2. Introduction
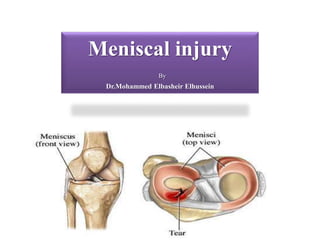
• The menisci are fibrocartilaginous structures that are semilunar in shape
and wedge-shaped in cross-section.
• Two menisci(medial and lateral) exist between the femoral and tibial
articulation.The femoral articulating meniscal surface is concave,whereas
the tibial articulating surface is convex.These surfaces conform to the
convex and concave opposing chondral surfaces, respectively.
• The conforming articulation provides perfect congruency between
the femoral condyle, meniscus,and tibial plateau, which establishes
the foundation for the biomechanical function of the menisci.
5. Introduction
• Acute tears are often
related to trauma, most
frequently as a result of
a twisting motion.
• Most common in active
people aged 10–45.
6. Introduction
• Early diagnosis and
treatment of acute meniscal
tears can significantly
affect the short-term
meniscal viability and
subsequent long-term
articular chondral
protection.
14. Anatomy
• Innervation
– peripheral two-thirds innervated by Type I and II nerve endings
– posterior horns have highest concentration of mechanoreceptors
16. Stability
• medial meniscus
– posterior horn of medial
meniscus is the
main secondary
stabilizer to anterior
translation
• lateral meniscus
– is less stabilizing and
has 2X the excursion of
the medial meniscus
17. Function
• Force transmission
1. increasing
congruency
2. shock-absorption
3. transmits 50%
weight-bearing load
in extension, 85% in
flexion
18. Meniscal Pathology
• Epidemiology
– most common indication
for knee surgery
– higher risk in ACL
deficient knees
• Location
– medial tears
– lateral tears
• more common in
acute ACL tears
19. Injury & Healing potential
• Tears in peripheral 25% red zone
– can heal via fibrocartilage scar formation
• Tears of central 75%
– have limited or no intrinsic healing ability
20. Classification
• Descriptive classification
– location
• red zone (outer third, vascularized)
• red-white zone (middle third)
• white zone (inner third, avascular)
– size
– pattern
1. vertical/longitudinal
2. bucket handle
3. oblique/flap/parrot beak
4. radial
5. horizontal
6. complex
21. • The repairability of a meniscus depends on a number of factors these
include:
1. Age/strength
2. Activity level
3. Tear pattern
4. Chronicity of the tear
5. Associated injuries (anterior cruciate ligament injury)
6. Healing potential
27. Presentation
Symptoms
1. Pain, often along the joint line of the knee .
2. Swelling (“effusion” in the joint).
3. Inability to fully extend or flex the knee without discomfort .
4. Locking or catching of the knee.
5. Weakness of the leg.
28. Presentation
Signs
• Joint line tenderness
• Effusion
• Positive McMurray's test
29. Imaging
• X-ray:
– Images (normally during weightbearing)
to rule out other conditions .
30. Imaging
• MRI
– Indications
• MRI is most sensitive diagnostic test, but also has a high false
positive rate
31. Treatment
Non-operative
Rest, NSAIDS, rehabilitation
• indications
– indicated as first line of treatment for degenerative tears
32. Treatment
Operative
– The definitive treatment of meniscal tears involves either repair or
excision of the pathologic tissue.
– Surgery.
33. Treatment
The indications for arthroscopy include
(1) symptoms of meniscal injury
(2) positive physical findings
(3) failure to respond to nonsurgical
treatment
(4) ruling out other causes of knee pain
34. Treatment
– Partial meniscectomy
• indications
– tears not amenable to repair (complex, degenerative, radial tear
patterns)
• outcomes
– >80% satisfactory function at minimum follow-up
– 50% radiographic changes (osteophytes, flattening, joint space
narrowing)
35. Treatment
– Meniscal repair
• indications
– best candidate for repair is a tear with the following
characteristics
» peripheral in the red zone (vascularized region)
» rim width correlates with the ability of a meniscal repair to
heal (lower rim width has better blood supply)
» vertical and longitudinal tear
» 1-4 cm in length
» acute repair combined with ACL reconstruction
36. Treatment
• outcomes
– 70-95% successful
– highest success when done with concomitant ACL
reconstruction
– poor results with untreated ACL-deficiency (30%)
37. Treatment
– Total meniscectomy
– of historical interest only
• outcomes
– 20% have significant arthritic lesions and 70% have
radiographic changes three years after surgery
– 100% have arthrosis at 20 years
– severity of degenerative changes is proportional to % of the
meniscus that was removed
38. Treatment
• Techniques of Partial
Meniscectomy
– approach
• standard arthroscopic
approach
– technique
• minimize resection
• do not use thermal (heat
probes)
– postoperative
• early active range of motion
• prolonged immobilization
(10 weeks) is detrimental to
healing in a dog model
Typical locations of arthroscopic surgery
incisions in a knee joint following surgery for a
tear in the meniscus
39. Treatment
• Meniscal repair
– approach
1-inside-out technique
– considered gold standard
– medial approach to capsule
– lateral approach to capsule
2-all-inside technique (suture devices with plastic or
bioabsorbable anchors)
– most common
– many complications (device breakage, iatrogenic chondral
injury)
3-outside-in repair
– useful for anterior horn tears
– open repair
– uncommon except in trauma, knee dislocations
42. Treatment
• Side effects of meniscectomy include:
1. The knee loses its ability to transmit and distribute load and absorb
mechanical shock.
2. Persistent and significant swelling and stiffness in the knee.
3. The knee may be not fully mobile, there may be the sensation of
knee locking or buckling in the knee.
4. The full knee may be in full motion after tear of meniscus
43. Treatment
• Meniscal Transplantation
– technique
• bone to bone healing
with plugs at each horn
or a bridge between
horns
• peripheral vertical
mattress sutures
• correct sizing of the
allograft is
essential (commonly
based on radiographs,
within 5-10% error
tolerated)
44. Prevention
There are three major ways of
preventing a meniscus tear.
1. wearing the correct footwear.
2. Strengthening and stretching the
major leg muscles.
3. learning proper technique for the
movement.
Proper parallel squat form to improve knee
stability
These tears are more likely to produce a moveable fragment that can catch in the knee and therefore require surgical treatment
This treatment is particularly critical in a younger population
The menisci are C-shaped wedges of fibrocartilage located between the tibial plateau and femoral condyles.
The menisci contain 70% type I collagen.[3]
The larger semilunar medial meniscus is attached more firmly than the loosely fixed, more circular lateral meniscus.
The anterior and posterior horns of both menisci are secured to the tibial plateaus.
Anteriorly, the transverse ligament connects the 2 menisci; posteriorly, the meniscofemoral ligament helps stabilize the posterior horn of the lateral meniscus to the femoral condyle.
The coronary ligaments connect the peripheral meniscal rim loosely to the tibia.
Although the lateral collateral ligament (LCL) passes in close proximity, the lateral meniscus has no attachment to this structure
Attachment
Blood supply
1-medial inferior genicular artery supplies peripheral 20-30% of medial meniscus
2-lateral inferior genicular artery supplies peripheral 10-25% of lateral meniscus
central 75% receive nutrition through diffusion-This presents a problem when there is an injury to the meniscus, as the avascular areas tend not to heal without the essential nutrients supplied by blood vessels.
Which is a sensory receptors that responds to mechanical pressure or distortion.
The menisci are made of
1-fibroelastic cartilage -interlacing network of collagen, proteoglycan, glycoproteins, and cellular elements composed of 65-75% water
2-Collagen- 90 % Type I collagen
3-Fibers -which allow the meniscus to expand under compressive forces and increase contact area of the joint .
the meniscus deepens tibial surface and acts as secondary stabilizer
The meniscus functions to optimize force transmission across the knee and this will be done by
1-increasing congruency -increases contact area leads to decreased point loading
2-shock-absorption the meniscus is more elastic than articular cartilage, and therefore absorbs shock.
3-transmits 50% weight-bearing load in extension, 85% in flexion
Epidemiology
most common indication for knee surgery higher risk in ACL deficient knees.
Location
-medial tears- more common than lateral tears the exception is in the setting of an acute ACL tear where lateral tears are more common degenerative tears in older patients usually occur in the posterior horn medial meniscus
-lateral tears -more common in acute ACL tears
Fibrochondrocyte are the cells responsible for healing
pattern
Vertical or longitudinal is more common, especially with ACL tears repair when peripheral
bucket handle vertical tear which may displace into the notch.
oblique/flap/parrot beak may cause mechanical locking symptoms.
radial
horizontal more common in older population may be associated with meniscal cysts
The functional importance of these classifications, however, is to ultimately determine whether a meniscus is repairable..
Normally the medal and lateral menisci appear as low signal bow-tie-shaped structures between the femoral condyles and tibial plateauxThe absent bow tie sign represents the loss of the normal appearance of the menisci on parasagittal MRI images, and is suggestive of meniscal injury.
The double PCL sign appears on sagittal MRI images of the knee when there is a bucket-handle tear of the meniscus
1-often develops due to inflammation and/or bleeding from the injury
5-particularly the quadriceps muscle. This may be evident when trying to perform a straight leg raise or walk up and down stairs.
flex the knee and place a hand on medial side of knee, externally rotate the leg and bring the knee into extension
a palpable pop or click is a positive test and can correlate with a medial meniscus tear
The menisci themselves cannot be visualised with plain radiographs
knee arthroscopy allows quick diagnosis and simultaneous treatment. Recent clinical data shows that MRI and clinical testing are comparable in sensitivity and specificity when looking for a meniscal tear
is indicated in patients who have persistent mechanical symptoms and/or pain and have not responded to a course of nonoperative treatment
The indications for arthroscopy include
(1) symptoms of meniscal injury that affect activities of daily living, work, and/or sports participation, such as instability, locking,
effusion, and pain;
(2) positive physical findings of joint-line tenderness, joint effusion, limitation of motion, and provocative signs, such as pain with squatting, a positive pinch test, or a positive McMurray test;
(3) failure to respond to nonsurgical treatment, including activity modification, medication, and a rehabilitation program; and
(4) ruling out other causes of knee pain identified by patient history, physical examination, plain radiographs, or other imaging studies.
predictors of success
age <40yo
normal alignment
minimal or no arthritis
single tear
rim width is the distance from the tear to the peripheral meniscocapsular junction (blood supply).
Techniques of Partial Meniscectomy
approach
standard arthroscopic approach
technique
minimize resection (DJD proportional to amount removed)
do not use thermal (heat probes)
postoperative
early active range of motion
prolonged immobilization (10 weeks) is detrimental to healing in a dog model
???Meniscal repair
approach
inside-out technique
considered gold standard
medial approach to capsule
expose capsule by incising the sartorius fascia, retracting the pes tendons and semimembranosus posteriorly, and developing the plane between the medial gastrocnemius and capsule.
lateral approach to capsule
expose capsule by developing plane between the iliotibial band and biceps tendon interval, then retract lateral head of gastrocnemius posteriorly
meniscal allografts. Cylindrical bone-plug (C) or keyhole-slot (D) techniques may
F, Second-look arthroscopic views of a lateral meniscal allograft.
There are three major ways of preventing a meniscus tear
The first of which is wearing the correct footwear for the sport and surface that the activity is taking place on
The proper footwear is imperative when engaging in physical activity because one off balanced step could mean a meniscus tear.
The second way to prevent a meniscus tear is to strengthen and stretch the major leg muscles.
The third things learning proper technique for the movement that is taking place For the sports involving quick powerful movements it is important to learn how to cut, turn, land from a jump, and stop correctly