Gastric Cancer Surgery Reconstruction
•Télécharger en tant que PPT, PDF•
4 j'aime•5,651 vues

A 60-year-old man presented with dyspepsia for 6 months. Endoscopy revealed a fungating mass in his gastric corpus, and biopsies showed well-differentiated adenocarcinoma. He underwent a total gastrectomy with D1 lymph node dissection and reconstruction using a jejunal interposition. His recovery was uneventful.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Gastric Cancer Surgery Reconstruction
Similaire à Gastric Cancer Surgery Reconstruction (20)
Plus de KurdGEHS
Plus de KurdGEHS (15)
Dernier
Dernier (20)
Gastric Cancer Surgery Reconstruction
- 1. Shorish hospital kurdistan /Iraq . August/2008 . Kalandar 60 years old man ,farmer from sulaimany ,presented with 6 month history of dyspepsia ,for which empiric treatment was not successful. Upper G I T endoscopy has revealed fungating mass in the gasrtic corpu. multiple biobsy was done and it was well differentiated adenocarcinoma of the stomuch helico bacter was positive . Preoperative tumour marker were negative ,and all other investigation was within normal range .ultra sound of the liver was normal and endoscopic ultrasound was in favour of T3 , CHEST AND ABDOMINAL CONTRAST CT scan was not showing any local organ invasion and it was T3 NI M0. Total gastrectomy has been done through oblique upper abdominal incision ,the stages was like C T scan T3N1M0 ,and ( D1 ) resection has been done .Reconstruction has been done by jejunal loop interposition between the esophagus and the duodenum ,putting the loop in retrocolic position,no stomach tube ,a drain was left for 24 hours. Un eventful recovery .for follow up
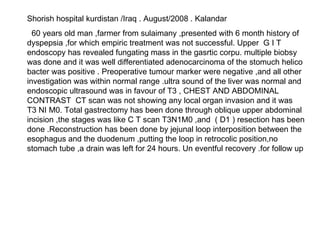
- 2. The tumour Duodenal end Proximal end
- 3. The jejunal loop brought up behind the colon colon The site of the jejunal loop after reconstruction of the bowel continuity
- 4. Proximal single layer anastomosis by polydioxanon ,end to end Distal anastomosis by single layer PDS . End to end
- 5. All anastomosis has been done by extramucosal single layer anastomosis ,using absorbable suture material .exept in the duodenum we use through and through technique single layer.
- 6. 67 years old lady kurd from sulaimany kurdistan regionalgovernment /iraq/,presented with typical gastric outlet obstruction .duration 4 months ,it has become sever for the last month which made the patient to consult . Not smoker no relevant past surgical or medical history ENDOSCOPY has revealed distal gastric tumour of signet ring type and moderately differentiated .image modalities all were in favour of T3 NO MO .the operation was done without laparoscopy because exploration already was mandatory and to scope her is to waste time. classical DI TOTAL GASTRECTOMY has been done and a jejunal loop interposition of 30 cm ,retrocolic has been performed .using as all other cases single layer anastomosis by P D S suture material ,and using extra mucosal technique .no stomach tube has been put ,and sinle tube drain was left in left subphrenic space for some ooze .she had un eventful recovery . NB.2 nd post operative day she had oral fluid because we kept 1 cm of the cardia which is helping the extra mucosal technique depending on the serosa of the cardia . operative finding was T3 NI MO and histopathology has revealed free margins .
- 9. Anastomosis with the cardia
- 11. Shorish hospital kurdistan /Iraq August /2008. kalandar 70 Years old man kurd from sulaimany ,kurdistan ,he was farmer . PRESENTATION.. Anaemia and abdominal discomfort ,2 month duration of his illness, diagnostic work up revealed gastric tumour at the body which was bleeding during the endoscopy. It was exophytic tumour which was bleeding at the gastric corpus, helico bacter pylori was positive ,the histopathology was moderately differentiated adenocarcinoma. Pre operative image assessment and diagnostic laparoscopy were T3 N1 M0 Then exploration by oblique upper abdominal incision was done and ( D1 ) resection has been done and reconstruction was done jejunal loop interposition between esophagus and duodenum .Using single layer end to end ,extramicosal technique by using polydioxanon suture .( N.B in the doudenal end we use to do through and through single layer not extramucosal ). No stomach tube has been used and single drain was left for 24 hours only. Un eventful recovery
- 12. Proximal end Tumour in the body extending to the lesser curve Distal end
- 13. Preparing the jejunal loop
- 14. Passing the loop behind the transverse colon (retrocolic)
- 15. Proximal end to end anastomosis Distal end of the loop with the duodenum the jejunal loop
- 16. Total gastrectomy with reconstruction of the continuity by separated jejunal loop 70 years old man. Farmer from kalar adistrict of kirkuk ,which is part of kurdistan of Iraq. Presented as melaena and anaemia .the upper G I T endoscopy has revealed fungating lesion in the distal part of the stomach which was bleeding obviously and we could not control it by ARGON PLASMA COAGULATOR resuscitation has been done and all investigations including blood picture and biochemistry was normal .chest x ray, E C G and liver function was normal the acid base was not available .s amylase was normal. Contrast C T ABDOMEN AND CHEST was showing the cancer in the middle of the stomach not involving any organ there was a big lymph node near the lesser curve ,no evidence of any metastasis .T3 NI MO . Ultrasound was not showing any liver involvement or ascitis . After the exploration of the abdomen the findings were the same as the pre op images Total gastrectomy was done with reconstruction of the part by jejunal loop inter position ,between the esophagus and the duodenum which was isoperistaltic and retrocolic .using single layer extra mucosal technique using absorbable synthetic suture materials .no stomach tube was lef ,and single drain has been left in the left hypochondrail region.The incision was right sub costal incision extended to the other side .the patient had un eventful recovery carcinoembrionic antigen after one month was normal and so the scope and images Note : pre operative biopsy was moderately differentiated adenocarcinoma and so the specimen after resectio .the margins were free and only single lymph node was involved as showed in the slides.it was gross curative resection at least .
- 17. The tumour reaching middle of the lesser curve Lesser omentum with a lymph node Greater omentum
- 18. Distal end Sub pyloric lymph nodes were free cardia
- 20. Anastomosis of the loop with the cardia Anastomosis of the distal end of the loop with the duodenum pancrease