
Recommandé
Contenu connexe
Tendances
Tendances (18)
En vedette
En vedette (20)
Similaire à HHL_7-7-14_web
Similaire à HHL_7-7-14_web (20)
HHL_7-7-14_web
- 1. Home Health Line | 9737 Washingtonian Blvd., Ste. 200 | Gaithersburg, MD 20878-7364 | 1-855-CALL-DH1 IN THIS ISSUE Home Health LineRegulatory news, benchmarks and best practices to build profitable home care agencies homehealthline.com July 7, 2014 | Vol. 39, Issue 26 Benchmark of the Week CMS will release new OASIS-C1 guidance manual any day. Are you ready? CMS is moving full speed ahead with OASIS- C1, effective Jan. 1. Make sure you are ready by signing up for the 10th Annual National Quality Outcomes OASIS-C Conference Sept. 15 to 18 in Chicago. Save $300 by signing up by July 7 at www.homecareoutcomesconference.com. Opposition mounting against Part D plans’ role in deciding hospice drug coverage.............................1 CMS’ provider relations coordinator to help agencies with contractors..................................1 Require clinicians to turn in same-day documentation to avoid deficiencies..........................2 Use objective measurements to document required therapy reassessment visits........................3 Make it essential for staff to submit documentation in a timely fashion..............................4 Learn from the past, prepare for the future with revised timelines......................................4 Most common referral sources for home health agencies...........................................................5 Having same nurses, aides visit ALFs each time will strengthen relationships..............................6 Proposed PPS rule would trim payments, ease face-to-face burden....................................................8 Hospice compliance Opposition mounting against Part D plans’ role in deciding hospice drug coverage The hospice industry now has nearly four dozen organiza- tions — including the Medicare Payment Advisory Commission, AARP and the American Medical Association, the National Association for Home Care and Hospice and the National Hospice and Palliative Care Organization — joined in opposi- tion to CMS instructions which would require that Part D drug plans preauthorize drugs needed by hospice patients. (see Part D, p. 7) Denials management CMS’ provider relations coordinator to help agencies with contractors You now have a new CMS resource to turn to when you expe- rience problems with recovery audit contractors (RACs) and other contractors. The new staff position, which CMS announced last month, is designed to “increase program transparency and offer more efficient resolutions to providers affected by the medical review process,” CMS says. The provider relations coordinator will “improve communication between providers and CMS.” (see Coordinator, p. 8)
- 2. July 7, 2014 Home Health Line Exclusive web content and searchable CMS documents at www.homehealthline.com.2 Subscriber Information Have questions on a story? Call or email us. EDITORIAL Have questions on a story? Call or email: PLEDGE OF INDEPENDENCE At DecisionHealth, the only person we work for is you, the provider. Home Health Line is not affiliated with any special interest groups, nor owned by any entity with a conflicting stake in the healthcare industry. For nearly three decades, we’ve been independently watching out for the financial health of healthcare providers, and we’ll be there for you and your peers for decades to come. WEBSITE www.homehealthline.com SUBSCRIPTIONS Direct questions about newsletter delivery and account status, toll free, to 1-855-CALL-DH1 or email: customer@decisionhealth.com. ADVERTISING To inquire about advertising in HHL, call Elizabeth Christian, 1-301-287-2232. COPYRIGHT WARNING Copyright violations will be prosecuted. Home Health Line shares 10% of the net proceeds of settlements or jury awards with individuals who provide essential evidence of illegal photocopying or electronic redistribution. To report violations, contact our copyright attorney Steve McVearry at 1-301-287-2266 or email smvearry@ucg.com. REPRINTS To request permission to make photocopy reprints of Home Health Line articles, call 1-855-CALL-DH1 or email customer service at customer@decisionhealth.com. Also ask about our copyright waiver, multiple copy and site license programs by calling the same number. Home Health Line is a registered trademark of DecisionHealth. DecisionHealth is a registered trademark of UCG. Home Health Line is published 48 times/year by DecisionHealth, 9737 Washingtonian Blvd., Ste. 200, Gaithersburg, MD 20878. ISSN 0893-8121. Price: $597/year. © 2014 UCG DecisionHealth Product Manager: Maria Tsigas, 1-301-287-2305 mtsigas@decisionhealth.com President: Steve Greenberg 1-301-287-2734 sgreenberg@decisionhealth.com Vice President: Corinne Kuypers-Denlinger 1-301-287-2363 ckuypers-denlinger@decisionhealth.com Senior Content Manager: Marci Heydt, 1-301-287-2299 mheydt@decisionhealth.com Senior Editor: Burt Schorr 1-240-497-0392 burt.schorr@verizon.net Editor: Laura Thornton 1-301-287-2584 lthornton@decisionhealth.com Editor: Josh Poltilove 1-301-287-2593 jpoltilove@decisionhealth.com CMS survey penalties Require clinicians to turn in same-day documentation to avoid deficiencies Have clinicians complete their electronic clinical documentation during or right after each visit. That step can protect you from ramped up state surveyor scrutiny on documentation timeliness. In the past two months, two home health agencies in CMS Region 9 received multiple condition-level deficiencies, including G236 (failed to maintain client clinical records that met accepted professional standards) and G123 (Organization, services furnished, administrative control and lines of authority for the delegation of responsibility down to the patient care level are clearly set forth in writing and are readily identifiable), says Michael McGowan, senior consultant/ expert witness at Medicare Appeals Development, based in Albuquerque, N.M. Region 9 includes Nevada, American Somoa, Arizona, California, Guam, Hawaii and the Northern Mariana Islands. Agencies in both cases were using electronic medical record (EMR) systems and had policies that required clinical documentation to be turned in within a week, a policy not acceptable or sufficient to meet professional standards to surveyors because a patient who was declining could be in jeopardy without the agency knowing it, McGowan says. That’s a warning to all agencies as state surveyors recently gained the authority to hand out civil monetary penalties for as much as thousands of dollars a day for repeat standard- and condition-level deficiencies. The push to adopt EMRs in all areas of health care has led to an increased expectation from state surveyors that home health agencies should be using these systems as designed in terms of completing documentation during or directly following the visit, says McGowan. Doing so ultimately leads to better care coordination with colleagues and clinical supervisors. In its plan of correction, one of the agencies McGowan advised must now adhere to a policy of having clinicians turn in clinical documentation within 72 hours or potentially be terminated from Medicare pending an appeal to an Administrative Law Judge, he says. Still, he suggests documentation should be done the same day. Paper documentation needs to be timely Agencies that are still on paper should follow the same advice and turn in documentation on the same day in order to adhere to the same professional standards required in Medicare’s Conditions of Participation and by state nursing licensing boards, says McGowan. At Sutter Care at Home, a not-for-profit home care and hospice agency based in Emeryville, Calif. with branches in 24 counties in northern California, leadership recently approved a written company policy that the agency’s roughly 1,000 clinicians must submit clinical
- 3. Home Health Line July 7, 2014 © 2014 DecisionHealth® | www.decisionhealth.com | 1-855-CALL-DH1 3 documentation via mobile tablets to the agency’s EMR, Dallas-based Homecare Homebase, within 24 hours. This policy excludes one rural branch that is still on paper and whose clinicians have to drive long distances to treat patients, says Sandy Sanville, director of clinical practice for Sutter Care at Home. Those clinicians must turn in their documentation within 48 hours, says Paula Suter, director of clinical care management for the Sutter Center of Integrated Care, Sutter Care at Home. Tips for timely documentation •• Work out a comfortable routine for completing documentation. Have clinicians use their cars as a makeshift office to complete documentation for about 10 to 15 minutes after each visit and before they go to their next visit, says McGowan. Alternatively, have them go to a park, library or favorite coffee shop mid-day to complete documentation on morning patients, and do the same in the afternoon, he says. The idea is that they should not go home without completing that day’s documentation. •• Show clinicians how timely documentation can improve their quality of life. One clinician at Sutter Care at Home was not comfortable using mobile tablets and resisted charting in the home, says Sanville. Her supervisors asked her to use the point-of-care device during the visit after she received more training, she says. Once the employee began to document in the home, she realized it made her life more efficient. •• Use EMRs as a tool to train clinicians on documentation. Many EMR systems allow quality improvement staff and clinical supervisors to determine how much time was spent on documentation and how much time was spent on submission, says Sanville. Quality managers can use this feature to train clinicians in a more targeted way. — Nicholas Stern (nstern@ decisionhealth.com) Therapy reassessments Use objective measurements to document required therapy reassessment visits Reduce your risk for costly denials associated with the therapy reassessment requirement by conducting tests like the 30-second chair stand test. Tests such as these have been proven to reduce agencies’ average per-record risk by $672, according to a study by Northampton, Mass.-based Fazzi Associates that looked at more than 3,000 therapy reassessment records from over 60 agencies between August 2011 and June 2012. The content of the reassessments, including proper documentation to support the services, was one of the largest issues agencies had prior to receiving education on the topic. The chair stand test is one example of a way to objec- tively measure lower extremity weakness by comparing how many times a patient can stand from a chair within 30-seconds with normative data based on age and gender, says Dr. Kenneth Miller, physical therapists and clinical educator at Catholic Home Care in Farmingdale, N.Y. Provide training, annual follow-up Quality managers should perform onsite visits with the therapists to watch how they conduct the functional testing, Miller says. They should also track individual therapists’ perfor- mance on the reassessment requirements on at least a quarterly basis, says Miller. Incorporating education, performance tracking and auditing have resulted in greater compliance rated and reduced risk of denials, he says. Many electronic medical records (EMR) systems have built in queries that quality or compliance staff can use to audit for cases that receive visits beyond the 13th and 19th reassessment in order to mitigate risk by improving compliance, Miller says. Those therapists who are having trouble with this requirement can then receive follow-up instruction. Conduct reassessments bi-monthly Don’t forget to include the basics of when to conduct therapy reassessments in your training. Reliable Healthcare Solutions in Morgantown, W. Va., has accomplished 100% compliance with the therapy reassessment regulations. That’s a big improvement from between 10 and 12 instances of noncompliance the agency had a few months ago, says Dale Derby, home health director who is also responsible for quality management at the agency. Therapists were failing to complete reassessments at the right time — on the 13th and 19th visit or every 30 days for single-therapy cases, says Derby. For
- 4. July 7, 2014 Home Health Line Exclusive web content and searchable CMS documents at www.homehealthline.com.4 multi-discipline cases, therapists have to complete reassessments on visits 11, 12 or 13 to meet the 13th visit requirement and on visits 17, 18 or 19 to meet the 19th visit requirement. Solution: The agency began tracking compliance and discussing the matter at weekly operations meetings, Derby says. He also began training clinicians in two-on-one sessions for a couple hours each session over a period of about a month on the Medicare regulations concerning therapy services, including information about whether the patient’s condition is still appropriate for therapy services over the course of a care episode, he says. He developed the training materials by distilling infor- mation from a variety of sources such as the Medicare administrative contractor, CGS Administrators, Medi- care’s Conditions of Participation and more, he says. Sections 40.2.1 (b) of Chapter 7 of the CMS Home Health Manual, for instance, is particularly helpful to understanding reassessment timing. Therapists should conduct reassessments every two weeks; this will ensure the therapist meets the Medicare requirement that a reassessment be completed at least every 30 days and gives the patient the best possible treatment, Miller recommends. — Nicholas Stern (nstern@decisionhealth.com) Editor’s note: The proposed 2015 PPS rule, released July 1, would change therapy reassessment timeframes. Therapy reassessments would occur every 14 calendar days rather than before the 14th and 20th visits and once every 30 calendar days. See upcoming issues of HHL for more details. ICD-10 delay Learn from the past, prepare for the future with revised timelines Now is the time to go back to your ICD-10 transi- tion team and do a post-mortem of all your preparation efforts to assess what your agency was able to accom- plish, what it has yet to achieve, where your training was effective and what areas you may have neglected. Since ICD-10 was delayed to Oct. 1, 2015, determin- ing the most effective approach to ongoing preparation efforts over the next year and a half will depend on your agency’s level of preparedness at the time of the delay, says Trish Twombly, senior director for DecisionHealth in Gaithersburg, Md. For example, those agencies that were diligently preparing and following recommended timelines that called for the dual coding of 10 charts a week by April 2014, should scale back their dual coding efforts, but Make it essential for staff to submit documentation in a timely fashion Agencies that have issues with timely documentation need to incorporate that requirement into their conditions of employment. Make sure your agency has a clear, written policy regarding expectations for clinicians to complete documentation and upload it to the EMR system. Failure to do so should result in disciplinary actions, advises Robert Markette of Hall, Render, Killian, Heath Lyman in Indianapolis. Likewise, warnings for violations of the policy should be handed out in written notices. This could help prove that the agency was not being subjective or picking on anyone for violating the policy should a clinician decide to file a complaint with the Equal Employment Opportunity Commission (EEOC). A third warning in such a policy, for example, could mean termination for the errant employee. Aside from the requirement that clinicians using an EMR turn their in documentation within 24 hours, Sutter Care at Home’s standard also requires all visit documentation except for the comprehensive start of care visit be completed or close to completion during the actual visit while in the home, says Sandy Sanville, director of clini- cal practice for Sutter Care at Home. Clinicians at Sutter Care at Home receive a yearly supervisory visit during which a manager observes them documenting in a patient’s home. Supervisors also monitor documentation timeliness on an ongoing basis through the EMR, Sanville says. This is also a focus during new clinician orientation. — Nicholas Stern (nstern@ decisionhealth.com)
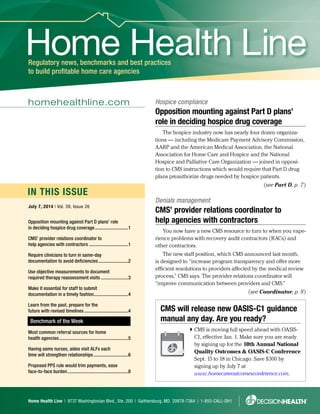
- 5. Home Health Line July 7, 2014 © 2014 DecisionHealth® | www.decisionhealth.com | 1-855-CALL-DH1 5 not stop them completely, Twombly says. Instead of dual coding 10 charts a week, now maybe just do two. It’s important to see that all the time, effort and money that’s been invested in ICD-10 to this point isn’t wasted, she says. The U.S. Department of Health and Human Services is expected to release an interim final rule “in the near future” enacting Oct. 1, 2015, as the new ICD-10 compliance date, and requiring all HIPAA covered entities to use the ICD-9 system through Sept. 30, 2015, CMS said its statement released May 1. Coders resolute to keep training More than 50% of home health agencies surveyed about the ICD-10 delay said while they could have been ready, they’re appreciative of more time to prepare. But 35% said they were prepared and are disappointed by the abrupt decision, according to the results of Decision- Health’s ICD-10 Delay Survey of 208 home health agencies. Despite the different feelings about the delay, every coder contacted by DecisionHealth expressed deter- mination to keep training and preparing, a position affirmed by coding experts. Assess gaps reset training timeline Reset your ICD-10 training timelines to one year from now, and if you haven’t been working from a timeline, now’s the time to get on one, says Ann Rambusch, presi- dent of Rambusch3 Consulting in Georgetown, Texas. A timeline developed for implementation this year called for establishing a transition team, budget and implementation plan by the end of the 2013 summer. Work from those benchmarks and begin retooling those things to be put into place over the next year, paying particular attention at this point to your budget and to critical gaps in your training processes, says Twombly. Quality and clinical managers who have already conducted documentation and/or coding audits to see whether clinicians are prepared for the increased level of detail required by ICD-10 should use the delay to do so again, this time with the benefit of their increased knowledge of ICD-10, says Twombly. Make a list of your agency’s top 10 diagnoses and make sure the clinical documentation is adequate for what will be required in ICD-10, she says. For example, make sure clinicians treating patients with diabetes with kidney failure document the stage of kidney failure, which is a requirement in ICD-10. Based on the results of clinician audits, quality manag- ers can focus training individual clinicians on such requirements as needed, Twombly says. Also, many agencies have overlooked the importance of training their intake staff in the increased documentation demands of ICD-10, Twombly says. However, it’s these people who are in a position to ensure that critical information about patients’ diagnoses, required to properly code in ICD-10, is received from referral sources up front, she says. To combat this training gap, make a list of the top 20 diagnoses that your agency treats, such as congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD), and then create tools that can be given to intake staff to help alert them to when they will need more specifics about a diagnosis, Twombly says. Currently, coders should focus on mastering or maintaining knowledge of ICD-10 fundamentals, like the Most common referral sources for home health agencies Below is the list of the most common home health referral sources. Note that nearly 20% of respondents to a recent HHL survey said that assisted living facilities were a top referral source. (See related story, p. 6.) The data include 50 home health agency responses to a recent HHL survey. 0% 10% 20% 30% 40% 50% 60% 70% 80% Physicians(general)Hospitals SkilledNursingFacilities Physicians(specialists) AcuteCareRehabilitation AssistedLivingFacilities(ALFs) WoundCareCenters InpatientRehabilitation PrviateDutyCompanies Other ACOsorOtherCare TransitionProjects Top referral sources Percentage of responents
- 6. July 7, 2014 Home Health Line Exclusive web content and searchable CMS documents at www.homehealthline.com.6 guidelines and conventions, with the aim of completing that by December. Intensive training should begin in January 2015 and continue through April, at which point dual coding should commence, says Judy Adams, presi- dent of Adams Home Care Consulting in Asheville, N.C. — Megan Gustafson (mgustafson@decisionhealth.com) Marketing referrals Having same nurses, aides visit ALFs each time will strengthen relationships Assign the same group of employees to visit assisted living facilities (ALFs) each time you have appoint- ments there. The assurance that the same people from your agency will visit each time will make patients and employees more comfortable about letting your agency into the facility, and could generate more referrals. Comfort Home Health in Daleville, Ind., assigns a physical therapist, occupational therapist, nurse and aide to a specific ALF. The familiarity the agency creates with ALFs — and the promises it keeps — helps it receive about 20% of its roughly 40 referrals a month through ALFs, says Kathy Eichelman, the agency’s community liaison. Strong relationships with ALFs will generate refer- rals, as many residents within the facilities have medi- cal issues that qualify them to become Medicare home health patients. ALFs are the sixth most common referral source in home health, according to HHL’s 2014 referrals survey. (See benchmark, p. 5.) About 18% of the survey’s 52 respondents listed ALFs among their agency’s top over- all referral sources. Show you can keep patients at home Your agency also can stand out to ALFs by showing that you can help with their bottom lines by keeping their occupancy rates high, industry experts say. Bring outcomes data to a meeting with the ALF, advises Katherine Northcutt, Marietta, Ga.-based senior manager at Simione Healthcare Consultants. Display your rehospitalization rates overall and by disease category, and show how they compare with other area agencies (HHL 6/30/14). When first speaking with an ALF’s employees, ask about the facility’s process for referring a patient to home health. If its social services director serves in that role, she would be the person to speak with about devel- oping a relationship, Northcutt says. Your goal from the initial conversation should be to determine the ALF’s needs and address how your agency can lessen problems, Northcutt recommends. Among the questions to ask: What are the biggest challenges with keeping residents? How is the ALF able to meet residents’ needs when they return from a hospital stay? How often are people hospitalized? Are there a lot of fall issues? After an initial conversation, provide the facility with the data that shows your agency can help best, Northcutt says. Offer educational sessions in ALFs Spending time inside an ALF and offering free, 10-minute monthly wellness presentations to residents also could potentially be a good way to generate refer- rals, adds Lori Moshier, president of Novi, Mich.-based Novaetus, a marketing firm. Presentation topics could include elder abuse, how to avoid falls in your home and heart-healthy diets for seniors. Since you’re not offering anything of value — much of the information you’d provide is available free online — there would not be a kickback concern, says home health attorney Robert Markette of Hall, Render, Killian, Heath Lyman in Indianapolis. But agencies performing presentations for residents should not spend more than $10 per person each time on food, Markette advises. And agencies should not spend more than $50 per person on food over the course of a year. Sell your agency’s benefits to ALFs •• Explain that you want to work with them, not against them. Educate ALFs about how your agency is trying to help their residents stay healthy and at home, says Jessica Vaughn, marketing and admissions director for At Home Assisted Living Services, an Anderson, Ind.- based private duty agency. In the past 18 months, 16 to 18% of the agency’s refer- rals have come from ALFs. The agency receives about 200 referrals a year. •• Highlight things you can do that the ALF can’t. At Home Assisted Living Services has some clients living within ALFs who simply need someone to spend the night and ensure they’re safe, Vaughn says. An ALF employee wouldn’t be able to spend all night with a resident, she says.
- 7. Home Health Line July 7, 2014 © 2014 DecisionHealth® | www.decisionhealth.com | 1-855-CALL-DH1 7 Please pass this coupon to a colleague who could benefit from a subscription to Home Health Line. Payment enclosed. Make checks payable to Home Health Line; (TIN: 26-3622553) Send me an invoice (PO __________________) Charge my: Card #: _________________________________________________ Exp.Date: ________________________________________________ Signature: _______________________________________________ Mail to: Home Health Line Two Washingtonian Center, 9737 Washingtonian Blvd., Ste. 200, Gaithersburg, MD 20878-7364 | 1-855-CALL-DH1 YES! I want the latest business and regulatory news, benchmarks, best practices and executive tools to increase my profitability and ensure agency growth. Please enter my one year (48 issues) subscription at $597 for Home Health Line. Name: __________________________________________________ Org: ____________________________________________________ Address: ________________________________________________ City/State/ZIP: ____________________________________________ Phone: __________________________________________________ Fax: ____________________________________________________ Email: __________________________________________________ www.homehealthline.com PAS 2014 •• Tell them you’ll respect their protocols and make them feel comfortable. Say that your employees will sign in at the ALF’s front desk and park in appropri- ate parking spaces, Moshier says. Also, if possible discuss your consistency in sending the same group of caregivers to the ALF for visits. “That goes a long way with those types of professionals, because they want to know who’s coming in and out of their building,” Vaughn says. — Josh Poltilove (jpoltilove@decisionhealth.com) Part D (continued from p. 1) In a letter to CMS last week, the organizations have urged CMS to withdraw its instructions “until a workable alternative is developed that does not place the burden of resolving payment disputes squarely on the shoulders of terminally ill Medicare beneficiaries.” The guidance in question — which took effect May 1 — states that hospices must provide “a coherent clinical explanation” to the patient’s Part D plan about why the drug is medically necessary but unrelated to a patient’s terminal condition and therefore not a cost the hospice needs to cover (HHL 5/12/14). Without such an explana- tion, the plan need not pay. Plan decisions against drug coverage have faced VNA of Hudson Valley’s hospice unit with hard choices. Recent examples cited by Rose Rosenberg, the Tarry- town, N.Y., agency’s VP for hospice, include two terminal cancer patients in need of an anticoagulant for their deep vein thrombosis. The patients’ Part D plan wouldn’t pay the twice-daily cost of $180. Those patients, both homebound, were able to choose palliative care as home health patients as an alternative to hospice. But, more and more the hospice unit finds itself, for compassionate reasons, absorbing the cost of secondary diagnosis drugs needed by non- homebound patients who can’t afford to foot the bill themselves, Rosenberg relates. Authorization stems from OIG report The issue of coordinating payments for drugs required by hospice patients grew out of an HHS Office of Inspector General study that found that Medicare had to spend $400 million in 2012 for drugs used by hospice patients but not covered by the hospice program. CMS has indicated that it ultimately would turn over to an independent reviewer the task of deciding whether disputed drug costs belong to the hospice or to the patient’s drug plan. But that process won’t be available in 2014 and first must be established through regulation, presumably in the final 2015 hospice rule. Meantime, the potential harshness of CMS’ current directions is evident in letters many hospices have received from a debt collection agency acting in behalf of Part D carrier United Healthcare Insurance. Sent by debt collector Payment Resolution Services of Nashville, Tenn., the letters seek reimbursement for pain-relieving analgesics billed in 2011 and 2012, which
- 8. July 7, 2014 Home Health Line Exclusive web content and searchable CMS documents at www.homehealthline.com.8 according to the collection company actually were costs the hospices were responsible for. In one case known to HHL, the Payment Resolution Services is seeking $1,000; in the second, the amount demanded is about $20,000, which the hospices in ques- tions have 30 days to pay, the letters state. Hospices are being told they have 30 days from the receipt of the letter to dispute the debt. CMS advised Part D drug plan sponsors last October of their obligation to recoup the payments in question (HHL 6/16/14). — Burt Schorr (burt.schorr@verizon.net) Coordinator (continued from p. 1) The coordinator will listen to overall process concerns and suggestions, though agencies still should direct questions about specific claims to RACs and Medicare Administrative Contractors (MACs), CMS says. Latesha Walker, the new CMS coordinator, has previously served as a program relations manager and senior advisor with CMS. She is helpful, and if she doesn’t know answers to questions, she finds people who do, says consultant Wayne van Halem, president of Atlanta-based van Halem Group. Van Halem has worked with Walker in recent weeks when dealing with issues involving StrategicHealthSolutions, a Supplemental Medical Review Contractor (SMRC) that he believed was neither cooperative nor communicative. But it’s unclear how effective this position will be. Given the volume of work RACs and MACs perform, Walker likely will be “hammered” with calls and emails in the new position, argues attorney Robert Markette of Hall, Render, Killian, Heath Lyman in Indianapolis. RAC pause continues for agencies Walker’s position will be even busier after RACs begin issuing additional documentation requests (ADRs) again in the coming months. On Feb. 18, CMS announced that it told RACs to stop issuing ADRs until it awards the next round of contracts (HHL 3/3/14). It appears contracts will be awarded this summer, followed by post-award protests that will further delay the start date for the new RACs, says Emily Evans, a partner and legislative/regulatory analyst for Nashville- based Obsidian Research Group. In the meantime, CGI Federal Inc. elevated its pre- award bid protest over re-procurement of the RAC contracts to the Court of Federal Claims last month. CGI is currently the RAC for Region B, which includes Ohio, Michigan and five other states. The lawsuit seeks an injunction against the award of the new RAC contracts. It also asks the federal court to eliminate new payment terms prohibiting RACs from being compensated until after the second level of appeal — a payment delay preventing RACs from being paid for about a year, Evans says. The lawsuit is likely among the reasons CMS is delaying the contracts for all RAC regions, including the region that will handle claims nationwide for more than 12,000 home health agencies, as well as hospices and DME companies, she says. When to contact the CMS coordinator •• Notify the contractor of lack of timely review results. Delays on notice letters from RACs create problems for some agencies, Markette says. RACs communicate to MACs electronically, but send the notice to the provider by regular mail. •• Point out cases where the contactors’ interpretation of the law is questionable. Situations arise where contractors view certain records with basically the same wording and approve some while denying others, says Arlene Maxim, owner of A.D. Maxim Consulting in Troy, Mich. — Josh Poltilove (jpoltilove@decisionhealth.com) Related links: Contact Latesha Walker by emailing RAC issues to RAC@cms.hhs.gov or emailing MAC issues to MedicareMedicalReview@cms.hhs.gov. Breaking news: Proposed PPS rule would trim payments, ease face-to-face burden Your Medicare payments would drop by a fraction, but you’d gain considerable face-to-face relief under the proposed 2015 PPS rule. CMS proposes to eliminate the controversial requirement that certifying physicians provide a narrative in their own words explaining why the patient is eligible for home health. For continued, in-depth analysis of how this rule affects your agency, go to www. homehealthline.com. To view the complete rule, link to: http://homehealthline.decisionhealth.com/ Articles/Detail.aspx?id=518249.
- 9. Home Health Line July 7, 2014 © 2014 DecisionHealth® | www.decisionhealth.com | 1-855-CALL-DH1 9 How did you get this email? It is illegal to forward Home Health Line Online to anyone else. It is a free benefit only for the individual listed by name as the subscriber. It’s illegal to distribute Home Health Line Online to others in your office or other sites affiliated with your organization. If this email has been forwarded to you and you’re not the named subscriber, that is a violation of federal copyright law. However, only the party who forwards a copyrighted email is at risk, not you. Reward: To confidentially report suspected copyright violations, call our copyright attorney Steve McVearry at 1-301-287-2266 or email him at smcvearry@ucg.com. Copyright violations will be prosecuted. And Home Health Line shares 10% of the net proceeds of settlements or jury awards with individuals who provide essential evidence of illegal electronic forwarding of Home Health Line Online or photocopying of our newsletter.
- 10. Home Health MARKETPLACE Guide | July 7, 2014 1 Home Health MARKETPLACE Guide In this supplement 5 tips to speed physician communication, reduce emergency room visits............................................................... 1 Have an idea for a story or a comment on an article in this supplement? Contact Elizabeth Christian at 1-800-929-4824 x2232 or by email at echristian@decisionhealth.com.FOR HOME HEALTH CARE PROFESSIONALS HOME HEALTH MarketplaceGUIDE A supplement to 5 tips to speed physician communication, reduce emergency room visits Use advance orders and other preventive strategies to make sure you’re able to reach physicians in the event of an emergency. Having a plan in place may allow you to avoid survey citations and unnecessary emergency room visits. In acute situations, waiting around for a physician to call you back could land your agency in trouble. A surveyor won’t care that the physician didn’t get back to you when a patient comes to harm, says Ann Rambusch, Georgetown, Texas-based clinical consultant. Your agency is responsible for its patients, so the surveyor will want to see that you have a solid plan in place when a physician response is late or doesn’t come at all. Multiple level 1 survey standards address the need to communicate with the physician when a patient’s condition changes. For example, G165 requires that agency staff administer drugs or other treatments only as ordered by a physician. That puts you at a potential disadvantage as hospitals begin to look for home health agencies that can help them avoid readmission penalties starting this fall. A.C.T. Health Care Services was recently forced to send a patient to the emergency room because it couldn’t get in contact with the supervising physician. The patient’s blood pressure was close to inducing a stroke, even though the patient had taken her blood pressure medicine, says Tamara Salyer, administrator at the Worthington, Ohio-based agency. When the agency attempted to contact the physician, it never got a return phone call. “We could have prevented an emergency room visit had the physician called and offered additional dosage(s) of her blood pressure medication or called in a prescription,” Salyer says. Encourage physician communication Employ these strategies to improve physician communication and response time in the event of a patient emergency: • Send physicians a list of vital sign parameters that would prompt a call. The list explicitly outlines when you will contact the physician, such as when the patient’s pulse falls below 90BPM when at rest. You can include the list of parameters on the plan of care as well. Make sure the parameters are specific and outline scenarios that are likely to come up based on the patient’s condition and history, Rambusch says. • Offer the physician a solution for the emergency. If your patient is teetering on the edge of an emergency, call the physician with a recommendation. This makes it easier for physicians to act quickly because all they have to do is give you a yes or no response, rather than finding a solution on their own, Rambusch says. Physicians would much rather deal with an assertive nurse than an unsure one, she says. • Ask for the back office number. The benefit of this is that physicians are much more likely to answer that line than the main line, Rambusch says. The main line gets more traffic, and on Friday at 4:30, the office staff may not answer, she says. • Keep all communications as short as possible. Call the physician and say the patient’s blood pressure is 140/90, and you need orders to prevent a visit to the emergency room, Rambusch says. • Use your medical director to establish contact in emergencies. Sometimes physicians are more inclined to speak with another physician, Rambusch says. Most agencies don’t use medical directors as a liaison between the physician and the agency, even when they have them, says Arlene Maxim, founder of A.D. Maxim Associates in Troy, Mich. — Danielle Cralle (dcralle@decisionhealth.com) The information in this article was current as of the date it was printed on July 2, 2012.
- 11. 2 July 7, 2014 | Home Health MARKETPLACE Guide Home Health MARKETPLACE Guide Boost referrals, increase profitability and navigate regulations certain to change the way you do business The days of non-medical home care flying under the regulatory radar are over. Health care reform will bring both challenges and opportunities for your business. Join hundreds of private duty executives at the conference and hear real-world success stories from top performing agencies to grow and thrive in the non-medical home care market. Register today and walk away with strategies and tools to: Become a care-transition partner, differentiate with dementia care and drive referrals Motivate and mentor a solid sales force Stay ahead of the competition with innovative customer service strategies and technology trends Turn your website into a marketing magnet Lessen the impact of new legal, human resource and wage-and-hour rules Master recruitment and retention with data-driven strategies Register at www.privatedutyconference.com or call toll-free 1-855-CALL-DH1 today! PRESENTED BY: 17TH ANNUAL PRIVATE DUTYNATIONAL CONFERENCE EXPO Encore, Las Vegas, NV | November 19–21, 2014 Download your materials ahead of time Visit the “Materials” tab on the website for details! Sign-up for Private Duty Insider’s free bi-monthly ezine! To start receiving this free ezine, go to www.decisionhealth.com/pdezine today. “Great Event! There were one or two sessions alone that were valuable enough to cover the cost of the conference. And, networking with other owners and industry leaders during and between sessions was as valuable as any presentation.” DEREK JONES, Director of marketing, Griswold Home Care, Erdenheim, Pa. Receive ready-to-use tools worth thousands of dollars!