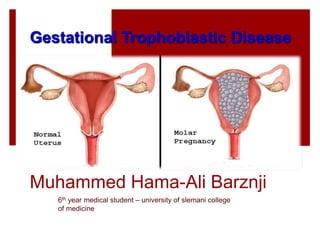
Gestational trophoblastic disease ( Molar pregnancy )
•Download as PPTX, PDF•
82 likes•11,088 views

Mrs. Soz Ali, a 34-year-old woman, presented with vaginal bleeding and nausea. Examination found a bulky uterus consistent with a 10 week gestation. Laboratory tests showed an elevated beta-hCG level of 7981 U/l and ultrasound revealed an increased uterine echogenicity with a "snowstorm" appearance. This is consistent with a diagnosis of complete hydatidiform mole based on the clinical presentation, lab tests, and imaging findings. Complete molar pregnancies carry risks of persistent trophoblastic disease, chemotherapy may be required for treatment.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Gestational trophoblastic disease ( Molar pregnancy )
Similar to Gestational trophoblastic disease ( Molar pregnancy ) (20)
Recently uploaded
Recently uploaded (20)
Gestational trophoblastic disease ( Molar pregnancy )
- 1. Muhammed Hama-Ali Barznji 6th year medical student – university of slemani college of medicine Gestational Trophoblastic Disease
- 2. Gestational Trophoblastic Disease Muhammed Hama-Ali Barznji 6th year medical student – university of slemani college of medicine
- 3. ”for his discoveries of mechanisms for autophagy”
- 4. Mrs Soz Ali 34-year-old woman from Slemani- sarchnar, she is vegetarian, married for 7 years 3rd Gravida ,Para 0 at 14 Ws GA. The previous abortions were at 7&8 weeks. She complains of: 1-Mild vaginal bleeding for 4 days 2-Nausea, and moderate vomiting Case Scenario
- 5. • . bright Red spots commenced & days before which she thought was normal in pregnancy. • However since then the bleeding is almost as heavy as period. there are no clots. mild abdominal pain. • systemically she has nausea for 3 weeks and vommit periodically. • there is no other significant gynaecologically history. Case Scenario
- 6. Examination: the patient had a blood pressure of 100/70 and a pulse of 100 bpm. She was well orientated, afebrile and had a slight pallor. She had some lower abdominal discomfort with more tenderness at the right iliac fossa, but there was no rebound or guarding. On speculum examination: reveals closed cervix with some blood coming from cervical canal. Bimanual examination: uterus feels bulky and soft, approximately 10 week in gestation. There is no adnexal tenderness or cervical excitation Case Scenario
- 7. Investigation Serology ↑ β-hCG: B-HCG was 7981 U/l Cross match and grouping: A+ , Hb was 8.0 g/l Ultrasound : increase uterine echoginicity classically have "snowstorm" appearance with no fetus Gross pathology : "honeycombed uterus" or "cluster of grapes" gross appearance Case Scenario
- 8. Google image US scanning revealed
- 9. Gestational trophoblastic disease (GTD) rare tumors abnormal growth of cells inside a woman's uterus. these tumors start in the cells that would normally develop into the placenta during pregnancy. The term gestational ==> pregnancy. GTD begins in the layer of cells called the trophoblast that normally surrounds an embryo. (Tropho- means nutrition, and -blast means bud or early developmental cell.)
- 10. Classification of gestational Trophoblastic disease WHO Classification Malignant neoplasms of various types of trophoblats Malformations of the chorionic villi that are predisposed to develop trophoblastic malignacies Benign entities that can be confused with with these other lesions Choriocarcinoma Complete Hydatidiform moles Placental site nodule Exaggerated placental site Epithilioid trophoblastic tumors Placental site trophoblastic tumor Partial Invasive
- 12. Risk factors Age: childbearing age (J curve) with extremes of reproductive life associated with an increased incidence. Prior molar pregnancy: an increased risk of further molar pregnancies. one mole < 2%, two molar one in six; following three moles the risk may be as high as one in two Family history: underlying genetic disorder in such cases. Nutrional and socioeconomic factors: low dietary intake of carotene and animal fat
- 13. Hydatidiform Mole The most commonGTD. Hydatidiform moles are not cancerous, but they can develop into cancerous GTDs. Histologically characterized by : Trophoblastic proliferation & Edema of the villous stroma (Hydropic) . Based on the degree and extent of these tissue changes, hydatidiform moles are categorized as either Complete hydatidiform mole. Partial hydatidiform mole.
- 14. A partial hydatidiform mole develops when 2 sperm fertilize a normal egg. These tumors contain some fetal tissue, but this is often mixed in with the trophoblastic tissue. It is important to know that a viable (able to live) fetus is not being formed. A complete hydatidiform mole most often develops when either 1 or 2 sperm cells fertilize an egg cell that contains no nucleus or DNA (an “empty” egg cell). All the genetic material comes from the father's sperm cell. Therefore, there is no fetal tissue.
- 16. Hydatidiform Mole Clinical Presentation: Complete mole: Vaginal bleeding Severe anemia Passage of hydropic villi
- 17. Hydatidiform Mole Usually, in association with, Excessive uterine enlargement Hyperemesis gravidarum Preeclampsia Markedly elevated hCG 100,000 mIU/mL Hyperthyroidism Theca lutein cysts Clinical Presentation: Complete mole:
- 18. Hydatidiform Mole Clinical Presentation: Partial mole: History: Vaginal bleeding Usually diagnosed as missed or incomplete abortion Physical: A uterus small or equal to gestational age
- 20. Feature Partial mole Complete mole Karyotype Most commonly 69, XXX or - XXY Most commonly 46, XX or -,XY Pathology Fetus Often present Absent Amnion, fetal RBC Usually present Absent Villous edema Variable, focal Diffuse Trophoblastic proliferation Focal, slight-moderate Diffuse, slight-severe Clinical presentation Diagnosis Missed abortion Molar gestation Uterine size Small for dates 50% large for dates Theca lutein cysts Rare 25-30% Medical complications Rare 10-25% Postmolar CTN 2.5-7.5% 6.8-20% Features Of Partial And Complete Hydatidiform Moles Clinical Gynecological Oncology 2007 Cunningham et al Williams Obsterics 23rd ,
- 21. Hydatidiform Mole Diagnosis: History Clinical examination Ultrasound examination Serum hCG levels Histopathological examination Cytogenetic and molecular biological examination
- 22. Hydatidiform Mole Diagnosis: Ultrasonography: * The diagnosis of molar pregnancy is nearly always made by ultrasonography Complete mole •The classical finding is a “snow storm" pattern •Theca lutein cysts are frequent findings on ultrasound
- 23. The snow storm appearance of complete hydatidiform mole
- 24. Theca lutein cysts, a frequent finding on ultrasound
- 25. Hydatidiform Mole Diagnosis: Ultrasonography: Partial mole Abnormal gestational sac The classic vesicular sonographic findings of a complete mole are usually not seen Focal sonographic cystic changes and/or hydropic changes in the placenta are significantly associated with the diagnosis of a partial molar pregnancy
- 26. Hydatidiform Mole Diagnosis: Ultrasonography: However, based on ultrasound, correct diagnosis can be suspected in only: • 84% of patients with complete mole and • 30% of patients with partial mole (Lindholm and Flam, 1999) The accuracy of ultrasonogrophy is gestational age dependent In comlete mole: • 100% of cases cane be diagnosed at a gestational age of 13 eeks or more • 50% of cases cane be diagnosed in earlier pregnancies (Lazarus et al, 1999)
- 27. Hydatidiform Mole Diagnosis: Serum hCG levels: Serum hCG levels of greater than 92 000 IU/l associated with absent fetal heart beat indicate a diagnosis of complete hydatidiform moles (Romero et al, 1985) Serum hCG level decreases quickly if the patient has an abortion, but it does not in molar pregnancy
- 28. Hydatidiform Mole Diagnosis: Histopathological examination: It should always be done as far as possible and samples should be kept for DNA analysis for a final diagnosis when histology can not differentiate molar pregnancy from abortion
- 29. Hydatidiform Mole Management: Complete history and physical examination Investigations Medical and surgical care 1 3 2
- 30. Hydatidiform Mole Management: History and physcal examination: Should aim to rule out the classic symptoms and signs that would lead to a diagnosis of: severe anemia dehydration preeclampsia thyrotoxicosis The patient should be stabilized hemodynamically
- 31. Hydatidiform Mole Management: Investigations: Laboratory: Pre-evacuation hCG Complete blood count Electrolytes, BUN, creatinine Liver function tests Thyroid function tests Imaging: Pelvic ultrasound Chest x-ray
- 32. Hydatidiform Mole Management: Medical care: Correction of: Anemia Dehydration Hyperthyroidism hypertension
- 33. Hydatidiform Mole Management: Surgical care: Suction curettage (with oxytocin or prostaglandin infusion) Hysterectomy •The method of choice •Increased risk of medical complications •Associated with a markedly decreased rate of malignant sequelae (3.5%) when compared with suction evacuation.
- 35. Persistent trophoblastic disease(GTN) In a proportion of patients (10%), trophoblastic disease persists, as evidenced by continuing clinical symptoms particularly vaginal bleeding and/or elevation of hCG levels, excessive uterine size and prominent theca lutein cysts. Because of routine registration and good follow-up , the great majority of patients requiring chemotherapy for persistent disease are recognized early. Unversity of slemani college of medicine lectures – department of gynecology
- 36. Defining persistent trophoblastic disease and Indications for initiating chemotherapy: 1-high, plateau or rising hCG level after evacuation. 2-persistent vaginal bleeding with raised hCG. 3-hCG > 20000IU/L more than 4 weeks after evacuation. 4- Histological evidence of choriocarcinoma. 5-pulmonary, vulval or vaginal metastases unless the hCG level is falling. 6-brain, liver, gastrointestinal metastases or lung metastases >2cm on chest radiography Unversity of slemani college of medicine lectures – department of gynecology
- 37. Hydatidiform Mole Complications associated with molar pregnacy: Those related to the increased trophoblastic tissue volume: Theca-lutein cysts Pregnancy-induced hypertension, hyperthyroidism, Respiratory distress Hyperemesis Those related to its management: Uterine perforation
- 38. Post-evacuation Surveillance Why? To determine when pregnancy can be allowed To detect persistent trophoblastic disease (i.e. GTN)
- 39. A baseline serum β -hCG level is obtained within 48 hours after evacuation. Levels are monitored every 1 to 2 weeks while still elevated to detect persistent trophoblastic disease (GTN). These levels should progressively fall to an undetectable level (<5 mu/ml). If symptoms are persistent, more frequent β hCG estimation and U/S examination ± D&C are advised RCOG Guideline No. 38 ; 2010 The Post-evacuation Surveillance. How?
- 40. Hydatidiform Mole Prognosis: Post-molar gestational trophoblastic disease: Risk: Following complete mole: 20% Following partial mole: 5% Type: 70% to 90% are persistent or invasive moles 10% to 30% are choriocarcinomas Subsequent fertility: Following chemotherapy, fertility is usually maintained and regular cycle restart 2-6 months after completion of treatment. Further pregnancy should be deferred for 12 month after treatment to avoid any teratogenic effect.
- 42. A malignant form of GTD which can develop from a hydatidiform mole or from placental trophoblast cells associated with a healthy fetus ,an abortion or an ectopic pregnancy.
- 43. Symptoms and signs Bleeding Infection Abdominal swelling Vaginal mass Lung symptoms Symptoms from other metastases
- 44. Doppler image of choriocarcinoma
- 45. FIGO staging: Stage I disease confined to uterus. Stage II outside uterus but limited to genital structures. Stage III extends to lung with or without genital tract involvement. Stage IV all other metastases. This disease ids highly chemo sensitive and surgery is indicated in small groups.
- 47. 1- International Journal of Gynecological Cancer, 14, 366- 369. (( http://dx.doi.org/10.1111/j.1048-891X.2004.014223.x )) 2- American Congress of Obstetricians and Gynecologists 3- American Cancer Society 4- Williams Gynecology, 2e Barbara L. Hoffman, John O. Schorge, Joseph I. Schaffer, Lisa M. Halvorson, Karen D. Bradshaw, F. Gary Cunningham, Lewis E. Calver 5- royal college of obstetricians and gynaecologists : Green–top Guideline No. 38 February 2010 6- Slideshare presentations plus medscape and some other websites 7- Case Scenario by XOM based on the above references 8- Kaplans vedio tutorial for USMLE 9- Unversity of slemani college of medicine lectures – department of gynecology References
- 49. If you Have questions Le Diktore bpirsn