A System to Improve Medication Safety in the Setting of Acute Kidney Injury

Inadequate dosing for nephrotoxic or renally cleared drugs in patients with acute kidney injury is common, though recent clinical decision support systems have proven successful in decreasing errors. Within the care provider order entry (CPOE) system, we developed a set of interventions with varying levels of workflow intrusiveness. The interventions alert providers about significant changes in renal function, defined as a 0.5 mg/dl change in serum creatinine, and advise discontinuation or modification of nephrotoxic or renally cleared drugs. Passive alerts appear as persistent text within the CPOE system and on rounding reports, requiring no provider response. More intrusive exit check alerts interrupt the provider at the end of the CPOE session, requiring the provider to modify or discontinue the drug order, assert the current dose as correct, or defer the alert. We evaluated the initial provider response to the interventions, using as our outcomes the resulting actions for alerted orders and the responses selected by providers as required by the exit check alert. Preliminary analysis shows the interventions to be effective in significantly improving provider response to changes in renal function, though initial provider response suggests future enhancements to increase success.
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to A System to Improve Medication Safety in the Setting of Acute Kidney Injury
Similar to A System to Improve Medication Safety in the Setting of Acute Kidney Injury (20)
More from Allison McCoy
More from Allison McCoy (11)
Recently uploaded
Recently uploaded (20)
A System to Improve Medication Safety in the Setting of Acute Kidney Injury
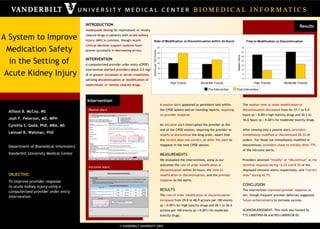
- 1. A System to Improve Medication Safety in the Setting of Acute Kidney Injury INTRODUCTION Inadequate dosing for nephrotoxic or renally cleared drugs in patients with acute kidney injury (AKI) is common, though recent clinical decision support systems have proven successful in decreasing errors . INTERVENTION A computerized provider order entry (CPOE) intervention alerted providers about 0.5 mg/dl or greater increases in serum creatinine , advising discontinuation or modification of nephrotoxic or renally cleared drugs . Allison B. McCoy, MS Josh F. Peterson, MD, MPH Cynthia S. Gadd, PhD, MBA, MS Lemuel R. Waitman, PhD Department of Biomedical Informatics Vanderbilt University Medical Center OBJECTIVE: To improve provider response to acute kidney injury using a computerized provider order entry intervention. A passive alert appeared as persistent text within the CPOE system and on rounding reports, requiring no provider response . An intrusive alert interrupted the provider at the end of the CPOE session, requiring the provider to modify or discontinue the drug order, assert that the current dose was correct , or defer the alert to reappear in the next CPOE session. MEASUREMENTS We evaluated the interventions, using as our outcomes the rate of order modification or discontinuation within 24 hours, the time to modification or discontinuation , and the provider response to the alerts. RESULTS The rate of order modification or discontinuation increased from 29.8 to 48.9 actions per 100 events (p < 0.001) for high toxicity drugs and 28.1 to 36.4 actions per 100 events (p = 0.001) for moderate toxicity drugs. The median time to order modification or discontinuation decreased from for 27.1 to 9.0 hours (p < 0.001) high toxicity drugs and 30.3 to 16.6 hours (p < 0.001) for moderate toxicity drugs. After viewing only a passive alert, providers immediately modified or discontinued 28.3% of orders. For those not immediately modified or discontinued, providers chose to initially defer 77% of the intrusive alerts. Providers selected “modify” or “discontinue” as the terminal response during 12.2% and 8.3% of the displayed intrusive alerts respectively, and “correct dose” during 42.7% . CONCLUSION The intervention improved provider response to AKI , though frequent provider deferrals suggested future enhancements to increase success. ACKNOWLEDGEMENT: This work was funded by T15 LM007450-06 and R03 LM009238-02. Results Intervention Passive Alert Intrusive Alert Pre-Intervention Post-Intervention