Drug-Induced Gingival Overgrowth in Hypertensive Patients on Calcium Channel Blockers
•Download as PPTX, PDF•
11 likes•3,170 views

Clinical Oral Diagnosis course DS4 presentation

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Drug-Induced Gingival Overgrowth in Hypertensive Patients on Calcium Channel Blockers
Similar to Drug-Induced Gingival Overgrowth in Hypertensive Patients on Calcium Channel Blockers (20)
Recently uploaded
Recently uploaded (20)
Drug-Induced Gingival Overgrowth in Hypertensive Patients on Calcium Channel Blockers
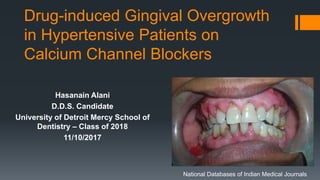
- 1. Drug-induced Gingival Overgrowth in Hypertensive Patients on Calcium Channel Blockers Hasanain Alani D.D.S. Candidate University of Detroit Mercy School of Dentistry – Class of 2018 11/10/2017 National Databases of Indian Medical Journals
- 2. Patient history 53 Years old middle eastern female presented to clinic with chief complaint “I am here to replace my missing teeth” Medical history Hypertension, Allergic to penicillin Patient was diagnosed with Hypertension in 2013 Medication 1) Amlodipine: Calcium Channel Blocker ADRX: dysphagia, erythema multiforme, gingival hyperplasia, maculopapular rash DrugInterX: 1. Antifungal agents: May enhance the adverse effects of calcium channel blockers. 2. Barbituates: May increase the metabolism of calcium channel blockers 3. Carbamazepine: May increase the metabolism of calcium channel blockers 2) Alprazolam: Benzodiazipine, ADRX: dysgeusia, dysphagia, Stevens-Johnson syndrome, syncope Patient had fillings, root canal therapy, crowns, full mouth scaling/root planing, extractions before.
- 3. Intra oral and extra oral Extra oral Nothing significant Intra oral Diastema between #24,25, moderate attrition #22-27, fractured #7,8, 1X1 mm nodule on the lateral border of the tongue. CI: Fibroma
- 4. Original Dx cast 5 views
- 9. Caries risk: HIGH Number of teeth lost to caries: 13 teeth All caries have been treated with amalgam and composite restorations
- 10. Periodontal charting and perio DX Contributing factor Etiologic factor: Plaque and missing teeth Systemic factors: Xerostomia Patient brushes once a day using fluoridated toothpaste and drinks tap water.
- 11. Before After
- 12. Before After
- 13. Prognosis The generalized prognosis is favorable as long as the patient follows the recommended treatment plans and home care. The patient could restore periodontal health especially that she is very compliant, all she needs to improve on is following OHI. The patient is put on periodontal recall every 3 months.
- 14. Objective Patient objective Replace posterior missing teeth Esthetic (fractured #7 and 8) Provider objectives
- 15. Treatment plan Patient is so motivated to get her missing teeth replaced She likes the implant option but she cannot afford it at the moment, we decided to go with RPD/RPD for the time being until financial situation improves She needs to improve on oral hygiene home-care for better results. Possible gingival overgrowth due to CCB therapy has to be addressed because it could interfere with her future implants Periodontal Maintenance, restorative, extraction of hopeless teeth RPD/RPD Maintain regular visits to the dentist, follow OHI, reduce carbohydrate intake to lower caries risk.
- 17. PICO Question In patients with drug-induced gingival overgrowth, would switching patient off of Calcium Channel Blocker to other drug category, as compared to maintenance of Calcium Channel Blocker therapy, reduce the degree of gingival overgrowth?
- 18. Hypertension Persistent elevation of Systolic blood pressure ≥140 mm Hg or Diastolic blood pressure ≥90 mm Hg • Worldwide an estimated 1 billion people have hypertension; about 1 in 3 Americans affected •
- 19. The “Rule of Halves” in Hypertension 1- Only ½ have been diagnosed. 2- Only ½ of those diagnosed have been treated. 3- Only ½ of those treated are adequately controlled. Overall, only 12.5% are adequately controlled
- 20. Therapeutics: Antihypertensive drugs 1) Diuretics 2) Beta-Blockers 3) Calcium Channel Blockers 4) ACE-Inhibitors Choice: → Previous experience of the patient → Cost → Risk profile, target organ damage, clinical cardiovascular or renal disease or diabetes or lung disorder → Patient’s preference • Long acting preparations providing 24-h efficacy on a once daily basis
- 22. What influences Blood pressure? Two factors control blood pressure: 1) Cardiac: Heart rate, Inotropic State, Neural, Humoral. 2) Renal Fluid Volume Control: Renin-Angiotensin-Aldosterone System (RAAS), Atrial Natriuretic Factor. Controlled by sympathetic nervous system by the means of Baroreceptors ( carotid artery and carotid arch)
- 23. What is gingival overgrowth? It is a tissue-specific condition that comes as a side effect for some medications, including calcium channel blockers. It poses a major problem to maintain oral hygiene due to inflammation and disfiguration of gingiva, as well as problems in mastication and bad appearance. Non-surgical approaches are used to reduce the size of lesion by up to 40%. In most cases of severe overgrowth, the recurrence after surgical excision is at a high rate if drug therapies are not altered. According to a study in the Journal of Dental Research, 34% of cases demonstrated recurrence during the 18 months following the surgery regardless of the drug (Trackman and Kantarci 2015). Plaque scores and gingival inflammation appear to exacerbate the level of overgrowth. Three main drug categories cause GO: anticonvulsants, immunosuppressants and calcium channel blockers. They all have similar mechanism of action at the cellular level by inhibiting cellular calcium ion influx.
- 25. Calcium channel blockers (CCB) Calcium channel blockers inhibit the L-type calcium channel on cells and are divided into two major categories based upon their physiologic effects: 1) Dihydropyridines: predominantly vasodilators and have a neutral or increased effect on vascular permeability. Gingival overgrowth is more predominant with this category of CCB. These are subdivided into three categories based on the half-life and their effect on contractility: a) Short-acting (capsule containing liquid)-nifedipine. b) Longer acting with little cardiac depressant activity – felodipine, isradipine, nicardipine, nifedipine – gastrointestinal therapeutic system (GITS) and coat-core (CC) and nisoldipine. c) Long-acting agents with no cardiac depressant activity – amlodipine and lacidipine. 2) Nondihydropyridines: such as verapamil, reduce vascular permeability and affect cardiac contractility and conduction. (Triggle 2003)
- 26. Mechanism of action leading to gingival overgrowth GO is characterized by an accumulation of extracellular matrix within the gingival connective tissue. The mechanism is still unknown. However, there are two suggested theories: a) Non-inflammatory: Defective collagenase activity due to an increased uptake of folic acid, a blockage of aldosterone synthesis in adrenal cortex with a consequent feedback increase in adrenocorticotropic hormone (ACTH) levels and an up-regulation of keratinocyte growth factor. b) Inflammatory: The inflammatory theory suggests that inflammation develops as a result of a direct toxic effect of concentrated drugs in the gingival crevicular fluid, possibly in connection with bacterial plaque. This inflammation may lead to an up-regulation of several cytokine factors and in particular the transforming growth factor beta 1 (TGF-b1).
- 27. Literature search Research via Detroit Mercy Library database using keywords: Hypertension, Amlodipine, drug switch, gingival overgrowth, Pubmed, Science Direct and Journal of Clinical Periodontology Types of information identified: Pubmed: Cohort studies and Case series. Science direct: Cohort studies and Case-control studies. Journal of Clinical Periodontology: Cohort studies and Case-control studies.
- 28. Evidence Chosen Management of periodontal disease in patients using calcium channel blockers – gingival overgrowth, prescribed medications, treatment responses and added treatment costs Ø Fardal, H Lygre Department of Clinical Science, University of Bergen, Bergen, Norwaye.g
- 29. Hypothesis/Purpose/Aim/Objective The aim of this study was to assess the influence of the prescribed CCB medication types and dosages on the frequency and severity of GO, treatment responses, outcomes, substitutions and extra treatment costs. The hypothesis is that these patients experience gingival overgrowth and long- term recurrence of gingival overgrowth.
- 30. Methods: Study Design, Setting What type of study was done? Case Control Study (Level of Evidence III) The study was conducted in real life circumstances All patients were selected from a periodontal practice. Patients were scored using a Gingival Overgrowth Index (GOI) and Horizontal Miranda & Brunet index (MBi) GOi:Measured GO in vertical direction: 0 - No overgrowth, feather edge gingival margin Grade 1 - Blunting of gingival margin Grade 2 - Moderate gingival overgrowth (one third crown length) Grade 3 - Marked gingival overgrowth (more than one thirds of crown) MBi: Measured GO in buccolingual direction both for buccal and lingual/palatal papilla. 0 – papillary thickness < 1 mm 1 – papillary thickness 1-2 mm 2 – papillary thickness > 2 mm In this study they combined these two indices into an integrated grading system of: 0 (absence of enlargement) 1 (light/moderate) 2 (severe).
- 31. Methods: Subjects One hundred and twenty-four patients (58 females, 66 males, 4.6% of the patient population) were using CCBs. 103 patients were assessed. Average age was 66.53 years (SD. 9.89, range 42–88) and the observation time was 11.30 years (SD 8.06, range 1–27). Eighty-nine patients had GO, 75 of these required treatment for GO. All patients completed a similar course of initial periodontal treatment, which included non-surgical therapy and surgical intervention Who was included in and who was excluded from the study? All patients who were diagnosed with chronic periodontitis and had received initial periodontal treatment by the clinical investigator (ØF) between 1986 and 2014 were assessed for the following inclusion criteria: Using or having used CCBs during the initial treatment and/or during the supportive periodontal therapy (SPT). The following data were collected anonymously from each patient: gender, age at reassessment, medical history, smoking (number of cigarettes pr. day at initial examination), number of SPT years, number of teeth present at initial examination, number of teeth lost. Oral hygiene was assessed by the clinician at each of the SPT visits based on the distribution and abundance of plaque. It was noted whether the patients were specifically referred for GO, the level of GO, type and dosages of CCB, how many years the drugs had been used, if and when the medications were terminated, changes in dosages, use of other prescribed drugs, changes in GO classifications, reasons for not terminating/replacing drugs, treatment responses, retreatment during SPT.
- 32. Methods: Interventions All patients completed a similar course of initial periodontal treatment, which included non-surgical therapy and surgical intervention. Initial therapy included oral hygiene instruction, scaling and root. The whole mouth was treated over a series of visits at 2–4 week intervals. Periodontal surgery was prescribed for patients who had sites with bleeding on probing with persistent deep pockets (≥7 mm) at re-assessment six weeks after completion of the initial therapy. The extent of overgrowth as well as the healing following non-surgical and surgical therapy was used to assess if cessation or replacement of the prescribed medication was recommended. Periodontal Maintenance was done either by perdiodontist or general dentist. Retreatment: Treatment over and above the prescribed periodontal maintenance and included non-surgical treatment and/or surgical treatment. Retreatment was judged necessary in two clinical situations. One was when deep pockets (≥7 mm) were identified which exhibited bleeding on probing. The other was when increases in pocket depth (≥3 mm) were identified which was accompanied by persistent bleeding on probing at three successive SPT visits. During the maintenance period, sites with increasing probing depths or gingival overgrowth were treated with SC/RP. If there was clinical signs of residual subgingival calculus which could not be removed non-surgically with the presence of persistent inflammation or marked gingival overgrowth, surgical treatment was performed using gingivectomy/modified Widman flap, laser and/or electro-surgery. Systemic antibiotic therapy was used in cases of acute exacerbation of periodontal disease.
- 33. Methods: Outcomes and Results Mean values, standard deviations and range were calculated for the variables mentioned previously. The study did not mention randomization or blind assessment. The study statistically assessed multiple factors for significant difference (p < 0.05), the area of interest here is terminating/replacing CCB and whether it makes a significant difference in reducing gingival overgrowth. Terminating or replacing with alternatives to CCBs resulted in significant decreases in gingival overgrowth (p = 0.00016, p = 0.00068) respectively. However, terminating/replacing did not result in ultimate resolution of the gingival overgrowth, but termination reduced the GOI from 3.45 to 1.45 and replacement reduced GOI from 3.20 to 1.84. The patients received the same initial therapy, the periodontal maintenance treatment depended on their clinical evaluation upon recall.
- 34. Results
- 35. What are the alternative drugs? 1) Differenct CCB: Verapamil. 2) ACE- Inhibitor: Enalapril 3) Beta-Blocker: Atenolol 4) Thiazide Diuretics: Hydrochlorothizide.
- 36. Conclusions More than 75% of patients using CCBs in the present periodontal practice needed treatment for GO. Stopping or replacing the medication with non-CCB antihypertensives significantly reduced the GO. Nearly half of the patient population experienced long-term recurrence of their GO requiring considerable extra treatment over and above the supportive therapy. The long-term tooth loss was considerably higher for patients using CCB than other populations reported on from the same practice setting. The results supports the aim of the study, terminating/replacing CCB significantly reduced the level of gingival overgrowth.
- 37. Evidence applied to case The study directly answers my PICO question. My patient is not currently suffering from gingival overgrowth, however, patient is considering implants for future treatment plan and this gingival overgrowth is a potential issue for patient on CCB therapy. The results recommend consulting with the physician to evaluate the possibility of terminating/replacing CCB with another antihypertensive drug category.
- 38. How case was treated My patient received full mouth SC/RP, and currently on 3 month recall for periodontal maintenance. The patient is in process for RPD/RPD treatment. Critique: The integrated gingival overgrowth index was not explained in details with specific measurements. I think I have been doing a good job treating this patient; significant improvement in periodontal health, all restorative work has been completed, addressed her esthetic concerns and extracted her hopeless teeth. The current plan is to finish the RPD/RPD and maintain regular visits for periodontal maintenance. Patient will seek implant treatment later.
- 39. References 1- Trackman, P. C. & Kantarci, A. (2015) Molecular and clinical aspects of drug induced gingival overgrowth. Journal of Dental Research 94, 540–546. 2- Triggle, D. J. (2003) Drug targets in the voltagegated calcium channel family: why some are and some are not. Assay Drug Development Technology 1, 719–733 3- Miranda, J., Brunet, L., Roset, P., Farre, M. & Mendieta, C. (2012) Reliability of two measurement indices for gingival enlargement. Journal of Periodontal Research 47, 776–782. 4- Fardal, Ø. & Grytten, J. (2013) A comparison of teeth and implants during maintenance therapy in terms of the number of disease-free years and costs – an in vivo internal control study. Journal of Clinical Periodontology 40, 645–651. 5- Mavrogiannis, M., Ellis, J. S., Thomason, J. M., & Seymour, R. A. (2006). The management of drug‐induced gingival overgrowth. Journal of clinical periodontology, 33(6), 434-439. 6- Trackman, P. C., & Kantarci, A. (2015). Molecular and clinical aspects of drug-induced gingival overgrowth. Journal of dental research, 94(4), 540-546.