More Related Content
Similar to 2016_11_2_066-072
Similar to 2016_11_2_066-072 (20)
2016_11_2_066-072
- 1. CANCER & CHEMOTHERAPY Rev. 2016;11CANCER&CHEMOTHERAPYREVIEWS
66
Correspondence to:
Beatriz Pérez-Villamil
Laboratorio de Genómica y Microarrays
Laboratorio de Oncología Molecular
Servicio de Oncología Médica
Instituto de Investigación Sanitaria San Carlos (IdISSC)
Hospital Universitario Clínico San Carlos
Paseo Profesor Martín Lagos, s/n
28040 Madrid, Spain
E-mail: beatriz.perezvillamil@salud.madrid.org
New Molecular Classification
of Colorectal Cancer
Mateo Paz-Cabezas, Tania Calvo-López and Beatriz Pérez-Villamil
Laboratory for Genomics and Microarrays, Laboratory for Molecular Oncology, Department of Medical Oncology, Instituto de Investigación Sanitaria
San Carlos (IdISSC), Hospital Clínico San Carlos, Madrid, Spain
ABSTRACT
Colorectal cancer is a heterogeneous disease and traditional histological
classification in stages is not enough to accurately predict the course of the pathology
or the response to therapy. Many attempts to complement this classification with
molecular markers have been carried out in order to improve accuracy. First markers
considered were the presence of microsatellite or chromosomal instability, DNA
methylation, or mutations in relevant genes such as KRAS or BRAF and subgroups
were described with different combinations of these biomarkers. However, these
classifications are not used in clinical practice since significant overlapping among
subtypes is present.
The emergence of genomic methodologies has considerably improved the search for
prognostic biomarkers, the identification of driver mutations, or relevant pathways
implicated in tumor progression. Particularly, transcriptomics constitutes an excellent
tool for tumor classification and the discovery of relevant genes and pathways.
Using microarray gene expression, a robust classification in four Consensus Molecular
Subtypes has been reported that is the basis for future clinical intervention in
colorectal cancer. (Cancer & Chemotherapy Rev. 2016;11:66-72)
Corresponding author: Beatriz Pérez-Villamil, beatriz.perezvillamil@salud.madrid.org
KEY WORDS
Colorectal cancer. Molecular classification. Microarray analysis. Transcriptomics.
Gene mutation. Tumor heterogeneity.
PERMANYER
www.permanyer.com
www.cancerchemotherapyreviews.com Cancer & Chemotherapy Rev. 2016;11:66-72
Nopartofthispublicationmaybereproducedorphotocopyingwithoutthepriorwrittenpermissionofthepublisher. ©PermanyerPublications2016
- 2. Mateo Paz-Cabezas, et al.: CRC Molecular Classification
CANCERCHEMOTHERAPYREVIEWS
67
Introduction
Colorectal cancer (CRC) is a major health prob-
lem and is the third leading cause of cancer deaths
in developed countries1
. Traditionally, it is classified
according to clinical and morphological character-
istics such as depth of tumor invasion into the intes-
tinal wall (T), number of affected lymph nodes (N),
or the presence of distant metastases (M); these
parameters constitute the basis for the TNM clas-
sification in stages I to IV2
.
Surgery is curative in localized disease (stages I,
II, III), with 85-95% overall survival at five years for
stage I, 60-80% for stage II, 30-60% for stage III,
and roughly 10% for stage IV3
. To increase overall
survival, adjuvant chemotherapy after surgery is
administered in stage III and in high-risk stage II
cases4
. Almost all patients with advanced disease
(stage IV; distant metastases) require chemothera-
py to increase survival. Approximately 35% of pa-
tients have metastatic disease at diagnosis and
20-50% of stage II-III patients develop metastases
in the course of the disease, with the liver being
the most common site of metastatic spread. There
is a small subset of patients with metastatic dis-
ease isolated in the liver or lungs that can be of-
fered potentially curative surgical treatment. He-
patic resection has become the treatment of choice
for patients with hepatic metastases only, and neo-
adjuvant chemotherapy currently has a major role
in this setting as it increases the success of resec-
tion5
. The prognosis for patients with metastatic dis-
ease is generally poor, and only a small portion of
these patients shows an objective response to che-
motherapy.
This high variability in part is caused because CRC
is not a single disease; it is a heterogeneous complex
of diseases. Each patient has unique features caused
by distinctive genetic background and following
events that lead the tumor development. Even within
the same tumor, continuous clonal selection makes
the tumor a non-homogenous environment, suffer-
ing constant evolutionary pressure6. Within this het-
erogeneity, not only the cell must be considered, but
also the tumor microenvironment and its interactions
with tumor cells can determinate the molecular pro-
file, evolution, and clinical behavior of the carcinoma
in a strong way. These are the main reasons why
histological grades are not enough to explain colon
cancer phenotypic diversity, clinical behavior, or re-
sponse to therapies.
Despite important improvements in the tradition-
al TNM system of classification7
, new strategies are
needed to obtain a better stratification of patients
with CRC. The identification of novel prognostic
and predictive markers is required in order to com-
plement this traditional CRC classification for a bet-
ter management of the patients with CRC.
Classification Based
on Microsatellite Instability
and DNA Methylation
Molecular features, such as chromosomal frac-
tures, microsatellite instability, or DNA methylation,
have been considered for the classification of CRC
and three main groups have been described: (i) chro-
mosomal instable (CIN) tumors with big chunks of
DNA deleted, amplified, or translocated; (ii) microsat-
ellite instable (MSI) tumors with deficient mismatch
repair mechanisms; (iii) CpG island methylator phe-
notype (CIMP) tumors with higher levels of methyl-
ated DNA. Combinations of these main groups with
mutations in KRAS and BRAF were used as a first
attempt at CRC classification8 as they are well-known
features, playing an important role in the molecular
basis and development of the disease.
Genetic instability has been shown to be an im-
portant mechanism implicated in cancer develop-
ment and has been used to classify CRC. One class
Key issues
– Cancer is a complex and highly heterogeneous disease. Traditional histopathological classification
of colorectal cancer in stages is not enough to precisely anticipate clinical outcome or response
to therapy.
− Biomarkers such as the presence of microsatellite instability, DNA methylation or mutations in
relevant genes such as KRAS or BRAF and different combinations of them have been used to
classify colorectal cancer, although significant overlapping occurs, and consequently, this clas-
sification is not used in clinical practice.
− The potential of combined information from various “-omics” technologies to define disease states
and assist understanding of biological processes has motivated translational research for new
biomarkers and novel and robust classifications have been reported.
Nopartofthispublicationmaybereproducedorphotocopyingwithoutthepriorwrittenpermissionofthepublisher. ©PermanyerPublications2016
- 3. CANCER CHEMOTHERAPY Rev. 2016;11CANCERCHEMOTHERAPYREVIEWS
68
of genetic instability is composed by tumors with an
impaired DNA mismatch repair mechanism, causing
the formation of novel microsatellites fragments. The
CRCs with microsatellite instability (MSI) are catego-
rized in MSI-high (MSI-H), MSI-low (MSI-L), and MS
stable (MSS). Tumors with MSI-H represent approx-
imately 15% of all CRC. A second class is tumors with
aneuploidies and losses or gains of chromosomes
fragments. Tumors with chromosomal instability (CIN)
are MSS or MSS-L and represent the main propor-
tion, about 70%, of all CRCs. A subset of CRCs
(about 15%) is negative for both MSI-H and CIN.
Cytosines in CpG dinucleotides can be methyl-
ated; when these CpG islands are located in the
promoter region of the gene, the inhibition of its
expression is induced. The malfunction of this epi-
genetic mechanism (tightly controlled in every nor-
mal cell) plays an important role in tumor develop-
ment, being able to silence tumor suppressing genes
or releasing the repression over oncogenes expres-
sion9. The CpG island methylator phenotype (CIMP),
tumors with CIMP-H, represents approximately 20%
of all CRC and a fraction of them are negative for
both CIN and MSI-H.
Colorectal cancer has been stratified in five sub-
types using different combinations of these main
mechanisms and the presence of mutations in KRAS
and BRAF (V600E) that are mutually exclusive8.
– Type 1 (CIMP-H ⁄ MSI-H ⁄ BRAF mutation)
known as sporadic MSI
– Type 2 (CIMP-H ⁄ MSI-L or MSS ⁄ BRAF mu-
tation)
– Type 3 (CIN; CIMP-L ⁄ MSS or MSI-L ⁄ KRAS
mutation)
– Type 4 (CIN; CIMP-negative ⁄ MSS)
– Type 5 (CIMP-negative ⁄ MSI-H) known as fa-
milial MSI.
Type 4 has the highest proportion of tumors, ac-
counting for 57% of all CRC. The next most repre-
sented is type 3 with more than 20% of patients. The
proportion of patients in types 1, 2, and 5 ranges
between 12, 8, and 3%, respectively. These subtypes
are not pure; there is certain amount of overlap
between them. In this way, types 2, 3, and 5 com-
bine the molecular features of types 1 and 4 in
different ways (Fig. 1).
Serrated is one of the histological variants of
colorectal carcinomas, representing approximately
15% of all CRC. The serrated pathway is an alterna-
tive way of carcinogenesis with respect to the tradi-
tional pathway of colorectal carcinogenesis with the
aberrant activation of the APC/β-catenin pathway,
RAS, and p53 mutations. Serrated polyps are the
precursors of types 1 and 2 and a fraction of type 3
tumors, including all CIMP-H tumors with mutation
in BRAF, sporadic MSI-H, and some CIMP-L with
KRAS mutation.
Similar classifications have been reported using the
same parameters, taking into account those that are
mutually exclusive, mismatch repair proficient (MSS),
or deficient (MSI) and mutations in KRAS or BRAF
in order to reduce, as much as possible, subtypes
overlapping. Three types are mismatch repair pro-
ficient (MSS): MSS with mutations in BRAF repre-
senting 6.9% of patients; MSS with mutations in
KRAS representing 35% of tumors; and MSS lack-
ing KRAS or BRAF mutations representing the main
proportion (49%) of all CRCs. Two types are mismatch
repair deficient (MSI): MSI caused by MLH1 methyla-
tion and BRAF mutations representing 6.8% of the
patients, and MSI without BRAF mutation or familial
CRC representing roughly 2.6% of the tumors10.
The association of these subtypes with survival
reflects that types 4 and 5 have the lowest mortal-
ity, mainly type 5. Type 2 has the highest disease
mortality as well as type 3 that shows high mortal-
ity. In summary, all reports agree that MSI-H con-
fers good prognosis and KRAS and BRAF muta-
tions contribute to worse prognosis. Patients bearing
MSS tumors with BRAF and KRAS mutations show
Figure 1. Representation of the five molecular
subtypes described by Jass8. Overlapping of the
molecular features between subtypes is shown.
MSI: microsatellite instable; CIMP: CpG island
methylator phenotype; MSS: microsatellite stable;
CIN: chromosomal instable.
Nopartofthispublicationmaybereproducedorphotocopyingwithoutthepriorwrittenpermissionofthepublisher. ©PermanyerPublications2016
- 4. Mateo Paz-Cabezas, et al.: CRC Molecular Classification
CANCERCHEMOTHERAPYREVIEWS
69
poor survival. Patients with MSS tumors without
KRAS or BRAF mutations have longer survival times,
similar to patients with MSI-H tumors whether BRAF
mutations are present (sporadic) or absent (famil-
ial)10. Even taking into account mutually exclusive
parameters such as MSS and MSI, certain charac-
teristics are shared between them such as BRAF
mutations and CIMP-H or diploid genome.
This classification of CRC in five subtypes is not
used in everyday clinical practice since these sub-
types are not homogeneous and significant over-
lapping among them is present. Only the absence
of KRAS mutations is used in order to select pa-
tients that respond to anti-epithelial growth factor
receptor (anti-EGFR) therapy in stage IV patients.
Domingo, et al. proposed a slightly different clas-
sification in six groups based on the same param-
eters. First they considered two groups MSI-positive
and CIN-positive since there was almost no overlap
between them. Then BRAF mutations were consid-
ered in the MSI group and TP53 mutations were
added to the CIN-positive group. One group was
NRAS mutant, since NRAS mutations were not as-
sociated with any other molecular variable. The six
groups were: (i) MSI and/or BRAF-mutant; (ii) CIN-
positive and/or TP53-mutant with wild-type (WT)
KRAS and PIK3CA; (iii) KRAS and/or PIK3CA mutant,
CIN-positive, TP53-WT; (iv) KRAS and/or PIK3CA
mutant, CIN-negative, TP53-WT; (v) NRAS mutant;
and (vi) no mutations. Group (iii) had the worse sur-
vival; unfortunately they did not find an MSI group
with better clinical outcome as other authors report11.
Classification Based
on Genome-Wide DNA Mutations
Searching for driver mutations in CRC was ap-
proached in an important initiative of The Cancer
Genome Atlas Network, in which exome sequenc-
ing, DNA copy number, promoter methylation, and
gene expression (mRNA and microRNA) were mea-
sured in 276 patients with CRC12. The main feature
considered was the frequency of mutation, distin-
guishing a group of 16% hypermutated tumors in
which a high percentage (75%) were MSI as ex-
pected and showed a high ratio of CIMP pheno-
type and BRAF mutations. MSI was caused by ei-
ther MLH1 silencing or somatic mutations on gene
repairing genes. Non-hypermutated tumors did not
show main differences between them related to DNA
methylation, copy number, or gene-expression pat-
terns. The DNA methylation patterns identified four
subgroups: two clusters were CIMP and the other
two non-CIMP clusters that predominately were non-
hypermutated tumors. Gene expression profiles iden-
tified three main clusters; one significantly overlapped
with CIMP-H and enriched with hypermutated tu-
mors and MSI, but the others did not correlate with
any other subgroup, although one showed invasive
characteristics and the other was CIN predomi-
nately. In most CRCs ( 90%), one or more mem-
bers of the WNT signaling pathway are mutated,
mainly the APC gene, causing WNT signaling to be
upregulated in both in hyper- and non-hypermutat-
ed tumors.
Novel Colorectal Cancer
Classifications Based
on Expression Profiling
The analysis of tumor heterogeneity was consid-
erably improved with the emergence of genomic
methodologies, particularly transcriptomics. Micro-
array analysis of gene expression constitutes an
effective tool to search for all the genes that are
active in a specific tumor, identifying molecular bio-
markers and developing novel genomic classifiers.
Microarrays analyze areas of the genome where
there has been loss or duplication of material, dis-
cover new key genes, and examine globally how
basic cell functions are modified to identify new
biological pathways that are altered. Molecular
classification assessed by genome-wide expres-
sion analysis is important because it reflects the
underlying mechanisms of carcinogenesis and has
been shown to be crucial to classify cancer. Su-
pervised analysis of gene expression has been
used to discover gene signatures to identify pa-
tients at risk of recurrence in CRC. At the present
time, two extensively validated gene signatures,
Oncotype-DX and ColoPrint13,14
, are being used in
the clinic to select stage II/III patients at higher risk
of recurrence. Recently an elegant report found
that lack of CDX2 expression identified a small
subgroup of high-risk stage II CRC patients who
seem to benefit from adjuvant chemotherapy15
. Un-
supervised analysis is a different strategy. With this
approach, new subtypes of tumors can emerge or
the existing classification may be redefined, with the
result being more uniform groups of tumors. Cluster-
ing methods group together samples with similar
expression profiles; differential gene sets and bio-
logical pathways characterize each tumor subtype,
indicating underlying mechanisms of carcinogen-
esis that may be used for the selection of targeted
therapeutic procedures.
Recently, CRC molecular classifications based
in transcriptional profiling have been reported. Our
group identified four robust molecular subtypes, (i)
low-stroma subtype, the largest group accounting
for 40% of the tumors; (ii) immunoglobulin-related
Nopartofthispublicationmaybereproducedorphotocopyingwithoutthepriorwrittenpermissionofthepublisher. ©PermanyerPublications2016
- 5. CANCER CHEMOTHERAPY Rev. 2016;11CANCERCHEMOTHERAPYREVIEWS
70
subtype, including 13% of the samples; (iii) high-
stroma subtype comprising 25% of the tumors; and
(iv) mucinous subtype that comprise 16% of the
samples. Additionally, we found a small fraction
(6%) of unclassified samples. These tumor sub-
types are associated with stroma, mucinous tu-
mors, MSI, BRAF mutations, and nuclear β-catenin,
but are not correlated with the traditional histo-
pathological classification. Patients carrying tumors
with low stroma content have better prognosis16.
Subsequently, another group stratified CRC pa-
tients in five tumor subtypes. Three types were
mesenchymal with an epithelial-mesenchymal tran-
sition (EMT) expression signature: subtype 1.1 ac-
counting for 19% of the tumors; subtype 1.2 com-
prising 15% of the samples higher proportion of
MSI and immune system-related; and subtype 1.3
comprising 11% of the tumors. Two subtypes were
epithelial; subtype 2.1 with 23% of the samples and
genes related to stress response and immune sys-
tem-related; and subtype 2.2 comprising 32% of
the tumors and upregulation of genes related to
cell cycle. This study confirmed that our high-stro-
ma subtype corresponds to a subtype defined by
a gene signature associated with EMT and sug-
gests that these groups may respond differently to
chemotherapy treatment17.
Then, Sadanandam, et al. reported a CRC clas-
sification in six subtypes that were named de-
pending on the type of genes expressed in each
subtype: (i) stem-like, comprising 19% of the sam-
ples with high expression of mesenchymal genes,
Wnt pathway, and worse survival; (ii) inflamma-
tory, accounting for 18% of the tumors with in-
creased expression of chemokines and interfer-
on-related genes and higher proportion of MSI
tumors; (iii) transit-amplifying (TA), the main and
heterogeneous group with 28% of the tumors
and higher expression of WNT targets, and this
subtype was subdivided in two groups depending
on the response to cetuximab CR-TA or CS-TA for
cetuximab resistant or sensitive; (iv) goblet-like
comprising 15% of the tumors and higher ex-
pression of TFF3, MUC2, and good survival; and
(v) enterocyte, comprising 20% of the tumors orig-
inated from the cells of the top of the crypt18.
Simultaneously, De Sousa e Melo, et al. reported
a CRC classification in three molecular subtypes;
CCS1 accounting for 49% of the tumors, CIN, and
higher proportion of KRAS mutations; CCS2 com-
prising 24% of the tumors and higher proportion
of MSI and CIMP; and CCS3 comprising 27% of
the tumors, increased MSS and CIMP, is origi-
nated in sessile serrated adenomas that show
upregulation of genes related to matrix remodel-
ing and EMT CCS3 tumors have the worse clinical
outcome19.
Marisa, et al. classified colon cancer in six
subtypes: C1, C2, C3, C4, C5, and C6, compris-
ing 21, 19, 13, 10, 27, and 10% of the samples,
respectively. Subtypes C1, C5, and C6 showed
higher CIN and CIMP phenotypes. These three
subtypes did not show major molecular or clinico-
pathological differences between them. Subtype
C2 is enriched in MSI tumors, BRAF mutations,
and upregulation of the immune system genes; C3
have more KRAS mutations; C4 and C6 showed
higher levels of EMT and worse survival; C1 and
C5 showed a conventional colon cancer pheno-
type; and C2, C3, C4, and C6 showed a serrated
phenotype20.
Budinska, et al. identified five tumor subtypes:
A first group defined as “surface crypt-like (A)”
showing low EMT, increased expression of metallo-
thionein, serrated features, and better survival. A
second group, “lower crypt-like (B)”, with similar
features to group A but higher activation of WNT
pathway and tubular morphology. A third group
defined by a higher proportion of CIMP features
“CIMP-H-like (C)”, MSI, mutations in BRAF, and
associated with immune response. A “mesenchy-
mal (D)” group, with high expression of EMT/stroma
genes and low expression of proliferation-associat-
ed genes. And a fifth “mixed (E)” subgroup with
mixed characteristics. Groups C and D are associ-
ated with poor survival and subtypes A and B had
better prognosis21.
Roepman, et al. described three subgroups.
Group A is characterized by a higher proportion of
BRAF mutations, MSI, and the best prognosis.
Group B shows higher proliferation index, MSS,
BRAF wt, worse prognosis and obtains benefit from
chemotherapy. Both A and B subtypes show up-
regulation of epithelial markers. Group C have
upregulated mesenchymal markers, the worst
prognosis, low proliferation, and show no benefit
from adjuvant chemotherapy22.
The number of different subtypes described in
these studies fluctuates from 3-6, and clinical and
biological interpretation of each subtype is barely
in agreement. However, relevant features coincide
among the different classifications. All these stud-
ies identified a subtype rich in MSI tumors. There
was a coincidence in important features such as
epithelial or mesenchymal structure, higher trans-
forming growth factor (TGF)-beta pathway linked to
epithelial-mesenchymal transition (EMT) and poor
survival (Fig. 2).
In order to translate molecular classification into
the clinic, there was a need to obtain a consensus
among these studies. With this goal, an interna-
tional consortium, the Colorectal Cancer Subtyping
Consortium (CRCSC), was created to obtain a con-
sensus among the reported molecular subtypes.
Nopartofthispublicationmaybereproducedorphotocopyingwithoutthepriorwrittenpermissionofthepublisher. ©PermanyerPublications2016
- 6. Mateo Paz-Cabezas, et al.: CRC Molecular Classification
CANCERCHEMOTHERAPYREVIEWS
71
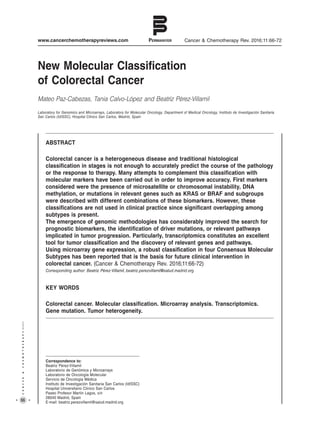
A network-based strategy was developed to
analyze the association of each reported classi-
fication23
and four consensus molecular sub-
types (CMS) were identified with distinctive char-
acteristics (Fig. 3):
– CMS1 (MSI immune), comprising 14% of the
tumors, CIMP-H, hypermutated, MSI and BRAF
mutations, strong immune activation and PD1
activation, increased JAK-STAT and caspases
pathways;
Figura 2. Coincidence of relevant pathways and markers identified in each study. Central circle represents
molecular subtypes reported by Perez-Villamil, et al.16. B: Budinska, et al.21; CCS: De Souza e Melo, et al.19;
M: Marisa, et al.20; R: Roepman, et al.22; S: Schlicker, et al.17; Sd: Sadanandam, et al.18.
MSI: microsatellite instable; TGF: transforming growth factor; EMT: epithelial-mesenchymal transition.
Figura 3. Main features and percentages of the Colorectal Cancer Subtyping Consortium (Guinney, et al.23)
subtypes.
CMS: consensus molecular subtypes; MSI: microsatellite instable; CIMP: CpG island methylator phenotype;
MSS: microsatellite stable; CIN: chromosomal instable; TGF: transforming growth factor; EMT: epithelial-
mesenchymal transition.
CMS1
Immune
MSI
Hypermutated
CIMP high
BRAF mutations
Inmune activation
PD1 activation
14%
CMS2
Canonical
Epithelial
CIN
WNT MYC
Cell cycle
Better outcome
37%
CMS3
Metabolic
Epithelial
Metabolic disreg.
KRAS mutations
13%
CMS4
Mesenchymal
Stromal invation
TGF- activation
EMT activation
Matrix remodelling
Angiogenesis
23%
Nopartofthispublicationmaybereproducedorphotocopyingwithoutthepriorwrittenpermissionofthepublisher. ©PermanyerPublications2016
- 7. CANCER CHEMOTHERAPY Rev. 2016;11CANCERCHEMOTHERAPYREVIEWS
72
– CMS2 (canonical), representing 37% of the
tumors, epithelial, CIN, marked WNT and MYC
signaling activation; cell cycle increased and
better outcome;
– CMS3 (metabolic), comprising 13% of the tu-
mors, epithelial, evident metabolic dysregula-
tion, and KRAS mutations;
– CMS4 (mesenchymal), comprising 23% of the
tumors, TGF-β and EMT activation, stromal
invasion, increased matrix remodeling and an-
giogenesis, and worse clinical outcome.
Additionally, 13% of the samples showed mixed
features, representing a transition phenotype or
caused by higher intra-tumoral heterogeneity.
The CMS subtypes constitute an excellent basis
for the clinical stratification of patients with CRC
and precision medicine.
References
1. Ryerson AB, Eheman CR, Altekruse SF, et al. Annual Report to
the Nation on the Status of Cancer, 1975-2012, featuring the in-
creasing incidence of liver cancer. Cancer. 2016;122:1312-37.
2. Edge S, Byrd D, Compton C, Fritz A, Greene F, Trotti A. AJCC
cancer staging manual. 7th ed. Springer-Verlag, New York, 2010.
3. National Health Service. The NHS Bowel Cancer Screening Pro-
gramme Information for Primary Care. 2010:1-19. Available at:
http://www.marsdenhealthcentre.co.uk/website/B85011/files/Bow-
el_Cancer_Screening_Leaflet.pdf
4. Labianca R, Nordlinger B, Beretta GD, et al. Early colon cancer:
ESMO clinical practice guidelines for diagnosis, treatment and
follow-up. Ann Oncol. 2013;24(Suppl 6):vi64-72.
5. Van Cutsem E, Cervantes A, Nordlinger B, Arnold D; ESMO Guide-
lines Working Group. Metastatic colorectal cancer: ESMO clinical
practice guidelines for diagnosis, treatment and follow-up. Ann
Oncol. 2014;25(Suppl 3):iii1-9.
6. Blanco-Calvo M, Concha A, Figueroa A, Garrido F, Valladares-
Ayerbes M. Colorectal cancer classification and cell heterogeneity:
A systems oncology approach. Int J Mol Sci. 2015;16: 13610-32.
7. Hu H, Krasinskas A, Willis J. Perspectives on current Tumor-
Node-Metastasis (TNM) staging of cancers of the colon and rec-
tum. Semin Oncol. 2011;38:500-10.
8. Jass JR. Classification of colorectal cancer based on correlation
of clinical, morphological and molecular features. Histopathology.
2007;50:113-30.
9. Jia M, Gao X, Zhang Y, Hoffmeister M, Brenner H. Different
definitions of CpG island methylator phenotype and outcomes of
colorectal cancer: a systematic review. Clin Epigenetics. 2016;
8:25.
10. Sinicrope FA, Shi Q, Smyrk TC, et al. Molecular markers identify
subtypes of stage III colon cancer associated with patient out-
comes. Gastroenterology. 2015;148:88-99.
11. Domingo E, Ramamoorthy R, Oukrif D, et al. Use of multivariate
analysis to suggest a new molecular classification of colorectal
cancer. J Pathol. 2013;229:441-8.
12. Muzny DM, Bainbridge MN, Chang K, et al. Comprehensive mo-
lecular characterization of human colon and rectal cancer. Nature.
2012;487:330-7.
13. O’Connell MJ, Lavery I, Yothers G, et al. Relationship between
tumor gene expression and recurrence in four independent stud-
ies of patients with stage II/III colon cancer treated with surgery
alone or surgery plus adjuvant fluorouracil plus leucovorin. J Clin
Oncol. 2010;28:3937-44.
14. Salazar R, Roepman P, Capella G, et al. Gene expression signa-
ture to improve prognosis prediction of stage II and III colorectal
cancer. J Clin Oncol. 2011;2917-24.
15. Dalerba P, Sahoo D, Paik S, et al. CDX2 as a prognostic bio-
marker in stage II and stage III colon cancer. N Engl J Med.
2016;374:211-22.
16. Perez-Villamil B, Romera-Lopez A, Hernandez-Prieto S, et al.
Colon cancer molecular subtypes identified by expression profil-
ing and associated to stroma, mucinous type and different clinical
behavior. BMC Cancer. 2012;12:1.
17. Schlicker A, Beran G, Chresta CM, et al. Subtypes of primary
colorectal tumors correlate with response to targeted treatment
in colorectal cell lines. BMC Med Genomics. 2012;5:66.
18. Sadanandam A, Lyssiotis CA, Homicsko K, et al. A colorectal
cancer classification system that associates cellular phenotype
and responses to therapy. Nat Med. 2013;19:619-25.
19. De Sousa E Melo F, Wang X, Jansen M, et al. Poor-prognosis
colon cancer is defined by a molecularly distinct subtype and
develops from serrated precursor lesions. Nat Med. 2013;19:
614-8.
20. Marisa L, de Reyniès A, Duval A, et al. Gene expression clas-
sification of colon cancer into molecular subtypes: Character-
ization, validation, and prognostic value. PLoS Med. 2013;10:
e1001453.
21. Budinska E, Popovici V, Tejpar S, et al. Gene expression patterns
unveil a new level of molecular heterogeneity in colorectal cancer.
J Pathol. 2013;231:63-76.
22. Roepman P, Schlicker A, Tabernero J, et al. Colorectal cancer
intrinsic subtypes predict chemotherapy benefit, deficient mismatch
repair and epithelial-to-mesenchymal transition. Int J Cancer.
2013;134:552-62.
23. Guinney J, Dienstmann R, Wang X, et al. The consensus molecu-
lar subtypes of colorectal cancer. Nat Med. 2015;21:1 350-6.
Nopartofthispublicationmaybereproducedorphotocopyingwithoutthepriorwrittenpermissionofthepublisher. ©PermanyerPublications2016