
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Kernicterus
Similar to Kernicterus (20)
More from Raafi Ul Zargar
Recently uploaded
Recently uploaded (20)
Kernicterus
- 1. PEDIATRICS RAAFI UL BASHEER ZARGAR
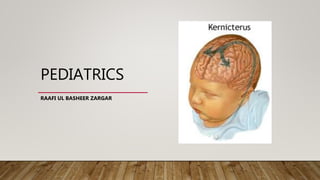
- 2. KERNICTERUS • Kernicterus, or bilirubin encephalopathy, is a neurologic syndrome resulting from the deposition of unconjugated (indirect) bilirubin in the basal ganglia and brainstem nuclei.
- 3. RISK FACTORS • Jaundice within first 24 hrs of birth • A sibling who was jaundiced as neonate • Unrecognised hemolysis (ABO- or Rh- incompatibility) • Non optimal sucking nursing • Deficiency of G6PD • Infection • Cephalhematomas bruising • East Asian or Mediterranean descent
- 4. PREVENTABLE CAUSES OF KERNICTERUS • The American Academy of Pediatrics has identified potentially preventable causes of kernicterus, as follows: (1) early discharge (<48 hr) with no early follow-up (within 48 hr of discharge); this problem is particularly important in near-term infants (35-37 wk of gestation); (2) failure to check the bilirubin level in an infant noted to be jaundiced in the 1st 24 hr; (3) failure to recognize the presence of risk factors for hyperbilirubinemia; (4) underestimation of the severity of jaundice by clinical (visual) assessment; (5) lack of concern regarding the presence of jaundice; (6) delay in measuring the serum bilirubin level despite marked jaundice or delay in initiating phototherapy in the presence of elevated bilirubin levels; and (7) failure to respond to parental concern regarding jaundice, poor feeding, or lethargy.
- 5. PATHOGENESIS • MULTIFACTORIAL 1. Unconjugated bilirubin levels, 2. Albumin binding and unbound bilirubin levels, 3. Passage across the blood-brain barrier, and 4. Neuronal susceptibility to injury.
- 6. ETIOPATHOGENESIS • The precise blood level above which indirect-reacting bilirubin or free bilirubin will be toxic for an individual infant is unpredictable, but in a large series, kernicterus occurred only in infants with a bilirubin >20 mg/dL. • Ninety percent of the infants in whom kernicterus developed were in previously healthy, predominantly breastfed term and near-term infants. • The duration of exposure to high bilirubin levels needed to produce toxic effects are unknown. • The more immature the infant is, the greater the susceptibility to kernicterus.
- 7. CLINICAL FEATURES • INITIAL SIGNS • LETHARGY • POOR FEEDING • LOSS OF MORO REFLEX • LATER SIGNS • INFANT APPEARS GRAVELY ILL • PROSTRATIONS • DIMINISHED TENDON REFLEXES • RESPIRATORY DISTRESS • OPISTHOTONOS WITH BULDGING FONTANELLE • TWITCHING OF FACE OR LIMBS • SHRILL HIGH PITCHED CRY
- 8. CLINICAL FEATURES • ADVANCED STAGE • CONVULSIONS AND SPASM OCCUR • AFFECTED INFANTS STIFFLY EXTENDING THEIR ARMS IN AN INWARD ROTATION WITH THE FISTS CLENCHED. • RIGIDITY IS RARE AT THIS LATE STAGE.
- 10. RECOVERY • Many infants who progress to these severe neurologic signs die; the survivors are usually seriously damaged but may appear to recover and for 2-3 months show few abnormalities. • Later in the 1st yr, opisthotonos, muscle rigidity, irregular movements, and convulsions tend to recur. • In the 2nd yr, the opisthotonos and seizures abate, but irregular, involuntary movements, muscle rigidity, or, in some infants, hypotonia increase steadily. • By 3 yr of age, the complete neurologic syndrome is often apparent; it consists of bilateral choreoathetosis with involuntary muscle spasms, extrapyramidal signs, seizures, mental deficiency, dysarthric speech, high-frequency hearing loss, squinting, and defective upward eye movements. • Pyramidal signs, hypotonia, and ataxia occur in a few infants. In mildly affected infants, the syndrome may be characterized only by mild to moderate neuromuscular incoordination, partial deafness, or “minimal brain dysfunction,” occurring singly or in combination; these problems may be unapparent until the child enters school.
- 11. INCIDENCE AND PROGNOSIS By pathologic criteria, kernicterus develops in 30% of infants (all gestational ages) with untreated hemolytic disease and bilirubin levels >25-30 mg/dL. The incidence at autopsy in hyperbilirubinemic preterm infants is 2-16% Overt neurologic signs have a grave prognosis; more than 75% of infants die, and 80% of affected survivors have bilateral choreoathetosis with involuntary muscle spasms. Mental retardation, deafness, and spastic quadriplegia are common.
- 12. PREVENTION • Universal screening for hyperbilirubinemia in the 1st 24-48 hr after birth to detect infants at high risk for severe jaundice and bilirubin induced neurologic dysfunction. • Protocols • Hour-specific bilirubin nomogram • Physical examination, and • Clinical risk factors
- 13. MANAGEMENT • The following approach is further recommended: (1) any infant who is jaundiced before 24 hr requires measurement of total and direct serum bilirubin levels and, if it is elevated, evaluation for possible hemolytic disease and (2) follow-up should be provided within 2-3 days of discharge to all neonates discharged earlier than 48 hr after birth. • Early follow-up is particularly important for infants younger than 38 wk of gestation. • Parental communication with regard to concerns about infant’s skin color and behavioral activities should be addressed early. • Mothers should be advised to nurse their infants every 2-3 hr and to avoid routine supplementation with water or glucose water in order to ensure adequate hydration and caloric intake.
- 14. REFERENCES I. NELSON TEXTBOOK OF PEDIATRICS, 20TH EDITION
- 15. THANK YOU