
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Complex Role of Methadone in Opioid Substitution Treatment
Similaire à Complex Role of Methadone in Opioid Substitution Treatment (20)
Dernier
Dernier (20)
Complex Role of Methadone in Opioid Substitution Treatment
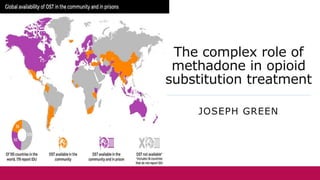
- 1. The complex role of methadone in opioid substitution treatment JOSEPH GREEN
- 2. Introduction Diamorphine (heroin) is a semi synthetic opioid. Highly effective in pain relief due to its analgesic and sedatory properties. Highly addictive (5x more than morphine). Facilitates a state of dependence and tolerance in users. Estimated 9.2 million illicit heroin users worldwide. Most commonly used illicit opioid in Europe. UK has the highest usage within this continent.
- 3. Overcoming addiction Dependent users may make a conscious decision to abstain from the drug. Abrupt cessation - The individual suddenly discontinues their heroin usage. Unpreferred as it triggers intense withdrawal symptoms that are only alleviated by administering heroin. Opioid Substitution Therapy (OST) - The individual is prescribed a legal synthetic opioid which they can use as a “safer alternative to heroin”. Preferred as this supplementation minimises or completely eliminates withdrawal.
- 4. Methadone Utilised as a substitute drug for the longest period of time. Synthetic opioid consisting of an S-enantiomer and R-enantiomer. Full opioid agonist that binds to central and peripheral Mu (μ) receptors. Activates the same biochemical pathways as heroin metabolites and induces identical effects within the body after oral administration. These effects typically last 24 hours.
- 5. Methadone treatment Maintenance (Long term programme). Enable patients to transition from using heroin to using methadone. Provided with a starting dosage which is increased until a point where the patient is stabilised and their withdrawal symptoms are effectively controlled. Detoxification (Short term programme). Enables patients to completely abstain from opioids both legal and illegal. Patient is stabilised in the same manner as in maintenance before their dosage is decreased until the end point where it is stopped completely.
- 6. Role(s) of methadone Reduces the likelihood of contracting and spreading infectious diseases associated with heroin usage. Improves mental and social functioning to facilitate stabilisation of their life. Reduces criminal behaviour related to the; manufacture, distribution and possession of heroin.
- 7. Challenging methadone's role Buprenorphine was introduced into the NHS later than methadone. Partial agonist towards mu (μ) receptors. Active effect at these receptors for between 24-72 hours. Lower overall potency than methadone and induces a ceiling effect. Reduced opioid effects and decreased potential for misuse and addiction. Precipitated withdrawal and trivial effectiveness in severe dependence. NICE guidelines recommend methadone as the first-line option in OST.
- 8. Relation to employment Opioid substitution treatment was chosen as it relates to both my current employment and future aspirations. Contracted to a community pharmacy that offers both methadone and buprenorphine to those dependent on heroin. Desire to study public health at postgraduate level and ultimately work in this area of science.
Notes de l'éditeur
- My PowerPoint pertains to the complex role of methadone in opioid substitution treatment which may also be referred to as opioid substitution therapy in other countries.
- Diamorphine otherwise referred to as heroin is a semi-synthetic opioid derived from morphine which is obtained from the dried latex of the opium poppy. It is highly effective in pain relief and is medically used to alleviate pain associated with surgery and cancer. However it is highly addictive and induces both dependence and tolerance, so not only does the individual keep taking the drug they have to do so in continuously higher doses to maintain an effect. Therefore there is a high potential for misuse and this is a worldwide problem but from a more focused perspective most recent studies estimate that the prevalence of heroin use in the UK is 8 people aged 15-64 per every 1000 in this age bracket.
- Addiction is not always lifelong or fatal biopsychosocial disorder as those with heroin dependency may reach a point where they wish to abstain from the drug. This goal may be achieved through abrupt cessation where the individual suddenly stops using the drug. This is unpreferred as it triggers psychological and physical changes such as anxiety, restlessness, sweating, gastrointestinal cramps among others and these can only be stopped through relapse. It may also be achieved through “opioid substitution treatment” where the individual is prescribed a synthetic opioid which they can use instead of heroin. This is preferred as it minimises or completely eliminates withdrawal therefore reducing the likelihood of relapse.
- Out of its current and past counterparts, methadone has historically been utilised as a substitute for the longest period of time and been the drug of choice for this purpose. It binds to mu receptors in the same manner as 6-monoacetylmorphine and morphine to dissociate its bound G-protein into individual subunits. These subunits subsequently open potassium channels, close calcium channels and prevent the formation of cyclic-AMP, all of which lead to reduced; production of neurotransmitter, neuronal excitability and nociception of signals, particularly those related to pain and behaviour.
- Methadone has two clearly defined pharmacological interventions. The first of which is maintenance. Here the patient is started on a dosage of 10 or 20 mg per day and this is increased in 10 mg increments with a minimum of 3 days between each increase, to finally reach a dosage which sufficiently controls their withdrawal symptoms. This may be as low as 30 mg or as high as 120mg depending on addiction severity. The other method is detoxification. Here this dose is achieved then reduced in 10mg decrements until the starting dosage is reached, when it is then reduced to 5 or 2mg per day until abstinence.
- Aside from the obvious benefit of stopping their heroin usage methadone has a commonly described trio effects. Reduces the likelihood of contracting and spreading infectious diseases associated with heroin usage such as HIV and both variations of hepatitis (B and C). Improves the mental and social functioning of the individual undergoing treatment allowing them to reconcile any relationships and gain employment. Reduces criminal behaviour related to the; manufacture, distribution and possession of heroin and therefore the resources diverted to deal with it.
- Buprenorphine was introduced into the NHS in 1998 and was heralded as a potential replacement to methadone due to its unique pharmacological profile. Partial agonist towards the mu receptors meaning it both activates them and occupies their sites to prevent other opioids from binding. This reduced intrinsic activity is beneficial as it means the drug causes a lesser degree of sedation and analgesia whilst still controlling withdrawal and induces a ceiling effect, meaning these effects only increase with dosage to a certain point, after which the effects will not increase no matter how much drug is administered, reducing the likelihood of addiction and overdose. It is also detrimental though as it induces precipitated withdrawal when first beginning treatment as Buprenorphine displaces and prevents further binding of any circulating opioids from the receptor, so initiating treatment in a individua who has recently taken an opioid (either heroin or methadone) it will always initiate withdrawal symptoms until their body becomes adjusted to the drug. It is also typically ineffective in those with severe dependence as these patients prefer the intense opioid effects. Ultimately was not effective in its purpose as 2019 NICE guidelines recommended methadone over buprenorphine when the patient is eligible for both drugs.
- The concept of methadone and opioid substitution treatment relates to both my current employment and future aspirations I currently work in a community pharmacy that offers OST to a fairly high number of people (50 as of yesterday) most of which are severely dependent and have been on the treatment for a long time, as a result I've seen see first-hand a lot of the most of the information in this PowerPoint. To reiterate the prior points about buprenorphine, only 9 of these individuals take this substitute whilst the remaining 41 take methadone. Upon completion of undergraduate study, I am hoping to study a masters in public health and find a life-long career in this field. This is relevant to the topic as addiction (whether it be to an opioids or something more commonplace like nicotine or alcohol) is resolutely a public health challenge as you need to be aware of the epidemiological data surrounding this problem, devise and ultimately utilise appropriate strategies to reduce it and its related risks.