
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Tef ppt copy
Similaire à Tef ppt copy (20)
Plus de Nidhi Chauhan
Plus de Nidhi Chauhan (18)
Dernier
Dernier (20)
Tef ppt copy
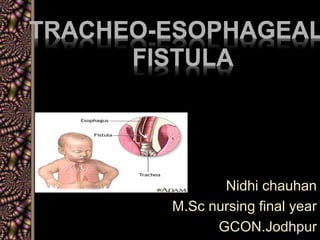
- 1. TRACHEO-ESOPHAGEAL FISTULA Nidhi chauhan M.Sc nursing final year GCON.Jodhpur
- 2. Introduction Tracheo esophageal fistula occurs in one of 3000 to 5000 births. Before the performance of the first successful repair in 1939, this condition was fatal over the post 50 years. Estimates today suggest that in the absence of other severe anomalies, survival rate in these infants approach 100%.
- 3. DEFINITION Tracheo esophageal fistula is an abnormal connection between trachea and oesophagus .These disorder commonly found among premature and low birth weight neonate and mother’s having polyhydramnias
- 5. RISK FACTORS OF TEF- The exact cause of these anomalies is not known in most cases. But these anomalies develop due to deviation of septum between the oesophagus and trachea or altered growth of septum between them. It mostly occurs during fourth and fifth week of gestational life.
- 6. • Heritable genetic factor • Intrauterine environment • Teratogenic stimuli
- 7. CLASSIFICATION Type I - EA without fistula (8%). There is no connection of esophagus to trachea. The upper (proximal) segment and lower (distal) segment of esophagus are blind.
- 9. Type II - EA with TEF (upper). It is rare and found in less than 1%of all cases. Upper segment of esophagus open into trachea by a fistula. The distal or lower segment is blind. Type III -EA with Fistula (80-90%). It is the most common type. In this condition, proximal and upper segment of the esophagus has blind end. The distal lower segment of esophagus connects into trachea by a fistula.
- 10. Type IV –EA with TEF both upper and lower segment. It is also rare, less than 1%. There is with fistula between both proximal and distal ends of trachea and esophagus. Type V-H shape type of TEF. It is found in about 4% of all cases and not usually diagnosed at birth. Both proximal /upper and distal/lower segments of esophagus open into trachea by a fistula. No EA present
- 12. PATHOPHYSIOLOGY
- 13. • Respiratory distress may develop due to gastric distension and elevation of diaphragm.
- 14. CLINICAL MANIFESTATION OF TEF- The clinical feature appears soon after birth. The baby presents with excessive salivation, constant drooling, large amount of secretions form nose, and also shown 3 “C” signs . coughing, chocking and cyanosis, gagging.
- 16. Intermittent unexplained cyanosis occurs due to laryngospasm caused by aspiration of accumulated saliva in blind pouch. On the very first feed, after first and second swallow, the infant coughs, chokes or fluid returns out through nose and mouth. The infant struggle for breath and cyanosis occurs. Only abdominal distension and poor feeding may found in some infants.
- 17. SOME OTHER ANOMALIES PRESENT IN CLIENT WITH TEF. LIKE - VACTERL V- vertebral anomalies A- anal atresia C- cardiac malformation T- tracheo esophageal fistula R- renal anomalies L- limb anomalies and hydrocephalus.
- 18. DIAGNOSIS OF TEF- Clinical presentations arouse a strong suspicious. Simple technique can be done to diagnosis the condition with plain catheter. Inability to pass catheter through nose or mouth into the stomach indicate blind pouch or atresia.
- 20. Antenatal diagnosis of the condition can be done by USG. Postnatal diagnostic procedures include USG, plain X-ray of abdomen, chest X- ray or passing of radio-opaque catheter through esophagus and confirming the anomalies by X-ray. Bronchoscopy also help to confirm the diagnosis. ECG can be done to detect associated cardiac anomalies
- 21. MANAGEMENT OF TEF- a. Immediate management – Immediately after diagnosis, the infant should be managed with propped up position(30 angle) to prevent reflux of gastric secretion, and nothing per mouth, oxygen therapy, I/V fluid therapy.
- 23. b. Nasogastric tube aspiration- Nasogastric tube to be kept in situ and suctioning to be done frequently to prevent aspiration. c. The blind pouch to be washed with normal saline to prevent blocking of tube with thick mucus. d. Gastrostomy is done to decompress the stomach and to prevent aspiration and afterwards to feed the infant
- 25. e. Supportive care should include maintenance of nutritional requirement and warmth, prevention of infection, antibiotic therapy, respiratory support, detection and treatment of complications, continuous monitoring of patient condition, chest physiotherapy and postural drainage.
- 26. SURGICAL MANAGEMENT The surgical correction of defect is done by end to end anastomosis with excision of the fistula by right posterolateral thoracotomy followed by intercostals chest drainage. This is done when the infant has more than 2kg body weight and no pneumonia present and the baby is clinically stable.
- 27. Surgical correction can be done in stages with division of fistula. Gastrostomy is performed in initial stage followed by esophageal or colonic transplant after 1year. Other surgical intervention includes Cervical esophagostomy, esophago- coloplasty and esophago-gastroplasty
- 28. NURSING MANAGEMENT – • Nursing management is very important to detect the condition immediate after birth or at first feed. • Clinical features and problems to be assessed promptly for lifesaving measures.
- 29. The important nursing diagnosis is include – I. Preoperative- • Risk for aspiration related to esophageal abnormality. • Risk for fluid volume deficit related to inadequate oral intake. • Parental anxiety related to congenital anomalies of the neonate.
- 30. II. Postoperative – • Ineffective airway clearance related to surgical interventions. • Altered nutrition, less than body requirement related to inadequate oral intake. • Pain related to surgical intervention. • Risk for infection related to hospital procedures. • Knowledge deficit related to home based long term care.
- 31. NURSING INTERVENTION- Nursing intervention are performed based on nursing diagnosis. Preoperative intervention- • Preventing aspiration by positioning, suctioning and nothing by mouth, thus reducing chance of respiratory infections.
- 32. • Preventing dehydration by I/V fluid, intake and output recording, monitoring of vital signs and child’s general health. • Preventing infections by infection control measures. • Reducing parental anxiety by emotional support.
- 33. Postoperative intervention- • Maintaining clear airway • Providing adequate feeding by I/V fluid and gastrostomy feeding. • Reducing pain by analgesics and comfort measures. • Maintaining chest tube drainage with necessary precautions.
- 34. • Preventing infection by general cleanliness, hygienic measures and administrating antibiotics. • Improving knowledge by necessary health education, encourage questions and explaining the answers.
- 35. SUMMARY Esophageal atresia is a failure of the esophagus to form a continue passage from the pharynx to the stomach during embryonic development. These anomalies develop due to deviation of septum between the oesophagus and trachea or altered growth of septum between them. It mostly occurs during fourth and fifth week of gestational life.
- 36. • Simple technique can be done to diagnosis the condition with plain catheter. • Postnatal diagnostic procedures include USG, plain X-ray abdomen, chest X-ray or passing of radio-opaque catheter through esophagus and confirming the anomalies by X-ray. Bronchoscopy also help to confirm the diagnosis.
- 37. • Immediately after diagnosis, the infant should be managed with propped up position(30 angle) to prevent reflux of gastric secretion, and nothing per mouth, oxygen therapy, I/V fluid therapy. • Nasogastric tube aspiration nasogastric tube to be kept in situ and suctioning to be done frequently to prevent aspiration. • The blind pouch to be washed with normal saline to prevent blocking of tube with thick mucus
- 38. conclusion • Most neonate who undergo repair of TEF have some degree of esophageal dysmotility. The extent of the repair dictates the severity of subsequent complication strictures at the site of the anastomosis are common and may subsequently require dilation. • Serial esophagraphy should be performed at two months, six months and one year of age or whenever swallowing difficulties occur