
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Medical Management of Fibroids, Dr. Sharda Jain
Similar to Medical Management of Fibroids, Dr. Sharda Jain (20)
More from Lifecare Centre
More from Lifecare Centre (20)
Recently uploaded
Recently uploaded (20)
Medical Management of Fibroids, Dr. Sharda Jain
- 1. Medical Management of Fibroids Dr. Sharda Jain Dr. Jyoti Agarwal Dr. Jyoti Bhaskar
- 2. OUR TEAM
- 3. U.S.P. of Fibroids Benign uterine fibroids are the most common pelvic tumor in women ---occur in 20 to 50 % of women . -- ESTIMATED LIFETIME RISK -- 70 percent In white women --- 80 percent in black women.
- 4. Uterine sarcoma is malignant form -- very rare (3 to 7 per 100,000 ) with a poor prognosis. Uterine Sarcoma
- 5. Majority of fibroids in women’s life, remain asymptomatic but some present with Abnormal uterine bleeding (AUB) INFERTILITY , PELVIC PAIN PRESSURE SYMPTOMS.
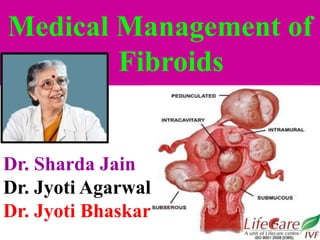
- 6. International Federation of Gynecology and Obstetrics (FIGO) classification of fibroids Submucous 0 Pedunculated intracavitatory 1 < 50% intramural 2 > 50 % intramural Others 3 Contacts endometrium, 100 % intramural 4 Intramural 5 Subserous >50 % intramural 6 Subserous < 50 % intramural 7 Subserous peduculated 8 Others (specify, e.g. cervical , parasitic)
- 7. Infertility Most Gynaecologists feel that R/O fibroids is going to improve fertility but this is not TRUE. Surgery wrongly done-- can cause adhesions, distortion of tubo ovarian relationship, blockage of tubes & then only treatment left is I.V.F.
- 8. Prophylactic therapy to avoid potential future complications from fibroids is NOT recommended except. women with significant submucous fibroids who are contemplating pregnancy. PROPHYLACTIC Treatment of fibroids .
- 9. PROPHYLACTIC Treatment of fibroids . women with ureteral compression leading to moderate or severe hydronephrosis. In these women, prophylactic treatment may prevent miscarriage or urinary tract obstruction.
- 10. Relief of symptoms (eg, heavy bleeding, pain, pressure ) is the major goal in management of fibroids . The type and timing of any intervention should be individualized, based upon factors. •TYPE AND SEVERITY OF SYMPTOMS, •SIZE OF THE FIBROID, • LOCATION OF THE FIBROID, • PATIENT AGE, • REPRODUCTION PLAN • OBSTETRICAL HISTORY. Symptomatic fibroids
- 11. Medical Management of Fibroids with Bleeding Medical therapy provides adequate symptom relief in some women, primarily in situations where bleeding is the dominant or only symptom. In general, 75 percent of women get some improvement over one year of therapy, but long-term failure rates are higher.
- 12. Same medical management of fibroids is effective with pressure symptoms as well Medical Management of Fibroids with Pressure symptoms
- 13. Hormonal Therapy COMBINED OCP and progestational agents are commonalty used in the treatment of HEAVY MENSTRUAL PERIOD Women with heavy menstrual bleeding associated with fibroids Do Respond to OCP therapy. It should be tried before invasive therapy. The mechanism of action is via endometrial atrophy.
- 14. Progestational agents There are NO DATA to show the effectiveness of progestin only contraceptive is specifically USEFUL for treatment of symptomatic fibroids. They can be considered for treatment of MILD SYMPTOMS, especially for women who need CONTRACEPTION.
- 15. Levonorgesrel-releasing intrauterine system (IUS ) Effective Observational studies and systematic reviews have shown a reduction in uterine volume and bleeding, and an increase in hematocrit after placement of this IUS the device
- 16. It is widely used for control of heavy menstrual bleeding and now approved by the US Food and Drug administration (FDA) for this indication . A second advantage of this treatment is that it provides contraception for women who do not desire pregnancy. Levonorgesrel-releasing intrauterine system (IUS ) (Effective)
- 17. Gonadotropine releasing hormone agonists (GnRH agonist ) GnRH agonist are the most effective medical therapy for uterine fibroids. First used by Filicouri in 1983. These drugs work by initially increasing the release of gonadotropine, followed by desensitization and down regulation to a Hypo gonadotropic - hypo gonadal state that clinically resembles menopause.
- 18. Most women will develop amenorrhea, Improvement in anemia is bonus. There is significant reduction (35 to 60 percent) in uterine size within three months of initiating this therapy. However, there is rapid resumption of menses and pretreatment uterine volume after discontinuation of GnRH agonists(short lasting effect). GnRH Agonist
- 19. Hypo estrogenic side effects on long term treatment is a big draw back. A RULE OF THUMB for women with endometriosis is that approximately 6 percent of bone is lost over 12 months of therapy and 3 percent is regained following the cessation of therapy. GnRH – Agonist
- 20. The side effects of long - term GNRH agonist administration can be minimized during therapy by giving ADD - BACK THERAPY with low dose estrogen - progestin after the initial phase of down regulation. GnRH – agonist
- 21. Low dose estrogen - progestin therapy, such as used for menopausal harmone replacement therapy i.e. 0.625 mg of conjugated estrogen and 2.5 of medroxy progesterone acetate or 5 mg norethindrone acetate) Maintains amenorrhea and the reduction in uterine volume, while preventing significant hypo estrogenic side effects. What is this add back therapy to prevent osteoporosis ??
- 22. Can OCP be given as add bad therapy to prevent osteoporosis ?? “No” Using OCP as add- back therapy for fibroids is not indicated.
- 23. Preoperative GnRH analogs use is not recommended before myomectomy except in cases of severe anaemia
- 24. GnRH - antagonist The advantage of antagonists over agonists is the rapid onset of clinical effects without the characteristic initial flareup observed with GNRH agonist treatment
- 25. GnRH - antagonist However, in the United States these agents are marketed at doses used for ovulation induction and long-acting preparations are not available . Thus , treatment of fibroids is cumbersome due to the need for daily injections.
- 26. Progesterone receptor modulators - drugs that modulate progesterone are increasingly used for medical treatment of fibroids. However, they not yet approved by the US Food and Drug Administration (FDA). They have the advantage of oral administration and minimal symptomatic side effects. The major concern is whether there are endometrial effects with long - term use. Progesterone Receptor modulator (PRM)
- 27. Ulipristal acetate is a progesterone receptor modulator (PRM) that Inhibits Ovulation, but has little impact on serum estradiol levels. The drug is approved for three months of preoperative therapy outside USA. Ulipristal Acetate Fertil. Steril 2014,101;1565
- 28. Ulipristal Acetate Ulipristal acetate (oral, 5 mg or 10 mg once daily for 13 weeks ) was compared with placebo in one randomized trial of 242 women with menorrhagia Fibroid – associated anemia improved, and uterus size decreased. Fertil. Steril 2014,101;1565
- 29. Mifepristone (RU - 486) is the most widely studied Progesterone Receptor Modulator and reduces uterine volume by 25 to 75 percent in women with fibroids, which is comparable to the reduction observed with GnRH agonists. Re growth occurs slowly following cessation of the drug. Mifepristone ( Ru- 486)
- 30. Raloxifene - The efficacy of selective estrogen receptor modulators for treatment of fibroids is unclear. Raloxifene
- 31. Danazol and gestrinone which are potent Androgenic steroids may be an effective treatment of fibroids symptoms in some women are associated with severe androgenic side effects. Danazol & Gestrinone
- 32. Nonsteroidal antiinflammatory drugs Nonsteroidal antiinflammatory drugs (NSAIDs) have not been extensively studied in fibroids – related menorrhagia. NSAIDs do not appear to reduce blood loss in women with fibroids but provide relief in painful periods.
- 33. Antifibrinolytic agents Antifibrinolytic agents, which are useful in the treatment of idiopathic menorrhagia, have not been well studied in fibroids – related menorrhagia.
- 34. Conclusion Most common pelvic tumor. All fibroids are not symptomatic still fibroids are blamed for infertility, abnormal bleeding, lower abdomen pain etc.
- 35. Conclusion Medical treatment of fibroids does not improve fertility Medical treatment fibroids causing heavy periods & presser symptoms is effective but still evolving. Preoperative GnRH anologs use is not recommended except in cases severe anemia
- 37. ADDRESS 11 Gagan Vihar, Near Karkari Morh Flyover, Delhi - 51 CONTACT US 9650588339 011-22414049 WEBSITE : www.lifecareivf.in www.lifecarecentre.in ISO 14001:2004 (EMS) …..Caring hearts, healing hands ISO 9001:2008 Helpline : 9599044257 Web.www.lifecareivf.in Helpline : 9910081484