areas.
• Cancellous bone is destroyed and
multiple calcium deposits are present
within the tumour.
• Tumour cell produced matrix-pink and
hyaline- > chondroid appearance.
8. • ‘Chicken wire Calcification ‘-connected network of pericellular
calcification.
9.
10. CLINICAL FEATURES
SYMPTOMS
• Pain
• Swelling
• Limp - when lower extremities are
affected
• Joint stiffness.
• Pathological fractures-rare.
• In cases involving the temporal
bone, tinnitus, dizziness, and hearing
loss have been reported.
11.
12. ON EXAMINATION:
• Localized tenderness
• Decreased range of motion in the involved bone and
nearby joint
• Muscle atrophy
•A palpable mass,
• Soft tissue swelling,
• joint effusion in the affected area
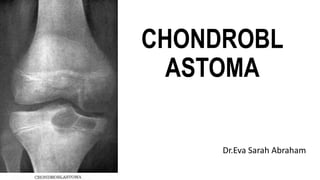
13. RADIOLOGICAL FINDINGS
• Well-defined eccentric lytic lesion that usually involves the
adjacent bone cortex without periosteal reaction.
• A surrounding sclerotic margin can be seen .
• Most lesions are less than 4 cm.
• A mottled appearance on the radiograph , indicates areas
of calcification which is commonly associated with skeletally
immature patients.
• Secondary aneurysmal bone cysts may occur as a result of
stress, trauma or hemorrhage.
17. MANAGEMENT
• Small lesions:Surgical curettage of the lesion with bone grafting.
• Large lesions:excision.
• In skeletally immature patients intraoperative fluoroscopy may be
helpful to avoid destruction of the epiphyseal plate.
• Depending on the size of the subsequent defect,bone grafts are the
preferred filling materials.
• Alternative options: polymethylmethacrylate (PMMA) or fat
implantation in place of the bone graft.
• Radiofrequency ablation has been used, but is typically most
successful for small chondroblastoma lesions.
18. REFERENCES
• Essential Orthopaedics; Maheshwari and Mhaskar
• Mercer's Textbook of Orthopaedics and Trauma
• Robbins and Cotran:Pathologic basis of disease
• Lovell and Winter's Pediatric Orthopaedics, Volume 1
• John Ebenezer Textbook of Orthopaedics
• Orthopaedics And Trauma; M.N.Kumar
• Campbell's Operative Orthopaedics, Volume 2