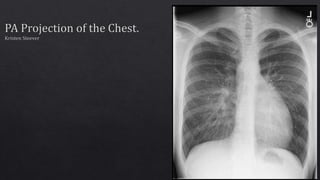
This document evaluates a PA chest x-ray image. It finds that while the image is of diagnostic quality, there are some technical factors that could be improved. Specifically, it notes that the collimation is centered slightly low at T8 instead of the ideal T7 level, and that the patient appears rotated slightly to the right side as their right clavicle and lung field are higher and farther from the spine than the left. The summary provides recommendations to improve patient positioning and centering for future images.
2. • The image is HIPAA compliant .
• There is no evidence of patient information
displayed on this image. Therefore, patient
information has been kept confidential and
has not been violated.
3. • The correct anatomical marker is on the image.
• There are no markers superimposed on pertinent
anatomy.
• An additional marker could be placed on this
image to help indicate that the image was taken in
PA position. An erect marker is not needed since
the three beads in the circle under the
technologist’s initials indicate the patient was
erect.
• Based on marker placement, this image was
displayed correctly. The left marker is on the
correct side of the patient and it appears on the
viewer’s right side. However, the marker should
have been flipped so that the “L” would not appear
backwards on the resulting image. The lettering
should have been facing towards the image
receptor and not towards the technologist.
4. • There must be at least three sides
of beam restriction on the image.
• There appears to be three sides of
beam restriction on this image
because of the white appearance
surrounding the edges.
• The gonads of the patient must be
shielded if they are within 5 cm of
the primary beam. There is
evidence of beam restriction on the
side closest to the gonads.
Beam restriction on side
closest to gonads.
5. Routine Projections:
• PA projection with perpendicular beam
• Lateral Projection with perpendicular beam
All anatomical parts are correctly visualized on this
image. The image includes the whole lung field from
the apices to the costophrenic angles.
6. • The following are not present in this image:
• Preventable artifacts
• Body parts superimposing that should
not be superimposed.
• Hospital paraphernalia.
• Patient belonging artifacts.
• Indwelling foreign bodies.
• CR/DR artifacts.
• Visible excess fog that is degrading the
image quality.
7. • There is no evidence of gross voluntary
movement in this image. Pertinent
anatomy is well defined and does not
appear to be blurred. Lung markings are
seen clearly. However, there may have
been slight movement of the clavicles
due to blurry appearance, but this is not
the anatomy of interest.
• There is no evidence of gross quantum
mottle in this image because a
grainy/mottled appearance is not
present.
• There is no evidence of double exposure
in this image. There is only one marker
and a ghosted image is not present.
• There is no evidence of grid lines/grid
cut-off or grid artifacts in this image. An
oscillating high frequency grid and
proper SID were most likely utilized.
Slight blur indicating
movement of clavicles.
8. • Size distortion does not appear greater than
expected.
• The centering for an erect PA Chest projection is
at T7 (blue star).
• Since the CR in this image is centered inferiorly
to T7, just about on T8, there may be slight
shape distortion. However, the centering is
within 1 cm of proper centering in my opinion,
so shape distortion will not be drastic.
1
2
3
4
5
6
7
8
9. • The part is properly aligned to the long axis of the
image media (red line). The viewer does not have to
tilt their head to see the image in its proper display.
• The part is not accurately centered to the image media.
The CR should be centered at the T7 (blue star). In this
image, the CR is centered to T8 (intersection of yellow
lines).
• I believe the CR is centered within 1 cm of the part.
Therefore, shape distortion is minimal and will not
degrade image quality.
• Assuming that the black edges of the image represent
the image media, the CR appears to be properly
centered to the image media. (intersection of green
lines).
1
2
3
4
5
6
7
8
10. • Since three sides of beam restriction can be seen,
this image follows an appropriate exposure field
template.
1
2
3
11. Position of Patient for an erect
PA Chest:
• If possible, always examine
patients in the upright position,
either standing or seated, so
that the diaphragm is at its
lowest position, and air or fluid
levels are seen. Engorgement of
the pulmonary vessels is also
avoided.
Source: Merrill’s Atlas 13th edition
Volume 1 Pg. 497-498
Position of Part for an erect PA
Chest:
• Place the patient, with arms hanging at
sides, before a vertical grid device.
• Adjust the height of the IR so that its upper
border is about 1.5 to 2 inches (3.8 to 5
cm) above the relaxed shoulders.
• Center the midsagittal plane of the
patient’s body to the midline of the IR.
• Have the patient stand straight, with the
weight of the body equally distributed on
the feet,
• Extend the patient’s chin upward or over
the top of the grid device, and adjust the
head so that the midsagittal plane is
vertical.
• Ask the patient to flex the elbows and to
rest the backs of the hands low on the hips,
below the level of the costophrenic angles.
Depress the shoulders and adjust to lie in
the same transverse plane. These
movements will position the clavicles
below the apices of the lungs.
• Rotate the shoulders forwards so that both
touch the vertical grid device. This
movement will rotate the scapulae
outward and laterally to reduce
superimposition of the scapulae with the
lungs.
• If an immobilization band is used, be
careful not to rotate the body when
applying the band.
Collimation:
• 14 x 17 inches lengthwise.
• Crosswise for hypersthenic patients.
CR:
• Perpendicular to the center of the
IR. The central ray should enetr at
the level of T7 (inferior angle of the
scapula)
SID:
• 72 inches.
• The least amount of rotation results in
considerable distortion of the heart shadow.
• If a female patient’s breasts are large enough
to be superimposed of the lower part of the
lung fields, especially the costophrenic
angles, ask the patient to pull the breasts
upward and laterally. This is especially
important when ruling out the presence of
fluid. Have the patient hold the breasts in
place by leaning against the IR holder.
• Shield gonads. Place a lead strip between
the patient and the x-ray tube.
***SIDE NOTE***
• It is best to place a lead shield in front of the
patient for this projection. This is because
more scatter radiation is being received by the
patient’s gonads anteriorly. The best lead
apron to use would be one that acts as a skirt
that covers the anterior and posterior of the
patient.
• Respiration: Full inspiration. The exposure is
made after the second full inspiration to
ensure maximum expansion of the lungs. The
lungs expand transversely, anteroposteriorly,
and vertically, with vertical being the greatest
dimension.
12. Images from Merrill’s Atlas 13th Edition
Volume 1 Page 496 and 498
Beam restriction
for gonads.
• For certain conditions, such as
pneumothorax and the presence of a
foreign body, radiographs are sometimes
made at the end of full inspiration and
expiration. Pneumothorax is shown more
clearly on expiration because collapse of
the lung is accentuated.
• The above picture demonstrates
Pneumothorax of the right lung with
radiograph taken during expiration.
• Orient the CR
crosswise for
hypersthenic
patients.
13. (Merrill’s Atlas Volume 1 page 394)
Apices
Costophrenic
Angles
The sternal ends of the clavicles
are not equidistant from the
vertebral column. There
appears to be slight rotation to
the patient’s right side, since the
right clavicle is farther away
from the vertebral column.
Trachea in
midline
The right side is wider than the left side.
14. McQuillen Martensen Image Evaluation
(McQuillen Martensen 4th Edition Pg. 88)
1
2
3
4
5
6
7
8
9
10
4th thoracic
vertebra
superimposing
manubrium
About 1 inch of
apical lung field
above clavicle.
Centered at T8
instead of T7
Apices
Costophrenic
Angles
Right border of posterior
ribs are farther from
vertebral column than
left, due to slight rotation
to the right side.
Right clavicle is
slightly higher
than left.
Right sternal clavicular end is farther than left.
15. • The most radiolucent structure in this image is the air
within the lung field and the trachea.
• The most radiopaque structure in this image is the
bony cortex of the spine, ribs, and clavicles.
• The image contrast is adequate in this image since
variations of gray differentiate structures from one
another. The image has a long scale contrast which is
needed for proper visualization of structures of the
thoracic viscera.
• There is no EI value to go with this image, but since
quantum mottle is not seen and structures in the lungs
such as the vessels and heart can be seen, the image's
brightness is adequate to visualize all anatomical
structures necessary.
16. • This image is of diagnostic quality and should not
be repeated. It seems to have an appropriate EI
value and all pertinent anatomy is visualized on
this image.
17. • The marker should be placed so that it should
face in its proper position for the viewer.
• The CR should be centered at T7, not T8.
• Clavicles need to be on the same horizontal
plane. The right clavicle is higher than the left
clavicle.
• The sternal ends of the clavicles must be at an
equal distance from the vertebral column on
both sides. The distance between the vertebral
column and the lateral border of the lungs
must also be equidistant on each side.
• Since the right sternal clavicular end is farther
from the vertebral column than the left, and
the right clavicle is higher on a horizontal
plane than the left, the patient was over
rotated to the right side and should be rotated
slightly more to the left side. This will put both
sternal clavicular ends on the vertebral column
and lung fields will be symmetrical.