Presentation1.pptx, interpretation of x ray on bone tumour.
•Télécharger en tant que PPTX, PDF•
109 j'aime•13,628 vues


Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Presentation1.pptx, interpretation of x ray on bone tumour.
Similaire à Presentation1.pptx, interpretation of x ray on bone tumour. (20)
Plus de Abdellah Nazeer
Plus de Abdellah Nazeer (20)
Dernier
Dernier (20)
Presentation1.pptx, interpretation of x ray on bone tumour.
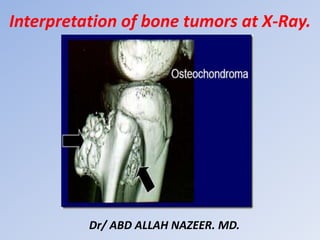
- 1. Interpretation of bone tumors at X-Ray. Dr/ ABD ALLAH NAZEER. MD.
- 39. Osteochondroma: Long bones++ The lesion is composed of cortical and medullary bone protruding from and continuous with the underlying bone. The areas of osseous continuity between parent bone and osteochondroma may be broad, involving a large portion of the bone circumference (dimension of the lesion base exceeding its length-sessile osteochondroma), or narrow, with a bulbous tip (pedunculated osteochondroma). Identifying the characteristic cortical and medullary continuity between lesion and parent bone on radiographs is dependent on lesion type (sessile or pedunculated), location, and image projection. This relationship is usually well delineated in lesions of long bones, particularly pedunculated osteochondromas, with standard radiographic projections (although often only on one view) . However, in osteochondromas of flat bones with complex anatomy (i.e., pelvis, spine, scapula) and sessile lesions, the continuity and thus the diagnosis may not be apparent on radiographs alone . Pedunculated lesions usually point away from the nearest joint owing to the forces of the overlying tendons and ligaments (although not typically attached to the osteochondroma.
- 42. X-ray appearance of different exostoses. (a) Solitary exostosis in a femur. (b) Multiple exostoses in the knee joint, antero-posterior view. (c) Multiple exostoses in the knee joint, lateral view. (d) Multiple exostoses in the upper hip and trochanter (arrows indicate the exostoses sites).
- 45. Osteoid osteoma.
- 46. Typical osteoid osteoma in the femur. Notice the extensive cortical broadening.
- 48. Osteoblastoma in a child.
- 49. Osteoblastoma of the distal radius.
- 50. Osteoblastoma of the right pubic ramus.
- 54. Unicameral bone cyst with fracture and fallen fragment sign.
- 56. Aneurysmal bone cyst - Proximal tibia.
- 57. Aneurysmal bone cyst - Distal tibia.
- 61. Giant cell tumor of the distal ulna.
- 62. Giant cell tumor of the distal radius.
- 64. Cortical fibrous defects and non-ossifying fibromas in children and young adults:
- 69. Fibrous Dysplasia • Long lesion in a long bone (often occurs in proximal femur). • Expansion and bone deformity • Lytic but becomes ground-glass in appearance as the matrix calcifies, and then becomes sclerotic. • Asymptomatic, but can fracture • No periosteal reaction • May be single or multiple lesion in different locations.
- 71. Fibrous dysplasia (polyostotic form).
- 72. Fibrous dysplasia: various presentations with or without sclerotic margin, with ground glass appearance, with calcifications or ossifications.
- 74. Fibrous dysplasia with Coxa vara of proximal femur.
- 75. Enchondroma • Most commonly seen in the phalanges • Asymptomatic but commonly fractures • Well-defined with narrow zone of transition • Lobulated • Can become slightly expansile • Causes endosteal scalloping and cortical thinning • Ollier's Disease = Multiple enchondromas • Maffuci's Syndrome = Multiple enchondromas with soft tissue hemangiomas • Contain calcified chondroid matrix (irregular, speckled) when located away from phalanges.
- 77. Enchondroma - Proximal humerus.
- 78. Plain X-Ray: Enchondroma of Proximal Phalanx.
- 79. A child with Ollier’s disease: a non-hereditary, sporadic, skeletal disorder characterized by multiple enchondromas
- 80. Ollier’s disease
- 81. Mafucci’s syndrome. Plain radiograph of the left hand. Note multiple enchondromas and soft-tissue hemangiomas with intralesional phleboliths.
- 84. Chondromyxoid fibroma - Proximal tibia.
- 88. Chondroblastoma.
- 89. Chondroblastoma.
- 92. Synovial chondromatosis – Shoulder.
- 93. Chordoma: • Uncommon malignant tumours: 40% of all sacral tumors • Location • 50% occur in sacrum, • • • 40% of all sacral tumors • Most common in 4th or 5th sacral segment • 35% at skull base around clivus (Benign tumors but may locally invade and compress) • 15% in remainder of spine: Cervical spine most common • Occurs between the ages of 30-70 with a 2:1 male: female ratio • Imaging Findings • Large presacral mass (>10cm) with displacement of the rectum and/or Bladder • Solid tumor with cystic areas in 50% • Destroys multiple sacral and coccygeal segments • Sequestered bone fragments are common • Sclerotic rim in 50% • May have amorphous calcifications, especially peripherally • May cross the sacroiliac joint
- 95. Sacral chordoma.
- 96. Chordoma of skull base.
- 98. Brown tumor.
- 99. Brown tumor at the femur diaphysis.
- 101. Adamantinoma of the proximal tibia.
- 102. Adamantinoma Tibia.
- 105. Skull and femur hemangioma.
- 106. Computerized tomography demonstrates lesions with osseous spicules in keeping with hemangiomas involved with left frontal bone, supraorbital wall, sphenoid sinus and ethmoid. The central portion of this lesion revealed subtle striated trabeculations and retained a thin sclerotic rim of peripheral bone condensation, and the boundary was clear. Both the inner and the outer tables of the skull were eroded
- 107. Hemangioma of the Long Bones
- 108. Intraosseous Hemangioma of the Nasal Septum.
- 110. Eosinophilic granuloma – Humerus.
- 111. Various presentations of eosinophilic granuloma.
- 112. Monostotic and polyostotic eosinophilic granuloma in the skull. Eosinophilic granuloma in the skull.
- 114. Ewing sarcoma.
- 115. Ewing sarcoma arising from the right iliac bone.
- 116. Ewing sarcoma of femur. Frontal radiograph and lateral radiographs of the femur demonstrate mottled, osteolytic lesion (blue circle) with poorly marginated edges in the diaphysis of the bone. There is sunburst periosteal reaction (red circle) and lamellated periosteal reaction (white arrows).
- 117. Ewing sarcoma
- 119. (a) X-ray anteroposterior and lateral views of proximal tibia and knee joint showing diaphyseal osteosarcoma of tibia with sclerosis (arrow), cortical destruction on posteromedial side (arrow heads) and new bone formation in the soft tissues (b) x-ray distal end of femur (anteroposterior and lateral views) showing sclerosis/radio-opacity in sclerosing osteosarcoma.
- 120. X-ray of knee joint anteroposterior views showing surface osteosarcoma: (a) parosteal (b) periosteal. See the under lying cortex is visibly intact in ‘a’ and lifting of periosteum in ‘b’ (red arrow). However, both are on the surface of the bone
- 121. Telangiectatic type of osteosarcoma of the proximal tibia: (a) X-ray anteroposterior and lateral views showing lysis and expansion (b) MRI showing fluid levels.
- 122. Osteosarcoma.
- 125. Chondrosarcoma of the iliac bone and proximal humerus.
- 126. Chondrosarcoma of the distal femur and proximal humerus.
- 128. Chondrosarcoma.
- 135. Typical x-ray appearance of osteolytic bone metastases. Typical x-ray appearance of osteoblastic bone metastases.
- 140. Anteroposterior radiograph of the lower legs demonstrates a permeative, lytic lesion in the metadiaphysis of the left tibia. Note the aggressive periosteal reaction with Codman triangles and soft-tissue extension/swelling. Soft-tissue involvement is easy to appreciate when the left leg is compared with the normal right leg.
- 141. Burkitt's lymphoma of the humerus.
- 142. 62-year-old patient with lymphoma and low back pain. Anteroposterior (A) and profile (B) X-rays showing a diffuse increase in bone density, with erosion on the left side of the L4 vertebral body (arrow).
- 144. The skull x-ray lateral and AP view reveals multiple oil droplet like punched out lytic defects throughout bony calvarium. The appearance is highly suggestive of, but not completely diagnostic for, multiple myeloma.
- 145. Multiple myeloma.
- 150. Thank You.